Surgery, Gastroenterology and Oncology

|
|
Background and Aim: Acute Mesenteric Ischemia (AMI) is a serious vascular emergency with significant fatality and a jumping rate in covid-19 patients. This research investigated many of the cases diagnosed with COVID-19 that were identified with the diagnosis of AMI, and it presented the primary and secondary outcomes, including mortality, with their predictors.
Materials and Methods: The study was conducted at four centers managing COVID-19 patients diagnosed with AMI in two countries between March 1, 2020, and July 1, 2023.
Results: This study included 84 patients diagnosed with COVID-19 and mesenteric ischemia. The average age of the participants was 62.3±11.9 years, and nearly three-fourths (76.2%) were male. The most frequent presenting symptoms were fever, and deterioration of general condition, followed by dyspnea and diarrhea. Less than one-third of the participants (28.6%) had pulmonary thrombosis, and nearly half (47.6%) had mesenteric vessel thrombosis. Most participants had necrotic ischemia (95.2%) and underwent surgical intervention. The average severity score was 12.3±2.6. Three quarters of the participants required mechanical ventilation. Female sex, age ³ 60 years, high CT severity score, and mechanical ventilation deployment were significant independent variables in the prediction of mortality risk in multivariate models.
Conclusion: This study outlined the existing situation regarding outcomes, including the high mortality of AMI in COVID-19 patients. Female gender, age 60 years, high CT severity score, and mechanical ventilation deployment were significant independent in the prediction of mortality risk in multivariate models. The results provide an overview of mortality predictors, which would support further studies based on these findings.
INTRODUCTION
The WHO Health Organization has designated COVID-19 because of the new SARS-CoV-2 virus. It may have substantial systemic effects on important organs including the respiratory and digestive systems. Apart from respiratory symptoms, gastrointestinal symptoms such as diarrhea (3.8–10.1%), nausea (5–10.1%), vomiting (3.6–5%), and abdominal pain (2.2%) have also been documented as primary complaints (1-3).
A growing body of research indicates that COVID-19 patients frequently experience coagulopathy, and there have been reports of significant rates of thrombotic complications, the most common of which is venous thromboembolism (VTE) in patients admitted to intensive care units (ICUs) (4,5).
Acute mesenteric ischemia (AMI) is a serious vascular emergency with significant fatality rates between 50 and 70% despite ongoing advancements in diagnostic, interventional, and surgical procedures. Mesenteric ischemia occurs in 0.09–0.2% of the general population, but in COVID-19-affected patients, the prevalence increases to 1.9%–3.8%, with substantial rates of related morbidity and mortality (6-9).
AMI is separated into mesenteric ischemia with non-occlusive and occlusive causes. These conditions have an overall mortality rate of 50–80% and necessitate prompt diagnosis and treatment because of the patients' rapidly declining clinical condition (10,11).
This study aimed to assess the usefulness of risk assessment of mortality in expanding its applicability as a predictive tool for mortality risk among patients with AMI. Many cases diagnosed with covid-19 were identified with a proven diagnosis of AMI and were collected to study the primary (mortality and morbidity) and secondary outcomes including different patterns of AMI and predictors of mortality.
MATERIALS AND METHODS
Study Design and Setting
This study was in line with the STROCSS criteria (12). This study examined the registered medical data. This study, which is a retrospective observational study, was conducted at four centers caring for COVID-19 patients at teaching and university Hospitals between March 1, 2020, and July 1, 2023. Every center has a high volume and is an emergency surgery-focused facility. Surgeons with board certifications conducted every surgery. Data from the patient records of individuals who contracted COVID-19 and showed symptoms of mesenteric ischemia including those of both sexes and all age groups were gathered. This study was approved by the local ethics committee of the surgery department.
Inclusion Criteria
All consecutive patients with acute mesenteric ischemia who were diagnosed with COVID-19 and underwent surgery for necrotic ischemia between March 1, 2020, and July 1, 2023.
Exclusion Criteria
-
patients operated outside the study period;
-
patients with aortic dissection or isolated dissection of the SMA, as well as those with subsequent ischemia from ileus or adhesions;
-
patients who were not diagnosed with COVID-19.
Data Collection and Sorting
The following patient data were gathered: detailed recording of sex, age, blood transfusion history, pre-existing comorbidities, in-hospital mortality, hospital stay, BMI, clinical images, diagnostic tests, surgical management, and results. A prognostic scoring system to predict the severity of corona virus disease was implemented for all cases using demographic data, radiological and laboratory diagnostics (13). Every patient had their postoperative course monitored, and further morbidity and mortality were noted. All data were gathered onto a unique performance sheet and tabulated for statistical analysis.
Diagnostic Methods
Computed Tomography CT revealed lesions consistent with COVID-19, and a specific SARS-CoV-2 polymerase chain reaction (PCR) confirmed this. Swabs were taken from the nasopharynx. Following blood testing, arterial blood gas analysis, thoracic CT, interstitial pneumonia, and acute respiratory insufficiency were identified. Oxygen was prescribed initially. The SARS-CoV-2 test result of the naso-pharyngeal swab was positive. Doppler US and CT Angio. were performed to screen for the status of the abdominal vasculature.
Statistical Analysis
Data were analyzed using the SPSS statistical package version 26. Numerical data were summarized as means and standard deviations (SD), while qualitative data were described as frequencies and percentages. Relation between qualitative data was performed using the chi-square test or Fisher’s exact test. The relationship between numerical data was done using the Mann-Whitney test. We extracted the instrumental variables and performed bidirectional univariate and multivariate logistic regression analyses. Multivariate logistic regression was conducted to determine mortality predictors. Multivariate analyses were used to identify independent risk factors for mortality. A probability (p-value) equal to or less than 0.05 is considered significant. This analysis facilitated the formation of equitable groups with comparable baseline characteristics such as age, sex, underlying health conditions, and level of consciousness. This minimized the possibility of bias in the assessment of outcomes.
RESULT
This study included 84 patients diagnosed with COVID-19 and mesenteric ischemia. Table 1 presents the demographic characteristics and the clinical variables of the study population. The average age of the participants was 62.3±11.9 years, and three quarters (76.2%) were male. The most frequent presenting symptoms were fever, deterioration of general condition, dyspnoea, and diarrhea. All patients had abdominal tenderness and 81% had abdominal distension. The average respiratory rate was 24.9±3.8 and most patients had O2 Sat. % more than 95% (table 1).
Table 1 - Demographic and clinical characteristics of patients
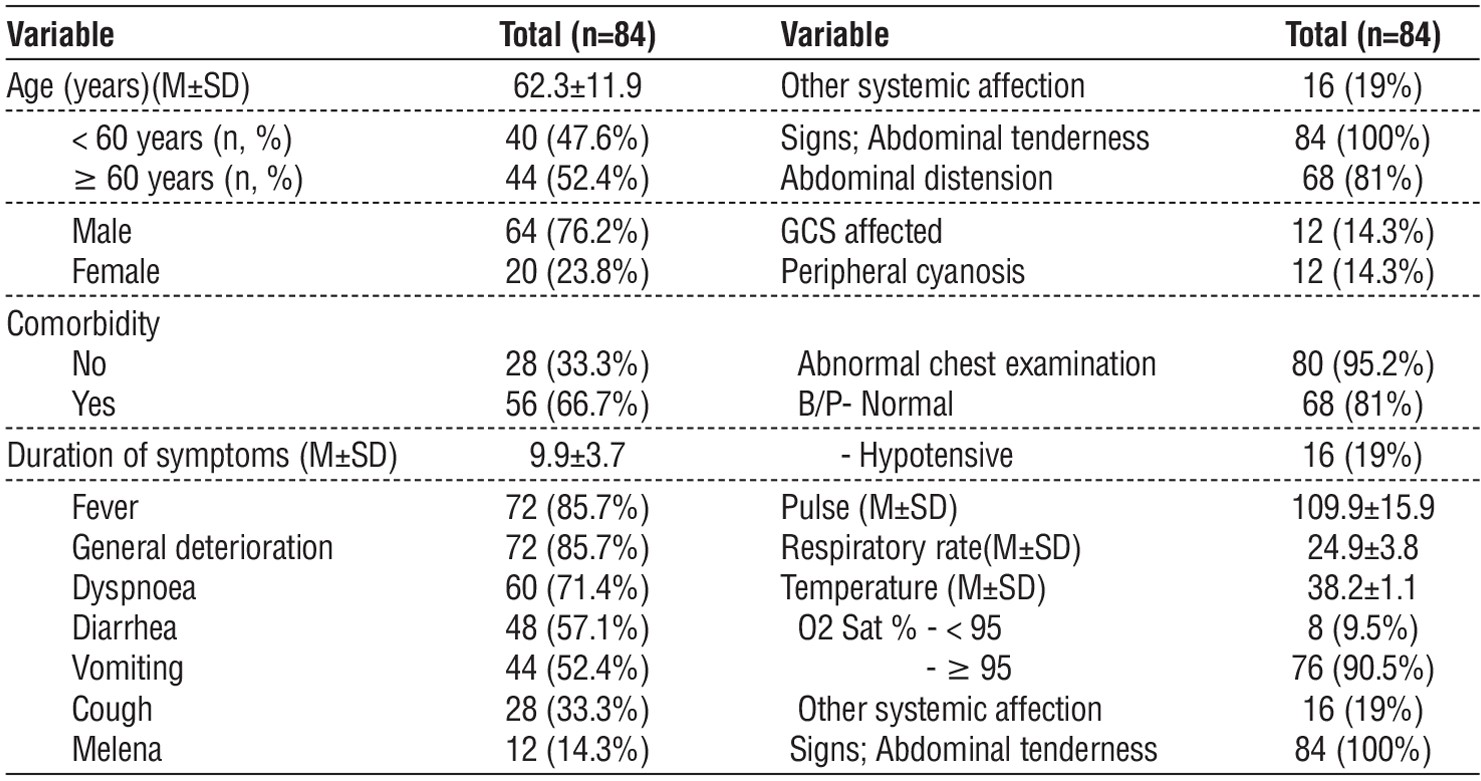
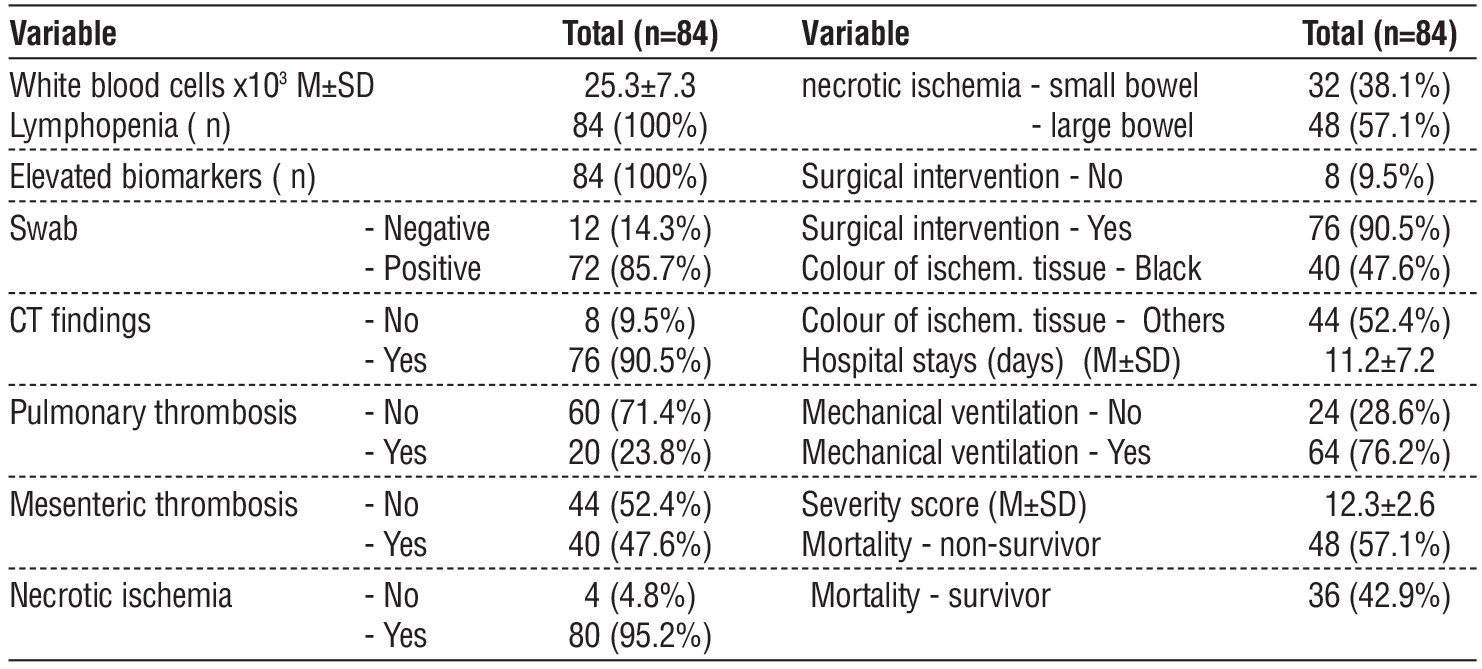
The average white blood cells was 25.3±7.3. All the participants had neutropenia and elevated levels of inflammation markers. Less than one-third of the participants (28.6%) had pulmonary thrombosis and half of the participants (47.6%) had mesenteric vessel thrombosis. Most participants had necrotic ischemia (95.2%) Most of them underwent surgical intervention. The average Hospital stay was 11.2±7.2 days, and the average Severity score was 12.3±2.6. Three-fourths of the participants needed mechanical ventilation (table 2).
Table 2 - Laboratory data and disease severity among the participants
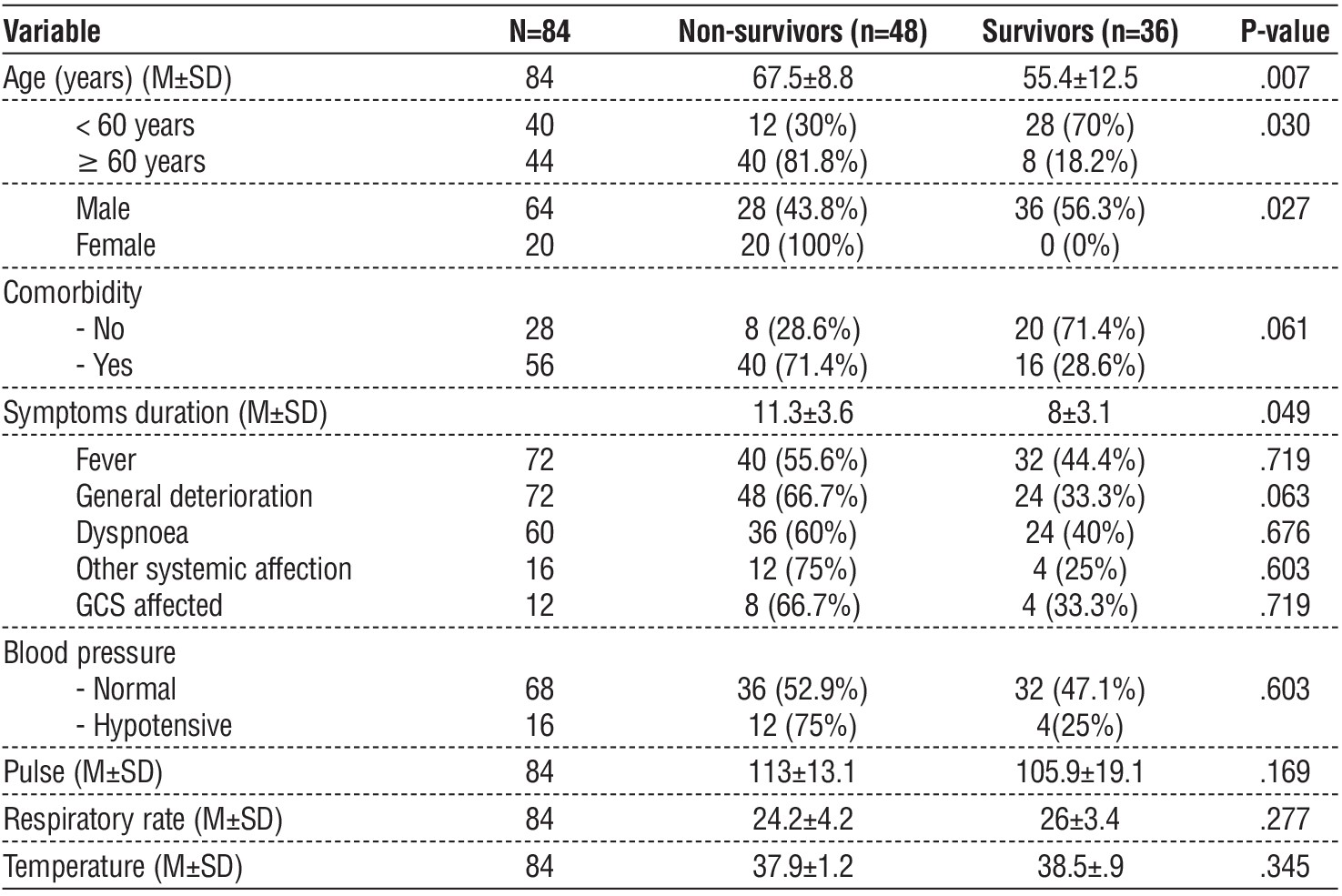
Non-survivors had significantly higher ages than survivor patients (67.5±8.8 years versus 55.4±12.5 years, p-value = .007). There was significantly higher mortality among females than among males (100% versus 43.8%, p-value=.027), and the duration of symptoms was significantly longer in the dead than among surviving patients (p-value-.049), there was no statistically significant relationship between clinical picture and mortality (table 3).
Table 3 - Univariate analysis of factors associated with mortality in patients.
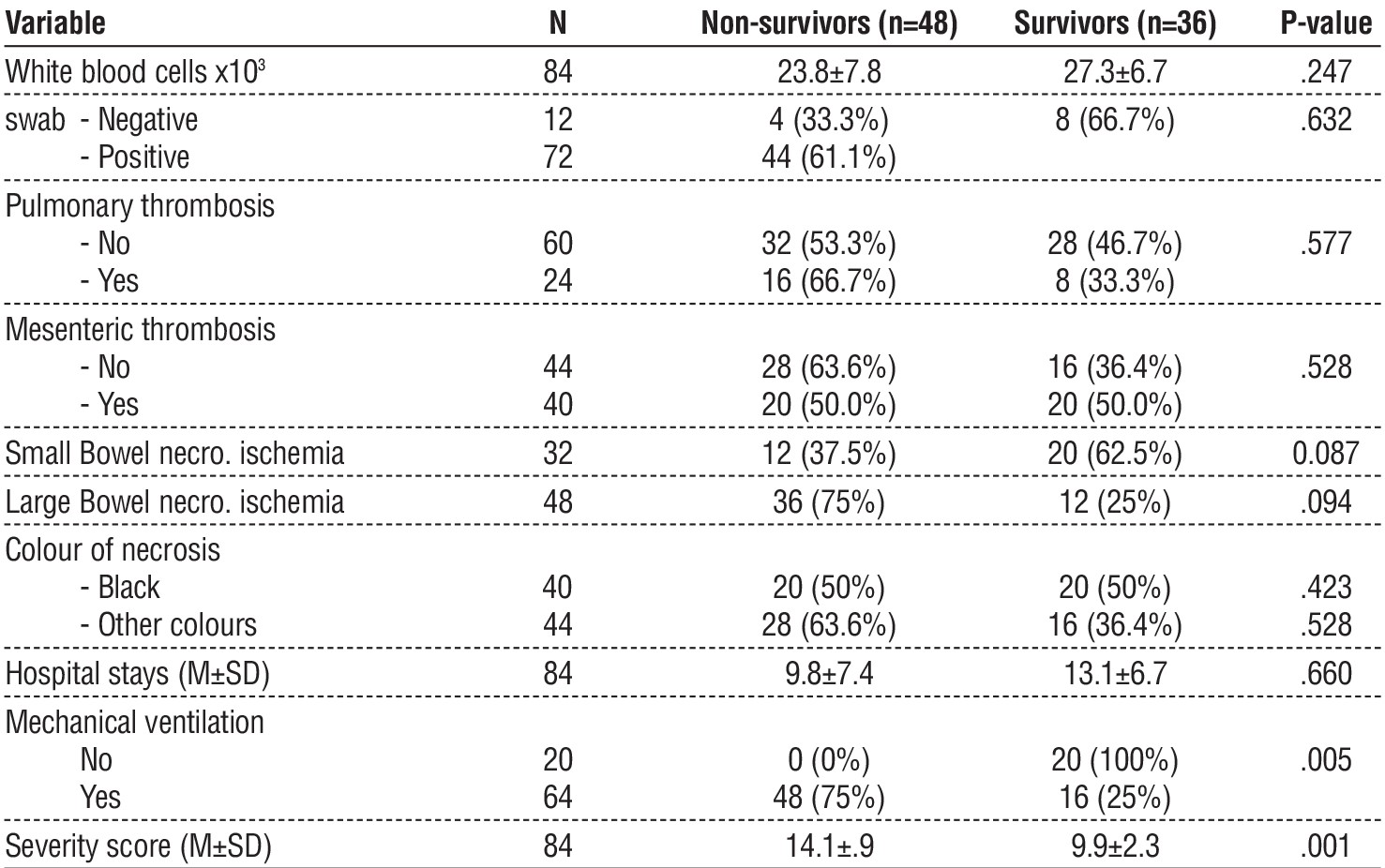
Most of the patients admitted to the ICU were placed on a mechanical ventilator and all patients were given heparin therapy. COVID-19 may predispose individuals to both venous and arterial thrombo-embolic diseases owing to excessive inflammation, hypoxemia, immobilization, and disseminated intra-vascular coagulation in severe cases. There was a significantly higher average severity score among dead than among survivor patients (14.1±.9 versus 9.9±2.3, p-value .001). patients who needed mechanical ventilation had significantly higher mortality than those who did not need mechanical ventilation (p-value =.005), however, there was no statistically significant relationship between white blood cells, pulmonary thrombosis, mesenteric vessel thrombosis, and mortality
(table 4).
Table 4 - univariate analysis of laboratory data, disease severity, and mortality
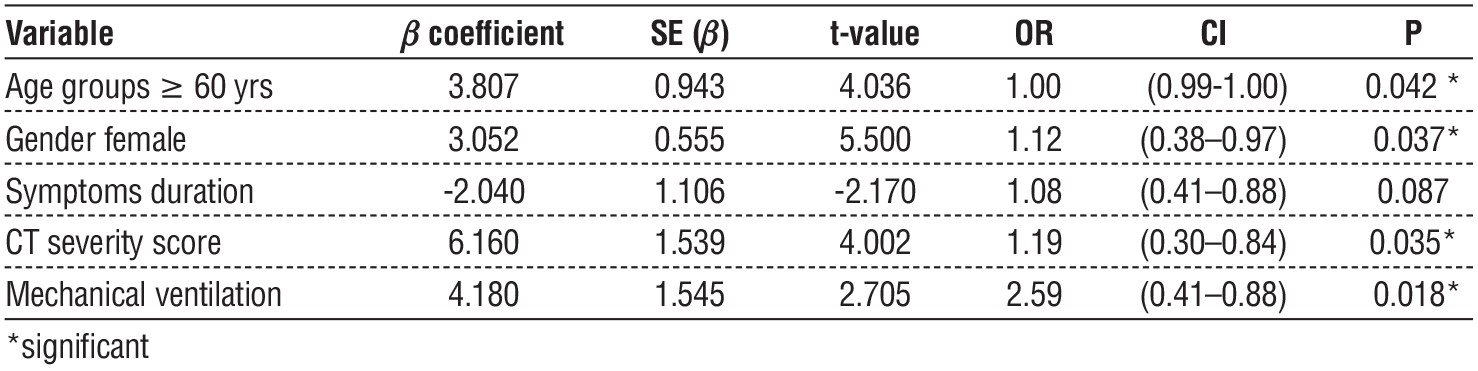
Most patients stayed at the hospital to recover, and the rest died, including all patients on mechanical ventilation. Statistically significant differences were observed in the measured epidemiological and peri-operative characteristics between the victims who lived and those who ceased living (table 5). In the multi-variate model, the female gender [P=0.037, 95% CI; 1.12 (0.38–0.97)], the age [P=0.024. 95% CI; 1 (0.99–01)], CT severity score [P=0.035, 95% CI; 1.19 (0.30–0.84)], and mechanical ventilation [P=0.018, 95% CI; 2,59 (0.44–0.89)] were significant independent variables in the prediction of mortality risk (table 5).
Table 5 - Multivariate analyses of Significant univariate factors associated with mortality.
DISCUSSION
AMI is a rare but extremely severe complication of SARS-CoV-2 infection in COVID-19 patients. It is a serious condition that occurs when the blood flow to the small intestine is restricted, leading to tissue damage and potential organ failure. COVID-19 can cause a hypercoagulable state leading to thrombotic complications in various systems. AMI is a rare complication of COVID-19, with a significant mortality rate. Demographic data play a crucial role in predicting and managing AMI as they provide valuable insights into the risk factors, disease progression, and outcomes associated with this condition (14).
In this study, many cases diagnosed with covid-19 were identified with a proven diagnosis of AMI and were collected to study the primary outcome (mortality and morbidity) and secondary outcomes, including different patterns of AMI and predictors of mortality. By examining demographic factors such as age, sex, and comorbidities, this study was conducted on 84 AMI COVID-19 patients, and it was found that females had higher mortality than males, and mortality in affected older patients was higher than that in younger patients. (67.5±8.8 years versus 55.4±12.5 years, p-value=.007). This finding was in line with the literature review given by Serban et al., where AMI with positive COVID-19 patients had a substantially worse prognosis when they were older; hospitalized individuals had a 54.4% mortality rate (14).
Several systemic conditions, such as arterial hypertension, atrial fibrillation, atherosclerosis, heart failure, and valve disease, are risk factors for AMI, as indicated by previous studies. Fever is less helpful in COVID-19 infected patients as they already might be taking antipyretic medicine (15). Hypotensive patients in this study represented 19% of the affected patients. Fever and deterioration of general condition were the most common presenting symptoms, followed by dyspnoea and diarrhoea. Noticeably, 81% of the patients experienced stomach distension, and all had abdominal discomfort.
A defining feature of Porto-mesenteric thrombosis, which is usually accompanied by fever and leuco-cytosis, is abdominal pain that is out of proportion to physical findings. All individuals experienced abdominal discomfort, which could be of high intensity, initially confined to the epigastric region, or generalized from the start. Pulmonary vein thrombosis occurs begin in the right hypochondrium, resembling biliary colic (16-18).
In our study and after the CT results, we found that nearly half of the individuals (47.6%) had mesenteric vascular thrombosis, while less than one-third (28.6%) had pulmonary thrombosis. Ischemia (embolism or thrombosis) may occur in the mesenteric arteries or veins. The manifestation of mesenteric ischemia and acute artery blockage of the small intestine can be attributed to hypercoagulability linked to SARS-CoV-2 infection, endothelial cell invasion through ACE-2 receptors, mucosal ischemia, and viral propagation (19). after all we find that there is no statistically significant correlation between mortality and symptoms or indications.
These, along with the laboratory findings that explained increasing leucocytosis in our population and elevated inflammatory biomarkers, were reviewed by Indian J Surg. Low-specificity fibrin breakdown products, such as D-dimer, and high lactic acid levels persist in severe COVID-19 patients without acute myocardial infarction. In contrast, biomarkers linked to hypercoagulable disorders help manage COVID-related thrombotic events and, to a lesser extent, help initiate preventive treatment. Increased indicators of inflammation and infection include procalcitonin, IL-6, C-reactive protein, and leukopenia (caused by cortico-steroid use). Other important markers included lactate dehydrogenase, ferritin, prothrombin time, and D-dimer levels. High mortality is correlated with elevated ferritin and lactate dehydrogenase levels (20).
Our analysis revealed that white blood cell counts, pulmonary thrombosis, mesenteric vascular thrombosis, and death were not significantly correlated. Approximately three-fourths of our participants required mechanical ventilation, and the mortality rate was very high among participants who were on mechanical ventilation. A systematic literature searched the need in mechanical ventilation for COVID-19 patients (13,21).
Regarding mortality predictors, we found that the prognosis of individuals with AMI was adversely affected by COVID-19 infection. There could be several reasons for this increased mortality, including systemic inflammation and the hypercoagulable state associated with COVID-19, which can exacerbate ischemic insult to the mesenteric vasculature. AMI is thought to account for 0.09–0.2% of all acute surgical admissions, although its frequency increases with age (13,21).
The COVID-19 individuals with AMI in our study also had identified mortality predictors. To account for confounders, we performed multivariable regression analyses adjusting for demographics, hospital-level characteristics, and relevant comorbidities in the multivariate model, the female gender, the age above 60 yr, high CT severity score, and mechanical ventilation deployment were significant independent variables in the term of prediction of the risk of mortality. Multi-variate analysis is a valuable prognostic tool of AMI in COVID-19 patients, providing a simple and rapid assessment method. Its high predictive accuracy supports its use in a broader patient population than in critically ill patients. Further studies are recommended to refine and validate the different predictors in diverse settings to enhance their clinical utility.
Limitations of the Study
This study has several limitations. First, the retrospective design may introduce selection bias and limit the ability to establish causality, as data accuracy and completeness depend on the quality of the recorded information in the registry. Second, the large discrepancy in the number of patients who survived versus those who died may introduce bias, reducing the study's statistical power and generalizability. Third, the study did not account for potential confounding factors such as variations in clinical practice, the existence of pre-hospital resuscitation, the execution of damage control surgery, the indication of transfusions, or the presence of other comorbidities, which could influence mortality outcomes. Although prospective studies are typically considered more robust, retrospective designs have their own strengths. This approach allows researchers to efficiently analyze large datasets and generate hypotheses for further investigation. Extensive analysis of multiple outcomes enables a more thorough evaluation of the illness load, related consequences, and a deeper understanding of how AMI affects COVID-19 patients. Therefore, a multidisciplinary approach based on early diagnosis and individualized treatment is essential for the effective management of AMI. We expect our study conclusions to be circulated to a larger population, many geographical locations, and various healthcare contexts to improve the external validity of our results. Large-scale prospective studies are required in the future to precisely identify the onset period and provide more detailed information on the primary and secondary outcomes.
CONCLUSION
This observational retrospective study showed the characteristics, outcomes, indications of mortality, and morbidity rates associated with AMI in COVID-19 patients. Female gender, age ≥ 60 years, high CT severity score, and mechanical ventilation deployment were significant independent variables for the prediction of the mortality risk. The results provided an overview of the primary and secondary outcomes, which would support additional studies based on these findings. These findings emphasize the importance of the early recognition and management of AMI in COVID-19 patients, especially in high-risk populations. This study simplifies the risk assessment of AMI in covid-19 patients but requires validation across diverse populations and settings for broader applicability.
Clinical Significance: This study showed the characteristics, outcomes, indications of mortality, and
morbidity rates associated with AMI in COVID-19 patients. This study helps in the prediction of mortality risk in patients of acute mesenteric ischemia of Covid-19 for better surgical implication and practice. The results provide an overview of mortality predictors, which would support further studies based on these findings.
Conflict of Interest: none
Sources of funding for research: none
Ethics Approval and Consent to Participate: available.
Availability of Data and Materials: available.
REFERENCES
-
Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020; 382(8):727–33.
-
Johns Hopkins University COVID-19 daily dashboard [cited 2020 Oct 22]. Available from: https://coronavirus.jhu.edu/map.html
-
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020; 323(11):1061-1069.
-
Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18(4):844-847.
-
Lodigiani C, Iapichino G, Carenzo L, Cecconi M, Ferrazzi P, Sebastian T, et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res. 2020;191:9-14.
-
Klar E, Rahmanian PB, Bücker A, Hauenstein K, Jauch KW, Luther B. Acute mesenteric ischemia: a vascular emergency. Dtsch Arztebl Int. 2012 Apr;109(14):249–56.
-
Romero MDCV, Cárdenas AM, Fuentes AB, Barragán AAS, Gómez DBS, Jiménez MT. Acute mesenteric arterial thrombosis in severe SARS-Co-2 patient A case report and literature review. Int J Surg Case Rep. 2021;86:106307–106307.
-
Chandrakar S, Sangadala P, Gupta M, Kumar DA, Agarwal A. Acute mesenteric ischemia in COVID-19 Case report and current understanding. Qatar Med J. 2022;2022(1):11–11.
-
Costa F, Nogueira L, Marques S, Torres L, Silva AF. An Improbable Thromboembolic Manifestation of COVID-19 A Case Report. Cureus. 2022;14(3):e23013.
-
Krothapalli N, Jacob J. A Rare Case of Acute Mesenteric Ischemia in the Setting of COVID-19 Infection. Cureus. 2021;13(3):e14174.
-
Kanasaki S, Furukawa A, Fumoto K, Hamanaka Y, Ota S, Hirose T. Acute Mesenteric Ischemia Multidetector CT Findings and Endovascular Management. Radiographics. 2018;38(3):945–961.
-
Mathew G, Agha R, Albrecht J, Goel P, Mukherjee I, Pai P, et al. STROCSS 2021: Strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int J Surg. 2021; 96:106165.
-
Emile SH, Khan SM. Predictors of severe and critical COVID-19: A systematic review. World J Clin Infect Dis. 2020;10(2):24-32.
-
Serban D, Tribus LC, Vancea G, Pantea Stoian A, Dascalu AM, Suceveanu AI, et al. Acute mesenteric ischemia in COVID-19 patients. J Clin Med. 2021;11(1):200.
-
Dumic I, Martin S, Salfiti N, Watson R, Alempijevic T. Deep Venous Thrombosis and Bilateral Pulmonary Embolism Revealing Silent Celiac Disease: Case Report and Review of the Literature. Case Rep Gastrointest Med. 2017;2017:5236918.
-
Radovanovic N, Dumic I, Veselinovic M, Burger S, Milovanovic T, Nordstrom CW, et al. Fusobacterium necrophorum subsp. necrophorum Liver Abscess with Pylephlebitis: An Abdominal Variant of Lemierre’s Syndrome. Case Rep Infect Dis. 2020; 2020: 9237267.
-
Abeysekera KW, Karteszi H, Clark A, Gordon FH. Spontaneous portomesenteric thrombosis in a non-cirrhotic patient with SARS-CoV-2 infection. BMJ Case Rep. 2020;13(12):e238906.
-
Randhawa J, Kaur J, Randhawa HS, Kaur S, Singh H. Thrombosis of the Portal Vein and Superior Mesenteric Vein in a Patient With Subclinical COVID-19 Infection. Cureus. 2021;13(4):e14366.
-
Yantiss RK, Qin L, He B, Crawford CV, Seshan S, Patel S, et al. Intestinal Abnormalities in Patients With SARS-CoV-2 Infection: Histopathologic Changes Reflect Mechanisms of Disease. Am J Surg Pathol. 2022;46(1):89-96.
-
Al Mahruqi G, Stephen E, Abdelhedy I, Al WahaibiK. Our early experience with mesenteric ischemia in COVID-19 positive patients. Ann Vasc Surg. 2021:73:129-132.
-
Kanugula AK, Kumar V, Gorle S, Maddika SR, Kaur J, Gaduputi V, et al. Outcomes of Acute Mesenteric Ischemia in Patients With COVID-19: A Nationwide Database Study. Cureus. 2023;15(7):e41444.
Full Text Sources:
Abstract:
Views: 2416

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.