Surgery, Gastroenterology and Oncology

|
|
Background: The early detection of colorectal anastomotic leakage (CAL) remains challenging despite advancements in diagnostic methods. Reliable markers are needed to reduce patient morbidity and mortality. Cytokines in drain fluid and systemic cytokine levels have shown potential as predictive markers for CAL, but more robust evidence is required. This systematic review and meta-analysis aimed to evaluate the importance of peritoneal and serum or plasma interleukin-6 (IL-6) levels in the early detection of CAL after colorectal surgery in colorectal cancer patients.
Methods: We conducted a comprehensive search in PubMed, Scopus, and Web of Science for relevant studies published before May 2023. Studies investigating plasma/serum, peritoneal IL-6 levels (or both) in CAL following colorectal surgery in colorectal cancer patients were included. Data on the mean and standard deviation of circulating and peritoneal IL-6 levels were extracted for CAL and non-CAL patients. Mean differences were analyzed for each postoperative day (POD) using OpenMeta [analyst].
Results: Sixteen articles were included in this meta-analysis, with 13 measuring peritoneal IL-6 levels and six measuring of circulating IL-6 levels. The systematic review included seven articles evaluating peritoneal IL-6 levels, revealing no significant elevation in CAL patients compared to non-CAL patients at any POD. Meta-analysis for circulating IL-6 levels was not feasible.
Conclusions: Based on the available evidence, peritoneal and serum or plasma IL-6 levels cannot be considered early markers for CAL following colorectal surgery in colorectal cancer patients. Further high-quality studies are necessary to determine whether IL-6 could be a reliable marker for anastomotic leakage after colorectal surgery.
INTRODUCTION
Despite significant advancements in surgical techniques, postoperative colorectal anastomotic leakage (CAL) continues to be a severe complication following colorectal surgery, leading to increased
morbidity and mortality (1). In addition, CAL is a prognostic factor linked to unfavorable outcomes in patients who undergo curative resection for colorectal cancer (2).
Currently, the detection of CAL depends on endoscopic examination, water-soluble contrast enema, and computed tomography (CT). CAL diagnosis remains challenging (3), despite the progress made regarding its detection. Many cases of CAL remain undetected until the advanced stages of this complication, resulting in high rates of dangerous reintervention. Consequently, early detection of CAL is crucial for reducing the mortality and morbidity of patients (4).
CAL involves a defect in the colorectal wall at the anastomotic site, causing communication between the intra- and extraluminal compartments. Localized inflammatory mediators, including cytokines present in drain fluid, have the potential to serve as predictive markers for anastomotic leakage (5). Furthermore, evaluating systemic levels of inflammatory mediators (6) and cytokines could aid CAL detection, although robust evidence is currently lacking (7).
Among the various cytokines, interleukin-6 (IL-6) has been extensively studied in CAL following colorectal surgery for colorectal cancer. Increased postoperative levels of IL-6 in both peritoneal fluid and serum or plasma may hold promise for early CAL detection. Indeed, two relatively recent meta-analyses have suggested that peritoneal IL-6 levels could be a diagnostic marker for CAL after colorectal surgery (8,9). However, while Qi et al. (9) applied a random-effects model in their data analysis and discussed the potential causes of high heterogeneity in their study, they did not present any data or figures that illustrated their sensitivity analysis conclusions. In addition, these systematic reviews and meta-analyses do not include all the studies available that provide information on circulating and peritoneal IL-6 levels. Furthermore, new related details have emerged. Therefore, we believe further exploration is necessary, considering the current literature and conducting a more rigorous analysis.
This systematic review and meta-analysis aimed to evaluate the significance of peritoneal and serum or plasma IL-6 cytokine levels in the early detection of CAL following colorectal surgery in colorectal cancer patients.
METHODS
Search strategies and eligibility of studies
This study follows the instructions of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (10). The following databases were evaluated: PubMed, Scopus, and Web of Science to recognize eligible studies published before May 2023, with no period restrictions. The following terms were searched in the title, abstract, and keywords to determine article eligibility: (‘colorectal’ OR ‘colorectal cancer’ OR ‘colorectal carcinoma’ OR ‘colorectal neoplasm’ OR ‘colorectal tumor’) AND (‘anastomotic leakage’ OR ‘anastomotic leak’ OR ‘anastomosis leakage’) AND (‘IL-6’ OR ‘IL6’ OR ‘interleukin 6’). Likewise, a manual search was conducted concerning articles included through the systematic search and Google Scholar database to capture eligible articles that the search strategy could not identify.
Inclusion and exclusion criteria
Peer-reviewed studies published in journals that met the following criteria were included: original research articles written in English investigating plasma or serum levels of plasma or serum, peritoneal IL-6 (or both) in CAL following the postoperative days (POD) of colorectal cancer surgery in humans and a control group was included for comparison purposes. Articles written in other languages, reviews, brief reports, books, comments, erratum texts, editorials, guidelines, letters, meeting reports, preprint manuscripts, theses, articles warning an expression of concern and retracted articles, non-human studies, studies assessing IL-6 in CAL but testing a product/compound for therapy aims, or studies that did not study serum or plasma or peritoneal samples, were excluded.
Study selection
Two researchers independently selected the articles. Relevant articles were detected based on titles and abstracts. Article sections were inspected, and eligible articles were compiled for inclusion in the review. Conflicts were resolved through discussion with a third author.
Quality assessment of included studies
The quality and risk of bias of the included studies were assessed using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) (11). Two researchers independently evaluated the articles. Conflicts were resolved through discussion with a third author.
Data extraction
Title, authors, year of publication, country of origin, study design, definition of CAL, name of configured groups, sample size, percentage of patients with CAL, type of sample, method, and results for IL-6 measurement were the data extracted from the analyzed articles.
Statistical analysis
The primary outcome was CAL and the mean and SD of peritoneal, circulating IL-6 levels (ng/mL), or both. IL-6 data from studies by Matthiessen et al. (12) and Yamamoto et al. (13) were obtained from Sparreboom et al. (8). We also considered the presence of skewed data. Therefore, in cases where mean values were not available, we utilized the median, Q1, and Q3 values, specifically in Sparreboom et al. (14) and Oikonomakis et al. (15). We then employed the quantile estimation (QE) method described by McGrath et al. (16) (https:// smcgrath.shinyapps.io/estmeansd/) to estimate the mean and SD, as it accounts explicitly for skewed data.
A meta-analysis was performed for each POD to compare the differences between patients with and without CAL. Quantitative statistical analysis was conducted using mean differences with a 95% confidence interval. The I² statistic, which represents the percentage of the total variation in the study estimates due to heterogeneity, was evaluated using Cochran’s chi-squared test. A random-effects model was used when I² > 50%, indicating high heterogeneity. Therandom-effects approach of DerSimonian and Laird was used to obtain a combined estimate and a 95% confidence interval (CI) for the ratio (17). A leave-one-out sensitivity analysis was performed to assess the influence of each study on the overall effect size and heterogeneity. Statistical analyses were performed using OpenMeta [analyst] (18).
RESULTS
Literature search and selection
The flowchart illustrating the literature search process is presented in fig. 1. Sixteen studies were included in the review according to predefined search criteria (12-15, 19-30). The general characteristics of each study are shown in table 1. All eligible studies were published between 2002 and 2022. Of the 16 studies, 13 were prospective (12-14,19-23,25,26,28-30), while three used a case-control design (15,24,27).
Figure 1 - PRISMA flow diagram

Table 1 - Characteristics of included studies
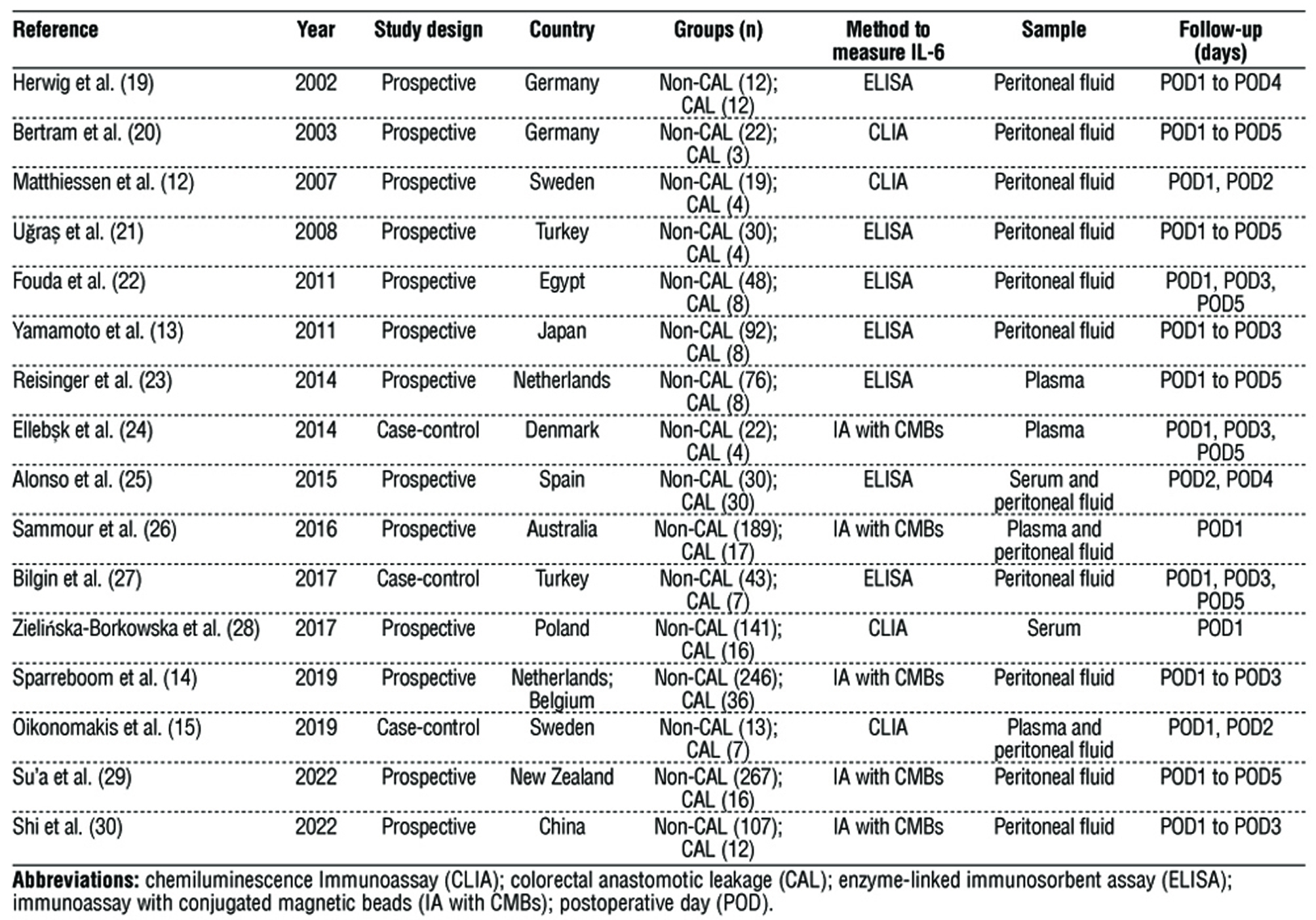
ELISA was the preferred method for assessing the peritoneal and circulating IL-6 levels. Ten studies specifically focused on determining peritoneal IL-6 levels, while three measured IL-6 levels only in plasma or serum (23,24,28). Three studies assessed both circulating and peritoneal IL-6 levels (15,25,26).
The enrollment across the 16 studies encompassed 1,549 participants, with 192 individuals having CAL and 1,357 individuals serving as control subjects. Peritoneal IL-6 levels were measured in 164 CAL patients and 1118 non-CAL subjects, whereas serum or plasma IL-6 levels were determined in 82 CAL patients and 471 non-CAL subjects. Finally, the preferred POD for investigating the outcome was POD1, with 15 studies examining IL-6 levels.
Definitions of colorectal anastomotic leakage
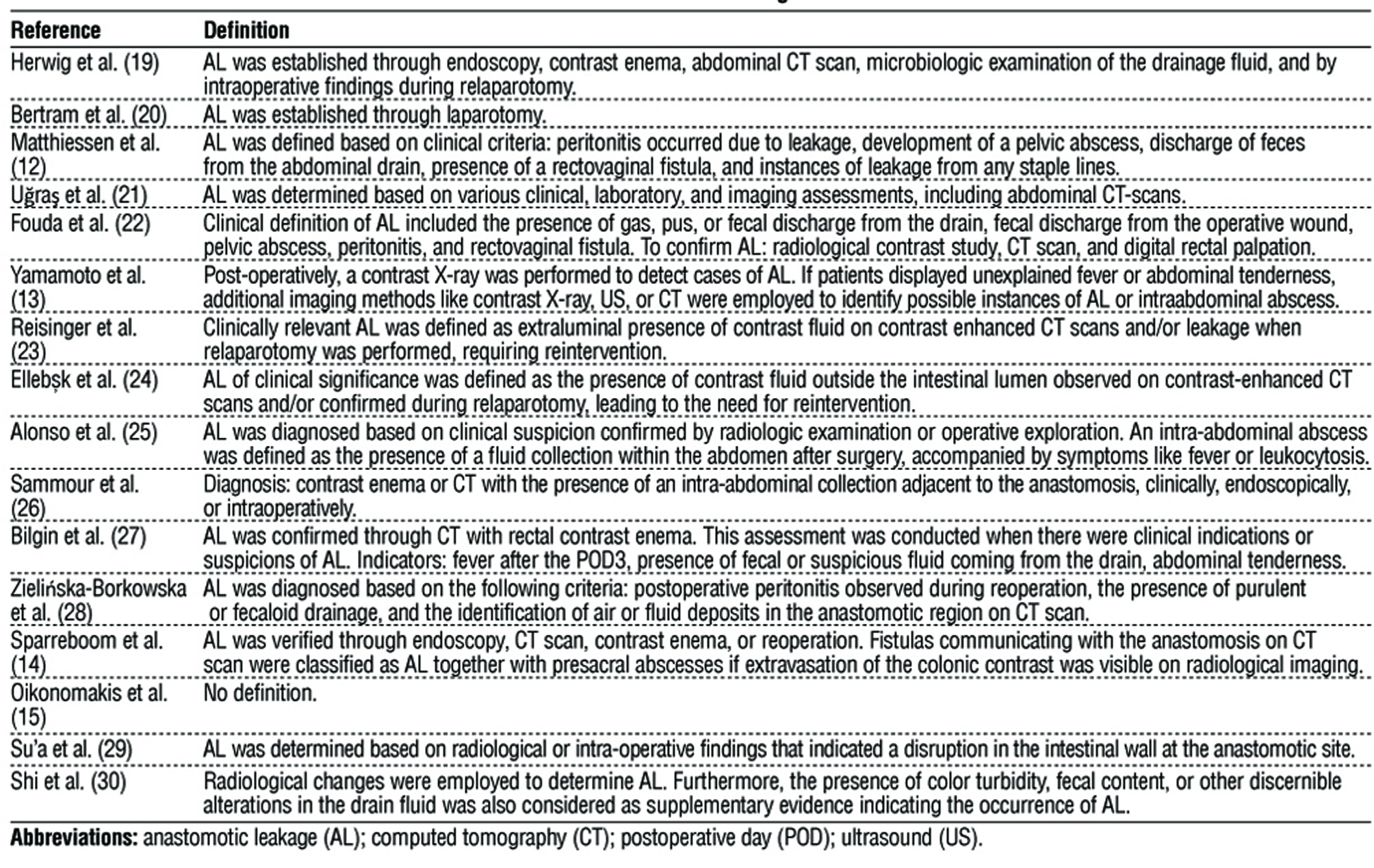
In the studies, the definitions of CAL varied (table 2). Most studies primarily relied on clinical signs but also incorporated imaging methods. All studies, except for Oikonomakis et al. (15), defined CAL. Several studies, including Herwig et al. (19), U?ra? et al. (21), Fouda et al. (22), Yamamoto et al. (13), Reisinger et al. (23), Ellebæk et al. (24), Alonso et al. (25), Sammour et al. (26), Bilgin et al. (27), Zieli?ska-Borkowska et al. (28), Sparreboom et al. (14), and Su’a et al. (29), involved imaging techniques such as contrast X-ray or CT scan in their definition for CAL. Additionally, Herwig et al. (19), Reisinger et al. (23), Ellebæk et al. (24), and Zieli?ska-Borkowska et al. (28) also incorporated the requirement of reintervention in their definition. These findings highlight the importance of consensus among research groups in defining CAL in patients. This consensus will improve the standardization of assessment methods and the management of these events, enabling meaningful comparisons between studies.
Table 2 - Definition of anastomotic leakage of included studies
Risk of bias assessment
The evaluation results indicated that several of the included studies were found to have a considerable risk of bias in patient selection, as confirmed by the assessment of applicability (table 3).
Table 3 - Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2)

The reported results of interleukin-6 in the studies
The results of studies examining IL-6 levels are summarized in table 4. Overall, while only a limited number of studies have investigated IL-6 levels in serum or plasma, and inconsistent findings have been reported, there was no significant difference in serum or plasma IL-6 levels between CAL and non-CAL patients. However, there is substantial evidence regarding peritoneal IL-6. Several authors, including Herwig et al. (19), Matthiessen et al. (12), U?ra? et al. (21), Fouda et al. (22), Alonso et al. (25), Sammour et al. (26), Oikonomakis et al. (15), and Su’a et al. (29), have reported increased levels of peritoneal IL-6 in CAL patients. In fact, out of the 13 studies measuring peritoneal IL-6 included in this systematic review, eight found a significant increase in peritoneal IL-6 levels in CAL patients compared to non-CAL patients.
Table 4 - The reported resultsof Interleukin-6 in the studies

Meta-analysis of IL-6 levels
The systematic review did not include certain studies in the quantitative statistical analysis. Specifically, the study of U?ra? et al. (21) reported peritoneal IL-6 levels that were 10 to 1,000 times higher than the results of other studies. Alonso et al. (25), Bilgin et al. (27), and Shi et al. (30) reported peritoneal IL-6 levels 10 to 1,000 times lower than the results of other studies. Sammour et al. (26) and Su’a et al. (29) presented their results only in terms of the median and interquartile range (IQR). Although there are methods for estimating the mean and SD from median and IQR, they mostly assume a normal distribution, which is not in line with the purpose of the present meta-analysis.
In the studies of Sparreboom et al. (14) and Oikonomakis et al. (15), the median, Q1, and Q3 were reported for their IL-6 results. Therefore, a recently reported robust method described by McGrath et al. (16) was used to estimate the mean and SD. McGrath et al. confirmed that meta-analysis was best performed when applying their methods for determining the mean compared to previously proposed methods (16).
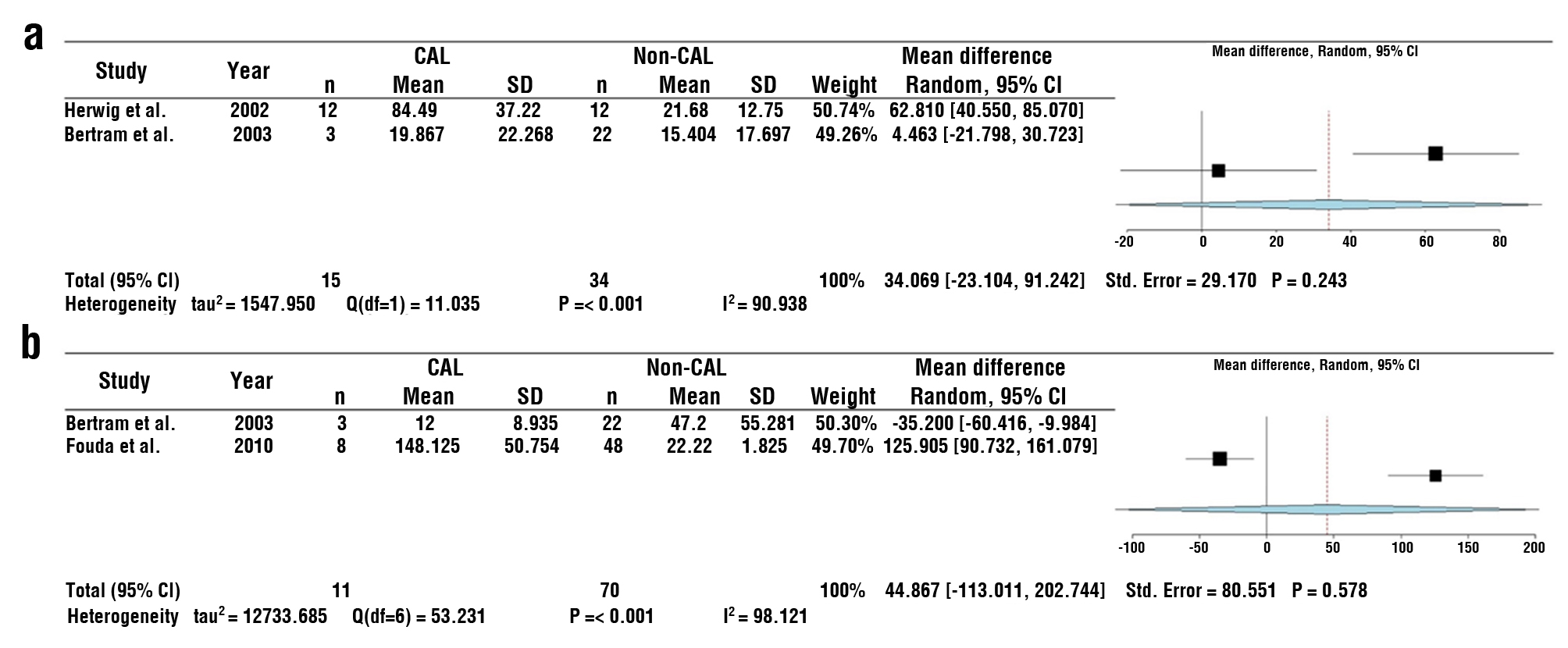
For the statistical analysis, we initially started with seven studies for POD1, which was reduced to six studies for POD2. We ultimately included five studies on POD3 in the meta-analysis examining peritoneal levels of IL-6 (fig. 2). Although only two studies considered POD4 (19,20) and POD5 (20,22) for IL-6 measurement, we performed the analysis following the approach of previously reported meta-analyses (8,9). Therefore, the results should be interpreted cautiously (Supplementary fig. 1).
Figure 2 - Forest plot of the mean difference of peritoneal levels of IL-6 (ng/mL) on CAL patients and non-CAL patients for postoperative days (POD) 1 (A), 2 (B), and 3 (C). Abbreviations: colorectal anastomotic leakage (CAL)
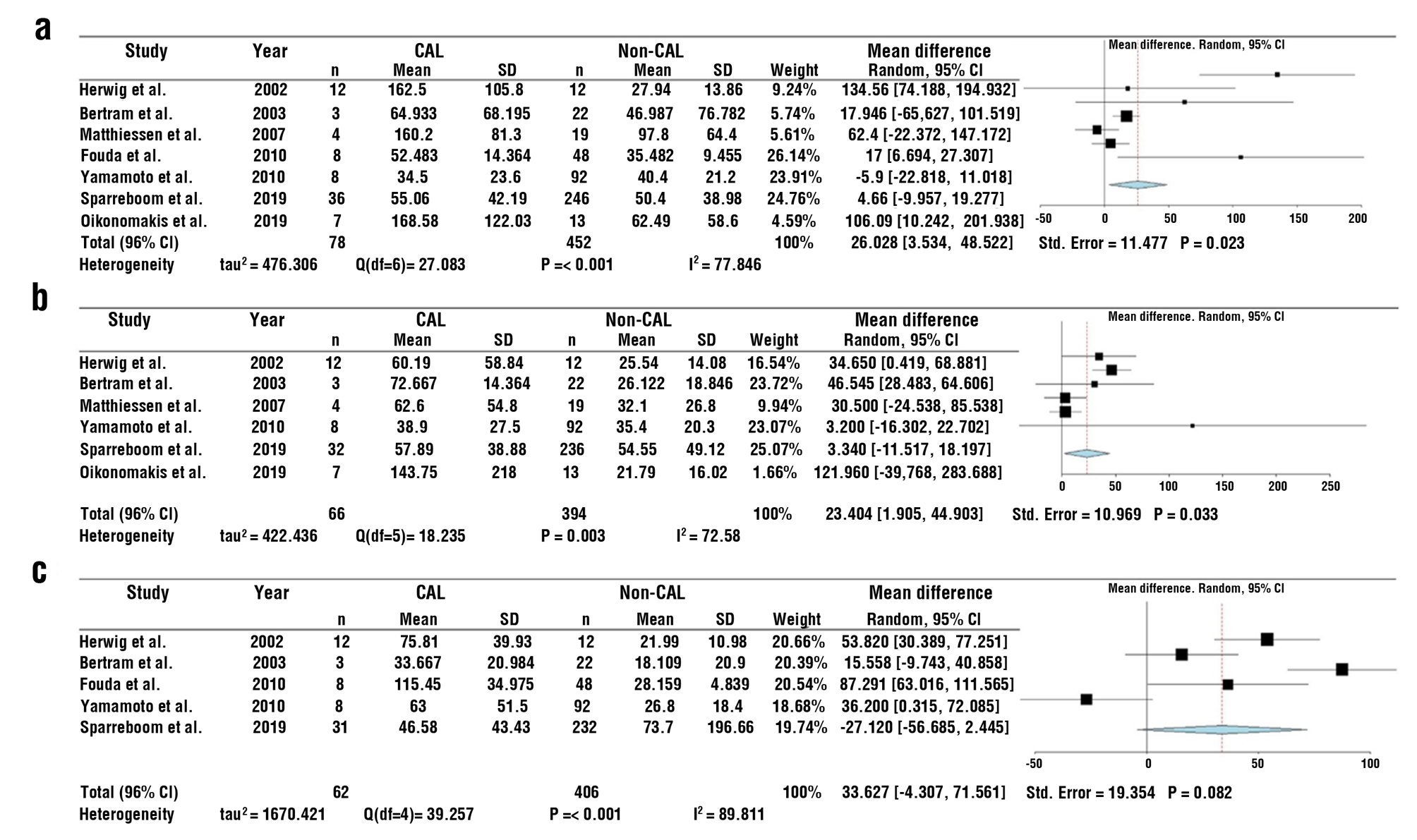
Figure S1 - Forest plot of the mean difference of peritoneal IL-6 (ng/mL) on CAL patients and non-CAL patients for postoperative days (POD) 4 (a) and 5 (b). Abbreviations: colorectal anastomotic leakage (CAL)
The combined data from the included studies revealed that peritoneal IL-6 levels were increased in CAL patients on POD1 (mean difference: 26.028, 95% CI: 3.534–48.522, P=0.023) and POD2 (mean difference: 23.404, 95% CI: 1.905–44.903, P=0.033). No significant difference was found between CAL and non-CAL patients on POD3 (P=0.082), POD4 (P=0.243), and POD5 (P=0.578).
Since we expected high heterogeneity, a leave-one-out sensitivity analysis was performed to confirm the conclusions. For POD1, the analysis revealed that the studies by Herwig et al. (19) and Oikonomakis et al. (15) were the main drivers of the results. The pooled data on peritoneal IL-6 levels were no longer different between CAL and non-CAL patients (fig. 3a) when each of these studies was removed separately. Furthermore, for POD2, when the studies of Herwig et al. (19), Bertram et al. (20), and Matthiessen et al. (12) were removed separately, the IL-6 levels between CAL and non-CAL patients were no longer different (fig. 3b). In POD3, the results remained consistent, as seen in fig. 2 (fig. 3c).
Figure 3 - Sensitivity analysis using the leave-one out method

DISCUSSION
Anastomotic leakage is a current problem that affects patients following colorectal surgery (1). This is related to increased costs (31), more extended hospital stays (32), and decreased health-related quality of life (33). CAL is linked to poor oncologic prognosis in colorectal cancer patients, including reduced disease-free survival (34) and cancer-specific survival (2).
Currently, many cases of CAL are not diagnosed until they reach an advanced stage (4,35). Therefore, research focusing on predictive markers for CAL is necessary. In this study, we aimed to determine whether peritoneal and serum or plasma IL-6 cytokine levels could serve as reliable markers for the early detection of CAL following colorectal surgery.
The studies did not consistently demonstrate a significant difference in circulating IL-6 levels between CAL and non-CAL patients. However, only six articles were found in the literature aiming to measure systemic cytokine levels, and out of those, five measured IL-6 levels in circulation on POD1 (table 1). Specifically, POD1 was the only postoperative day assessed more than three times. Among the five studies, three found increased systemic IL-6 levels of POD1 in patients who later experienced anastomotic leakage compared to non-CAL patients (15,24,26). Therefore, based on our results, we conclude that the literature lacks studies assessing IL-6 levels in circulation and POD1. More studies are needed to corroborate the potential role of POD1 IL-6 cytokine levels in circulation as markers in patients following colorectal surgery.
Since it has been stated that peritoneal IL-6 levels are more reliable markers of CAL compared to IL-6 measured in serum or plasma (8), we expected to find significant differences in the levels of peritoneal IL-6 when comparing pooled data. Based on the data reported to date, there is no apparent difference in the peritoneal levels of IL-6 between patients with CAL and non-CAL when the data is subjected to sensitivity analysis. This suggests that IL-6 levels cannot be considered markers of CAL following colorectal surgery.
The previous conclusion contradicts a recent meta-analysis conducted by Qi et al. (9). Our study did not observe significant differences in peritoneal IL-6 levels between CAL and non-CAL patients. However, Qi et al. reported that IL-6 levels were increased in the peritoneal fluids of CAL patients. Before conducting their meta-analysis, Qi et al. utilized the method developed by Hozo et al. (36) to estimate the mean when necessary (9).
Although the method by Hozo et al. is widely used for estimating the mean and SD, McGrath et al. recently developed a potentially more accurate method, as supported by their comparisons (16). McGrath et al.’s method considers the skewed nature of the data. They noted that a primary limitation is that they often assume a normal distribution for the outcome variable, although some formula-based methods effectively estimate the mean and SD. McGrath et al. found that the mean performed better when dealing with nonparametric variables. This highlights the potential advantages of using McGrath et al.’s method in estimating the mean and SD for skewed data (16).
It is common to find studies that report the median and other quantiles when the data are skewed. In our review, Sparreboom et al. (14) and Oikonomakis et al. (15) were examples of studies in which the authors reported the median, Q1, and Q3. In their meta-analysis, Qi et al. utilized Hozo et al.’s method to estimate the mean and SD for these particular studies (9).
Upon reviewing the estimation of the mean and SD in these studies, we observed an issue with the estimated SD for Oikonomakis et al. (15). The data reported in fig. 4A of the study by Qi et al. showed an estimated SD of 11.74 (9), which appeared unrealistically optimistic. The original data reported by Oikonomakis et al. for POD1 IL-6 levels were 165 ng/mL for the median, with Q1 and Q3 values of 60.7 ng/mL and 219.25 ng/mL, respectively (15). These data seem unlikely to produce a well-fitted estimated SD, as reported by Qi et al. (9).
The same example is also applicable when discussing the estimation of the mean for POD1 IL-6 levels using the median and other quantiles from Sparreboom et al. (14). This can be observed in fig. 4A of Qi et al.’s study (9) and table 2 in Sparreboom et al.’s study (14). The earlier explanations also apply to estimating the mean and SD for POD2 and POD3.
Our statistical analysis employed the same random-effects approach as Qi et al. (9), which involved the DerSimonian and Laird assessments (17). As Qi et al. did not specifically mention the DerSimonian and Laird evaluations, we conducted this test using their provided data to confirm their results. Then, using our data, we initially observed that peritoneal IL-6 levels on POD1 and POD2 were elevated in subjects who experienced CAL compared to those who did not (fig. 2). However, upon conducting sensitivity analyses using a leave-one-out approach, we discovered that the significance of the results was no longer attained (fig. 3). This is consistent with a recent meta-analysis evaluating the levels of different peritoneal cytokines, including IL-6, in POD1. Reeves et al. found that only IL-10 was significantly increased in CAL patients with POD1 (37).
IL-6 is a cytokine that plays a leading role in diverse host defense mechanisms, such as immune response and acute-phase reactions (38). Therefore, it is implicated in responding to many inflammatory conditions, including AL (8). Indeed, an experimental study conducted by Hintz et al. on rats indicated that systemic IL-6 had detrimental effects on the healing process of colonic anastomoses (39). It is worth highlighting that IL-6 exhibits dual roles, acting not only as a well-known pro-inflammatory molecule but also as an anti-inflammatory agent. Consequently, Zubaidi et al. reported that sustained elevation of IL-6 up to POD5 in the colon and small intestine may likely contributed to faster wound healing in anastomotic lesions in rats (40). Notably, IL-6 is also a major cytokine in the tumor microenvironment and is known to be deregulated in cancer (41). It is overexpressed in almost all kinds of tumors, including colorectal cancer (42). Therefore, the role of IL-6 levels in inflammatory and wound-healing processes in cancer conditions may be related to the pathogenesis, resolution, and prognosis of CAL.
As previously mentioned, significant progress has been made in this field of research. However, further investigation is imperative due to several limitations observed in included studies, which may explain the lack of significance in comparing IL-6 levels between patients. First, consistent with the findings of Qi et al. (9) and Sparreboom et al. (8), the low incidence rate of CAL following colorectal surgery poses challenges in conducting high-level evidence studies. Second, the variations in diagnostic criteria for CAL utilized across the included studies further undermine the reliability of the results. Third, considering the well-documented over-expression of IL-6 in colorectal cancer, discerning differences in IL-6 levels becomes challenging when studying patient groups already exhibiting elevated baseline levels. Consequently, more rigorous selection criteria, improved laboratory methods, and refined statistical approaches are warranted.
This review has some limitations. Namely, the limited number of available studies restricts the ability to perform subgroup analysis. Additionally, including a small number of CAL patients in each study decreased the precision of the obtained estimates. Finally, it is essential to acknowledge that the meta-analysis estimates are influenced by the chosen statistical methods, which can vary, including those used to estimate the mean and standard deviation.
CONCLUSIONS
Until now, peritoneal and serum or plasma IL-6 levels cannot be considered early markers of CAL following colorectal surgery in colorectal cancer patients. Further high-level evidence studies are needed to determine whether IL-6 could serve as a marker for CAL after colorectal surgery.
Acknowledgements
The authors thank the Instituto Mexicano del Seguro Social (IMSS) for providing facilities and software support for this research. Lucia is grateful for the infinite and selfless support she has received from Guillermina Coronado and Luis Villegas.
Conflict of interest
None.
Funding
None.
REFERENCES
1.Weber MC, Berlet M, Stoess C, Reischl S, Wilhelm D, Friess H, et al. A nationwide population-based study on the clinical and economic burden of anastomotic leakage in colorectal surgery. Langenbecks Arch Surg. 2023;408(1):55.
2.Takahashi H, Haraguchi N, Nishimura J, Hata T, Yamamoto H, Matsuda C, et al. The Severity of Anastomotic Leakage May Negatively Impact the Long-term Prognosis of Colorectal Cancer. Anticancer Res. 2018;38(1):533-9.
3.Chierici A, Granieri S, Frontali A. Diagnostic accuracy of water-soluble contrast enema, contrast-enema computed tomography and endoscopy in detecting anastomotic leakage after (Colo) proctectomy: A meta-analysis. Colorectal Dis. 2023. Epub 2023 Jun 1.
4.Chiarello MM, Fransvea P, Cariati M, Adams NJ, Bianchi V, Brisinda G. Anastomotic leakage in colorectal cancer surgery. Surg Oncol. 2022;40:101708.
5.Gray M, Marland JRK, Murray AF, Argyle DJ, Potter MA. Predictive and Diagnostic Biomarkers of Anastomotic Leakage: A Precision Medicine Approach for Colorectal Cancer Patients. J Pers Med. 2021;11(6):471.
6. Rama N, Lages M, Silva C, Lima P, Gil I, Guarino M, et al. The Usefulness of Inflammatory Biomarkers to Predict Anastomotic Leakage after Colorectal Surgery: Systematic Review and Meta-Analysis. Surg Gastroenterol Oncol. 2022;27:169.
7.Su'a B, Tutone S, MacFater W, Barazanchi A, Xia W, Zeng I, et al. Diagnostic accuracy of procalcitonin for the early diagnosis of anastomotic leakage after colorectal surgery: a meta-analysis. ANZ J Surg. 2020;90(5):675-80.
8.Sparreboom CL, Wu Z, Dereci A, Boersema GS, Menon AG, Ji J, et al. Cytokines as Early Markers of Colorectal Anastomotic Leakage: A Systematic Review and Meta-Analysis. Gastroenterol Res Pract. 2016;2016:3786418.
9.Qi XY, Liu MX, Xu K, Gao P, Tan F, Yao ZD, et al. Peritoneal Cytokines as Early Biomarkers of Colorectal Anastomotic Leakage Following Surgery for Colorectal Cancer: A Meta-Analysis. Front Oncol. 2021; 11:791462.
10.Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160.
11.Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-36.
12.Matthiessen P, Strand I, Jansson K, Tornquist C, Andersson M, Rutegard J, et al. Is early detection of anastomotic leakage possible by intraperitoneal microdialysis and intraperitoneal cytokines after anterior resection of the rectum for cancer? Dis Colon Rectum. 2007;50(11):1918-27.
13.Yamamoto T, Umegae S, Matsumoto K, Saniabadi AR. Peritoneal cytokines as early markers of peritonitis following surgery for colorectal carcinoma: a prospective study. Cytokine. 2011;53(2): 239-42.
14.Sparreboom CL, Komen N, Rizopoulos D, Verhaar AP, Dik WA, Wu Z, et al. A multicentre cohort study of serum and peritoneal biomarkers to predict anastomotic leakage after rectal cancer resection. Colorectal Dis. 2020;22(1):36-45.
15.Oikonomakis I, Jansson D, Horer TM, Skoog P, Nilsson KF, Jansson K. Results of postoperative microdialysis intraperitoneal and at the anastomosis in patients developing anastomotic leakage after rectal cancer surgery. Scand J Gastroenterol. 2019;54(10):1261-8.
16.McGrath S, Zhao X, Steele R, Thombs BD, Benedetti A, Collaboration DESD. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat Methods Med Res. 2020;29(9):2520-37.
17.DerSimonian R, Laird N. Meta-analysis in clinical trials revisited. Contemp Clin Trials. 2015;45(Pt A):139-45.
18.Wallace BC, Dahabreh IJ, Trikalinos TA, Lau J, Trow P, Schmid CH. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J Stat Softw. 2012;49(5):1-15.
19.Herwig R, Glodny B, Kuhle C, Schluter B, Brinkmann OA, Strasser H, et al. Early identification of peritonitis by peritoneal cytokine measurement. Dis Colon Rectum. 2002;45(4):514-21.
20.Bertram P, Junge K, Schachtrupp A, Gotze C, Kunz D, Schumpelick V. Peritoneal release of TNFalpha and IL-6 after elective colorectal surgery and anastomotic leakage. J Invest Surg. 2003;16(2):65-9.
21.Ugras B, Giris M, Erbil Y, Gokpinar M, Citlak G, Issever H, et al. Early prediction of anastomotic leakage after colorectal surgery by measuring peritoneal cytokines: prospective study. Int J Surg. 2008; 6(1):28-35.
22.Fouda E, El Nakeeb A, Magdy A, Hammad EA, Othman G, Farid M. Early detection of anastomotic leakage after elective low anterior resection. J Gastrointest Surg. 2011;15(1):137-44.
23.Reisinger KW, Poeze M, Hulsewe KW, van Acker BA, van Bijnen AA, Hoofwijk AG, et al. Accurate prediction of anastomotic leakage after colorectal surgery using plasma markers for intestinal damage and inflammation. J Am Coll Surg. 2014;219(4):744-51.
24.Ellebaek MB, Baatrup G, Gjedsted J, Fristrup C, Qvist N. Cytokine response in peripheral blood indicates different pathophysiological mechanisms behind anastomotic leakage after low anterior resection: a pilot study. Tech Coloproctol. 2014;18(11):1067-74.
25.Alonso S, Pascual M, Salvans S, Mayol X, Mojal S, Gil MJ, et al. Postoperative intra-abdominal infection and colorectal cancer recurrence: a prospective matched cohort study of inflammatory and angiogenic responses as mechanisms involved in this association. Eur J Surg Oncol. 2015;41(2):208-14.
26.Sammour T, Singh PP, Zargar-Shoshtari K, Su'a B, Hill AG. Peritoneal Cytokine Levels Can Predict Anastomotic Leak on the First Postoperative Day. Dis Colon Rectum. 2016;59(6):551-6.
27.Bilgin IA, Hatipoglu E, Aghayeva A, Arikan AE, Incir S, Mamal Torun M, et al. Predicting Value of Serum Procalcitonin, C-Reactive Protein, Drain Fluid Culture, Drain Fluid Interleukin-6, and Tumor Necrosis Factor-alpha Levels in Anastomotic Leakage after Rectal Resection. Surg Infect (Larchmt). 2017;18(3):350-6.
28.Zielinska-Borkowska U, Dib N, Tarnowski W, Skirecki T. Monitoring of procalcitonin but not interleukin-6 is useful for the early prediction of anastomotic leakage after colorectal surgery. Clin Chem Lab Med. 2017;55(7):1053-9.
29.Su'a B, Milne T, Jaung R, Jin JZ, Svirskis D, Bissett IP, et al. Detection of Anastomotic Leakage Following Elective Colonic Surgery: Results of the Prospective Biomarkers and Anastomotic Leakage (BALL) Study. J Surg Res. 2022;273:85-92.
30.Shi J, Wu Z, Wu X, Shan F, Zhang Y, Ying X, et al. Early diagnosis of anastomotic leakage after colorectal cancer surgery using an inflammatory factors-based score system. BJS Open. 2022;6(3): zrac069.
31.Capolupo GT, Galvain T, Parago V, Tong C, Masciana G, Di Berardino S, et al. In-hospital economic burden of anastomotic leakage after colorectal anastomosis surgery: a real-world cost analysis in Italy. Expert Rev Pharmacoecon Outcomes Res. 2022;22(4):691-7.
32.Kang J, Kim H, Park H, Lee B, Lee KY. Risk factors and economic burden of postoperative anastomotic leakage related events in patients who underwent surgeries for colorectal cancer. PLoS One. 2022;17(5):e0267950.
33.Arron MNN, Custers JAE, van Goor H, van Duijnhoven FJB, Kampman E, Kouwenhoven EA, et al. The association between anastomotic leakage and health-related quality of life after colorectal cancer surgery. Colorectal Dis. Epub 2023 Mar 31.
34.Bashir Mohamed K, Hansen CH, Krarup PM, Fransgard T, Madsen MT, Gogenur I. The impact of anastomotic leakage on recurrence and long-term survival in patients with colonic cancer: A systematic review and meta-analysis. Eur J Surg Oncol. 2020;46(3):439-47.
35.Hirst NA, Tiernan JP, Millner PA, Jayne DG. Systematic review of methods to predict and detect anastomotic leakage in colorectal surgery. Colorectal Dis. 2014;16(2):95-109.
36.Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13.
37.Reeves N, Vogel I, Ghoroghi A, Ansell J, Cornish J, Torkington J. Peritoneal cytokines as a predictor of colorectal anastomotic leaks on postoperative day 1: a systematic review and meta-analysis. Tech Coloproctol. 2022;26(2):117-25.
38.Kang S, Narazaki M, Metwally H, Kishimoto T. Historical overview of the interleukin-6 family cytokine. J Exp Med. 2020;217(5).
39.Greca FH, Souza Filho ZA, Giovanini A, Camargo Junior CA, Rubin MR, Silva RF. Interleukin-6 (IL-6) influence on colonic anastomosis healing in rats. Acta Cir Bras. 2007;22(2):110-4.
40.Zubaidi AM, Hussain T, Alzoghaibi MA. The time course of cytokine expressions plays a determining role in faster healing of intestinal and colonic anastomatic wounds. Saudi J Gastroenterol. 2015; 21(6):412-7.
41.Kaur S, Bansal Y, Kumar R, Bansal G. A panoramic review of IL-6: Structure, pathophysiological roles and inhibitors. Bioorg Med Chem. 2020;28(5):115327.
42.Waldner MJ, Foersch S, Neurath MF. Interleukin-6--a key regulator of colorectal cancer development. Int J Biol Sci. 2012;8(9):1248-53.
Full Text Sources:
Abstract:
Views: 3741

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.