Surgery, Gastroenterology and Oncology
|
|
Background: Phyllodes tumors (PT) of the breast represent a rare entity of breast neoplasms, their unpredictable behavior and high recurrence potential present these tumors as a clinical challenge. Those tumors necessitate careful diagnostic evaluation and management. Our retrospective study aims to discuss the different clinico-pathological features as well as different management approaches for phyllodes tumors.
Methods: A retrospective review of 175 PT patients diagnosed and treated in our institution between 2006 and 2023 was conducted. Data were collected from the medical records of our oncology center. The patients' epidemiological, clinical, pathological, therapeutic, and oncological data were analyzed.
Results: Our results denoted the mean age of PTs diagnosis to be 42.2 (14 – 81) years, with a mean radiological size of 57.76 (8-200) mm. The incidence of malignant PTs was 17.8% (31 cases). All patients in our research received surgery as their primary treatment, where 51 (29.5%) underwent lumpectomy and 91 (52.6%) underwent wide local excision. Mastectomy was the treatment used for 27 (15.6%) patients. 16.4% of PT patients (28/170) experienced recurrence, with a mean follow-up period of 161.93 months. Malignant recurrence was reported mainly among patients > 35 years old (13/16 patients, p value= 0.56). The mean DFS of malignant phyllodes in this cohort was 67.27 months (95% CI: 32.9-101.6 months). The mean OAS of malignant phyllodes in this cohort was 112.82 months (95% CI: 68.2-157.4 months), while non-malignant pathology had a OAS mean of 177.54 months (95% CI: 158.1-197 months).
Conclusion: Phyllodes tumors of the breast pose significant clinical challenges. Worse prognosis was noted in older age groups, larger tumor size, and higher tumor grade. Achieving clear surgical margins, and maintaining rigorous long-term follow-up are the cornerstone management of PTs. Still future studies with larger sample sizes are needed.
INTRODUCTION
Phyllodes tumors (PTs) of the breast are rare fibroepithelial neoplasms, accounting for 0.3-1% of all breast tumors (1). Though its rarity, It has been a quiet debatable topic in the literature for years, given its unpredictable behavior (2), the wide range of the age groups affected by the disease (3), and the different prognostic factors affecting its DFS and OS.
It’s highly recurrent nature drove the attention of researchers to collect as much data as possible, in order to understand its clinicopathological features and hence offer more suitable treatment options for the patients (4).
PTs generally comprise two cellular components: epithelial component and stromal component (5), which later determines the tumor grade (6). PTs are classified into benign, borderline, and malignant grades based on their histological features (3,5). The known local recurrence rates for benign, borderline, and malignant phyllodes are 7.1%, 16.7%, and 25.1% respectively (7). Surgical management is the cornerstone of PT treatment to this day, but the ideal surgical safety margin width remains controversial (8,9). The National Comprehensive Cancer Network (NCCN) guidelines recommend 1 cm as surgical margin, recently, some authors suggested that a safety margin < 1 cm in diameter might be oncologically safe (10). Till now, the role of adjuvant chemotherapy is less defined compared to other breast cancers. Additionally, there is no final word about adjuvant radiotherapy as a complementary treatment (11). The small number of studied patients hinders the understanding of the correlation between the published clinicopathological factors and the prognosis of such disease.
In this paper, a reasonable number of PT patients were included, and their clinical data were collected and analyzed, in order to offer a better understanding of the correlation between the different risk factors and the prognosis of PT, hence better chances for PT patients to receive curative treatment.
PATIENTS AND METHODS
Patients
A retrospective review of PT patients diagnosed and treated in our institution between May 2006 and May 2023 was conducted. Data was collected from the prospectively maintained medical records of our center.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows:
all patients with pathologically confirmed PT,
patients without any other malignancy, and
patients who underwent surgical intervention.
The exclusion criteria included the following:
1. PT patients with associated breast carcinoma elements,
2. lack of clinicopathological and treatment information.
The total number included was 175. The inclusion criteria were met across all 175 patients. However, due to the retrospective nature of the study, sample sizes for specific analyses vary depending on data availability. For example, physical examination data were available for 133 patients, and radiological tumor size was analyzed in 146 patients. The variability in sample sizes is clearly reported in the results section to maintain transparency and accuracy. This approach aligns with standard practices in retrospective research, where missing data are common and statistical analyses are adjusted accordingly.
Ethical Approval
The study was approved by Mansoura Faculty of Medicine Institutional Research Board (MFM-IRB) 2.2.?
Methods
The analyzed clinicopathological factors and treatment modalities included age, medical history, fibroadenoma surgical history, clinical and radiological tumor size, the initial diagnosis by preoperative core needle biopsy, type of surgery, axillary procedure, adjuvant chemotherapy and adjuvant radiotherapy. The postoperative histopathology of all cases was reviewed by expert pathologists from our institution. And for the cases initially operated outside the oncology center, the paraffin sections were retrieved and revised by our pathologists to confirm the final diagnosis. The recurrent cases were identified after the histopathological examination of specimens from the last excision.
Statistical Analysis
The data of patients in this study were analyzed using SPSS version 26 (Inc, Chicago, IL) on MacOS (iOS version 11.7). Continuous variables were presented as means or medians and range (according to their distribution), while categorical variables were presented as proportions. Bivariate analysis (between categorical variables) was done using Chi-Square test. Independent sample T-test was used to compare the means of different groups and dependent variables.
P value of < 0.05 was considered statistically significant. DFS, defined as the time from surgery until relapse, and overall survival (OS), defined as the time from diagnosis to the time of last follow up or death were computed using the Kaplan-Meier method.
RESULTS
Patient Characteristics
This study included 175 PT cases diagnosed and treated at the Oncology Center of Mansoura University from 2006 to 2023.
Table 1 - Clinico-pathological factors of phyllodes tumor patients
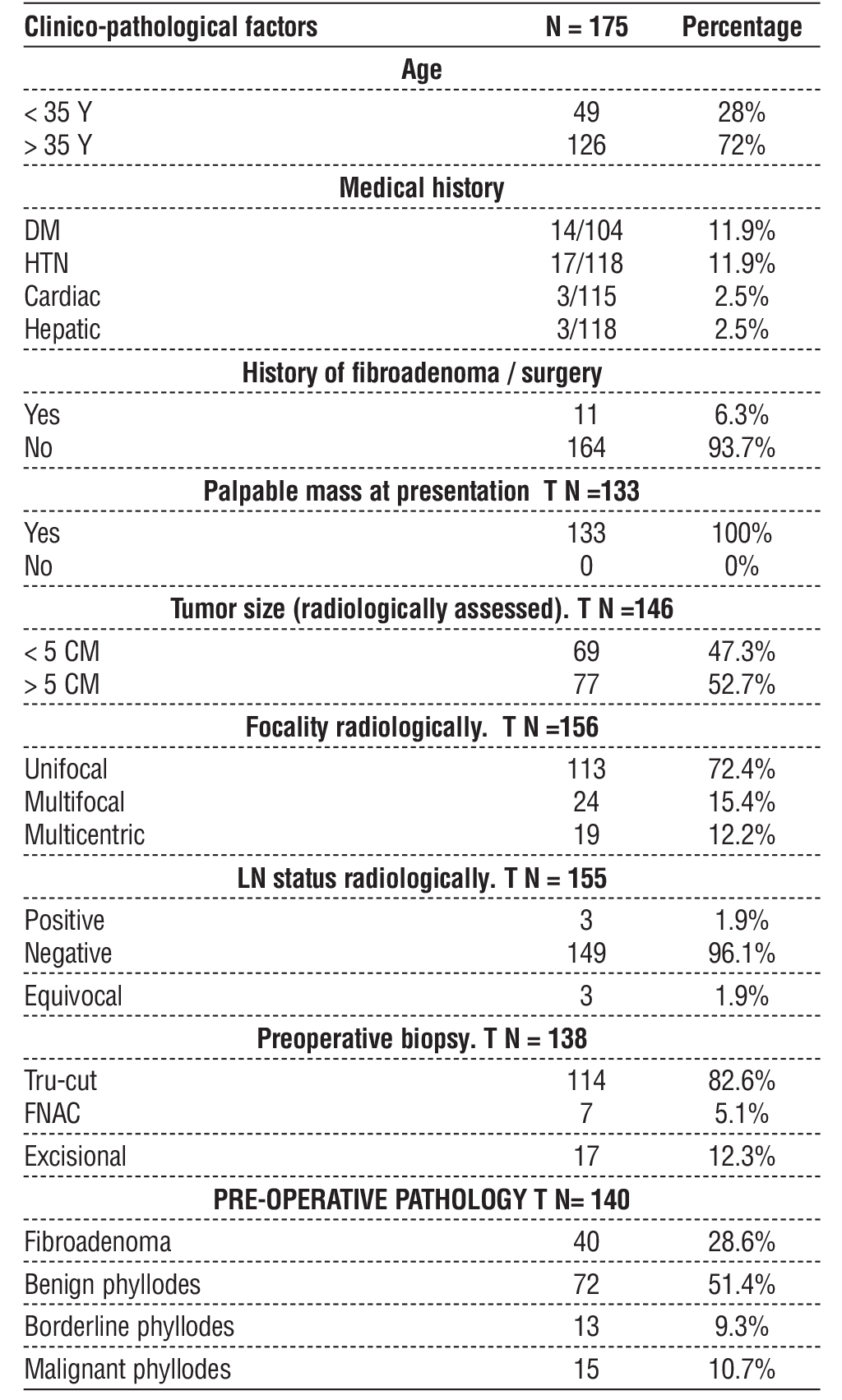 The clinicopathological features of these patients are represented in (table 1). Their mean age at diagnosis was 42.2 (14 – 81) years, 49 (28%) of them were ? 35 years of age. Clinically, 133 patients were presented with a palpable breast lump, with a mean radiological size of 57.76 (8-200) mm, 77/146 (52.7 %) of cases had tumors larger than 5 cm in diameter, being unifocal in 113/156 patients (72.4%), and multicentric in 19/156 (12.2%). 44.1% of cases had a BIRADS score of 4a. A preoperative core needle biopsy was performed in 114/138 (82.6%) patients, with 71.42% having a pre-surgical diagnosis of phyllodes tumor, and 15 (10.7%) cases were found to be malignant. None of the patients received any type of neoadjuvant therapy.
The clinicopathological features of these patients are represented in (table 1). Their mean age at diagnosis was 42.2 (14 – 81) years, 49 (28%) of them were ? 35 years of age. Clinically, 133 patients were presented with a palpable breast lump, with a mean radiological size of 57.76 (8-200) mm, 77/146 (52.7 %) of cases had tumors larger than 5 cm in diameter, being unifocal in 113/156 patients (72.4%), and multicentric in 19/156 (12.2%). 44.1% of cases had a BIRADS score of 4a. A preoperative core needle biopsy was performed in 114/138 (82.6%) patients, with 71.42% having a pre-surgical diagnosis of phyllodes tumor, and 15 (10.7%) cases were found to be malignant. None of the patients received any type of neoadjuvant therapy.
Malignant PT
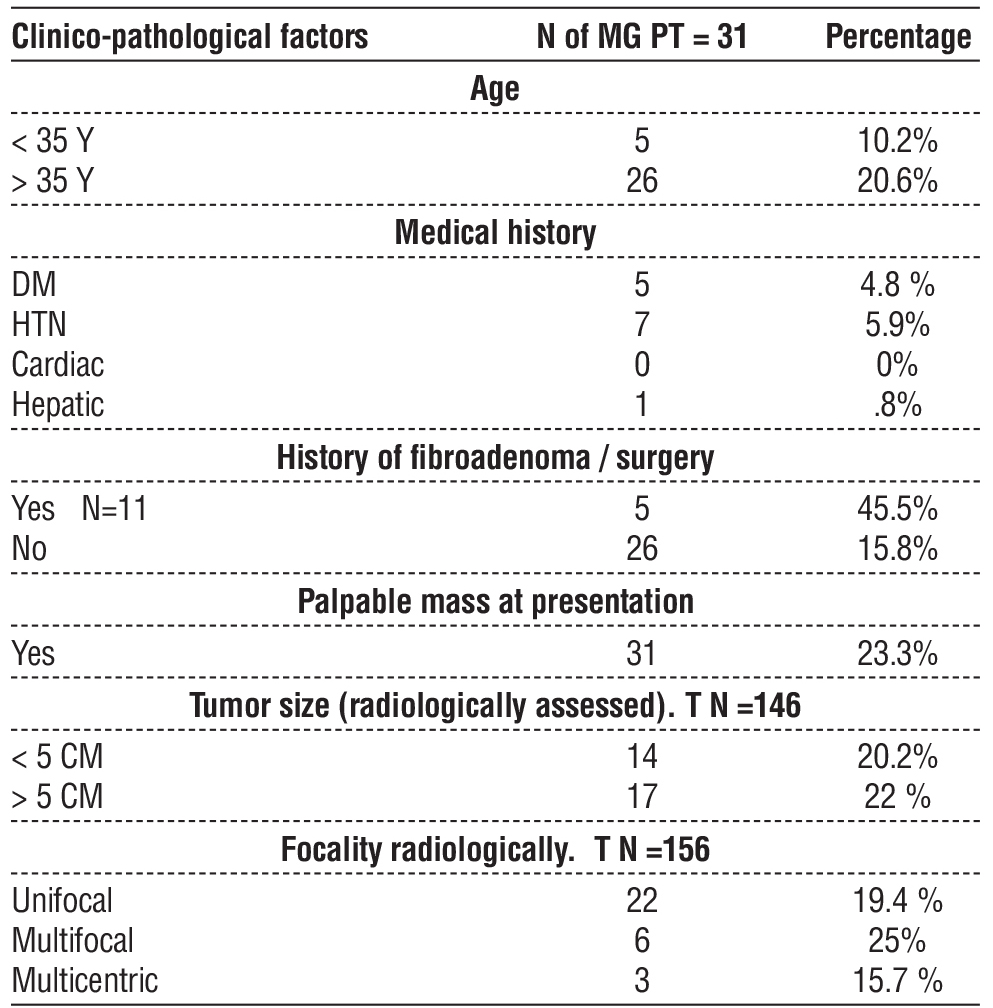
In our study, the incidence of malignant PTs at final diagnosis was 17.8% (31 cases), The number of Mg PT cases was estimated for each age group in (table 2), 10.2% of young patients (< 35 y.o) were found to be malignant, vs 20.6% of Mg PT in patients older than 35 y.o. 5 cases out of 11 with a history of fibroadenoma were diagnosed as Mg PT. All Mg PT cases were presented with a palpable mass in variable sizes, 22% of tumors larger than 5 cm in diameter were malignant.
Table 2 - Incidence of malignant phyllodes in different PT subgroups
Treatment
All patients in our research received surgery as their primary treatment (table 3), where 51 (29.5%) underwent lumpectomy and 91 (52.6%) underwent wide local excision. Mastectomy was the treatment used for 27 (15.6%) patients, four of them underwent immediate breast reconstruction. Axillary surgery was only performed in 6 patients, 3 patients, where axillary LNs were radiologically equivocal, had sentinel LN biopsy and frozen section, 2 of them were proven malignant by frozen section and received Axillary lymph node dissection (ALND). Another 3 patients, whose axillary LNs were radiologically suspicious, received ALND, all three turned out to have positive LN affection in postoperative pathology. The sum of 5 patients were proven to have LN metastasis. A total of 8/170 (4.7%) patients received adjuvant chemotherapy. While 7/170 patients received adjuvant radiotherapy.
Table 3 - Different treatment approaches for phyllodes tumor patients

Recurrence and Prognosis
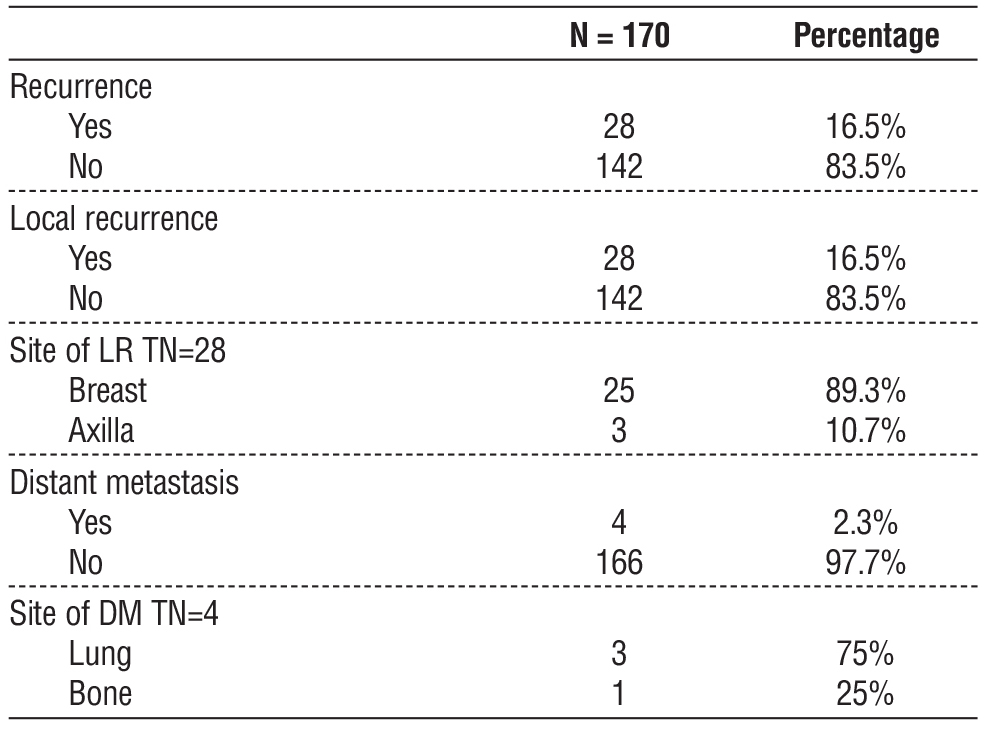
16.4% of PT patients (28/170) experienced recurrence, with a mean follow-up period of 161.93 months. All of recurrent cases had local recurrence (LR), 4 of them were presented with distant metastases (DM) (table 4), 25 of the LR cases were presented with ipsilateral breast LR, who were managed according to the size of recurrence, either by wider excision or mastectomy, while 3 of them experienced axillary LN metastasis. 3 of the DM cases were lung metastasis, only one case showed bone metastasis. All DM cases received chemotherapy. Death occurred in 14/174 (8%) patients, 6 of them were experiencing malignant recurrence.
Table 4 - Sites and rates of PT recurrence
DFS and OAS
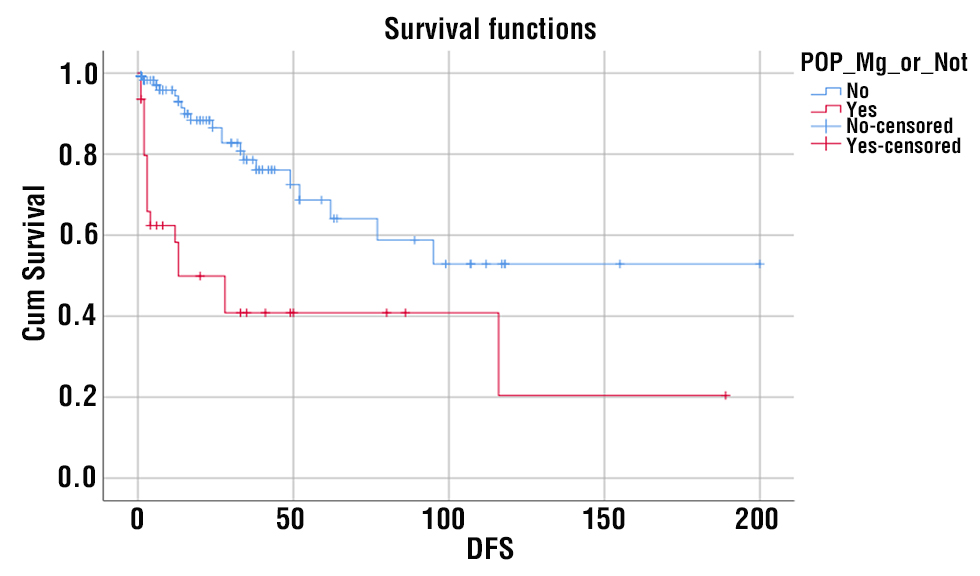
Malignant phyllodes showed significantly lower disease-free survival (DFS) compared with benign and border-line pathology (p <0.001). The mean DFS of malignant phyllodes in this cohort was 67.27 months (95% CI: 32.9-101.6 months), while non-malignant pathology had a DFS mean of 127.07 months (95% CI: 99.9-154.2 months) (fig. 1).
Figure 1 - DFS of malignant and non-malignant phyllodes tumor of the breast
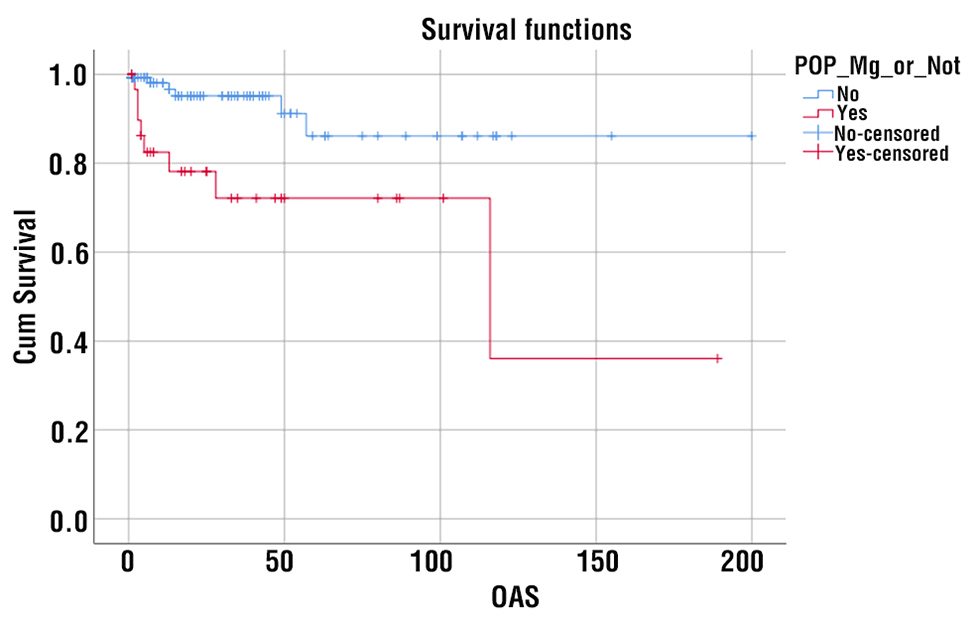
Similarly, malignant phyllodes showed significantly lower overall survival (OAS) compared with benign and border-line pathology (p=0.002). The mean OAS of malignant phyllodes in this cohort was 112.82 months (95% CI: 68.2-157.4 months), while non-malignant pathology had a OAS mean of 177.54 months (95% CI: 158.1-197 months) (fig. 2).
Correlation with Recurrence
Phyllodes tumor recurred in 16% of patients of our study. Malignant recurrence was reported mainly among patients > 35 years old (13/16 patients, p value = 0.56), without past history of excision of fibro-adenoma (p value= 0.27). Diagnosis of malignant phyllodes tumor was significantly correlated with recurrence (table 5) compared to benign and borderline diseases (p value <0.001).
Table 5 - Clinicopathologic parameters analysis of malignant phyllodes tumor recurrence

DISCUSSION
Phyllodes tumors of the breast have been widely investigated in recent times, given their different presentations and the multiple prognostic factors linked to them (12). The histopathological background of these tumors determines their behavior and mostly predicts their correlation with other clinicopathological factors.
Figure 2 - OAS of malignant and non-malignant phyllodes tumor of the breast
 The known local recurrence rates for benign, borderline, and malignant phyllodes are7.1%, 16.7%, and 25.1% respectively (7). PT recurrence is thought to be influenced by tumor size, stromal atypia and cellularity, stromal overgrowth, mitotic activity, and margin status. With no clear correlation till this moment (12).
The known local recurrence rates for benign, borderline, and malignant phyllodes are7.1%, 16.7%, and 25.1% respectively (7). PT recurrence is thought to be influenced by tumor size, stromal atypia and cellularity, stromal overgrowth, mitotic activity, and margin status. With no clear correlation till this moment (12). In this paper, we tried to investigate some of these clinicopathological parameters, with the association of the incidence of Mg PT and recurrence rates.
Age is thought to be a significant prognostic factor in PTs, that usually occur in middle-aged women 35-50 years (13). Few studies in the literature highlighted the correlation between age and recurrence, some of these studies denote that younger age at presentation tends to be associated with poorer outcomes, particularly those under 35 years old, that are more likely to have larger tumors and higher rates of recurrence compared to older patients (11). In a study of 106 PT patients, all were surgically treated, patients younger than 20 years old had higher recurrence rates (14). This aggressive biological behavior is thought to be due to the delayed detection among young patients. On the contrary, A study on 7 patients between the ages of 10 and 17 years, suggested that phyllodes tumors at young age were found to be benign and less aggressive, even suggesting simple or wide local excision as a curative surgical management, rather than mastectomy (15). Another study in 2017 by kim on 1974 Mg PT patients reported that older age (>50 years) was associated with worse prognosis and more extensive tumor behavior (16).
In agreement with the kim study, we found that the incidence of Mg PT diagnosis was higher in patients older than 35y.o (20.6%), vs 10.2% in patients < 35, with larger tumor size and more invasive behavior. Amongst the 27 cases that required mastectomy, 24 of them were older than 35 y.o, While Simple or wide local excision was enough for almost all the young patients, except for three cases that required mastectomy. The recurrence rate between the two groups (>35y.o, <35y.o) was almost equal, 15.8% and 14.2% respectively, the recurrent tumor upgrading was also similar in both groups, as 3 cases >35y.o were diagnosed postoperatively as benign phyllodes, and the recurrence pathology turned out to be malignant, versus 2 cases < 35 y.o. One case in each group experienced a borderline PT recurrence after Benign PT primary.
PTs are presented in variable size range, with an average size of 5 cm, though it could grow up to 40 cm as reported by Testori et al (13). PT prognosis is significantly influenced by their size and growth rate, studies have shown that tumors larger than 5 cm are more likely to exhibit malignant behavior (17), including increased mitotic activity and stromal overgrowth, which are indicators of aggressive biological behavior and hence poor prognosis (18). The relationship between the size of PT and local recurrence is controversial. Additionally, some studies found that larger tumors were more likely to develop local recurrence (19).
In our cohort, the mean radiological size was 57.76 mm, 77/146 (52.7 %) of cases had tumors larger than 5 cm in diameter. Those tumors were associated with higher incidence of recurrence, with a recurrence rate of 17.3% vs 11.8% in tumors < 5 cm (table 5). Another finding demonstrated, was that all the cases with tumor histological upgrading in recurrence were larger than 5 cm in diameter, thus highlighting the significance of PT size in predicting the tumor behavior and prognosis.
Phyllodes tumors and Fibroadenomas represent distinct entities in breast pathology, with varying historical backgrounds and prognostic implications (20). Fibroadenomas, are common benign breast tumors composed of both epithelial and stromal elements. Their typically predicted behavior favors conservative management in most cases (21). In contrast, phyllodes tumors, named for their leaf-like projections within the breast tissue, (22) were recognized for their aggressive behavior despite being identified as benign initially. the misdiagnosis of phyllodes as fibroadenoma might direct the treatment decision to inadequate surgical management, with all the cons of such inadequacy (20). The pathological overlapping features make it difficult to identify PT pre-operatively, (23). the lack of tissue in CNB might have a role, yet CNB remains the most reliable pre-operative diagnostic method compared to other investigations (24). A sensitivity for pre-operative diagnosis of PTs by CNB was reported to be 65% (25,26).
In our cohort, 114 patients were diagnosed pre-operatively by CNB 40 cases were initially misdiagnosed as fibroadenoma by CNB, and then diagnosed post-operatively as benign and borderline PTs, only two of them (2/40) were diagnosed as malignant PT in the POP. The total number of patients correctly diagnosed CNB was 74/114 (64.9%), of which 10 cases were diagnosed as Mg PT preoperatively by CNB. Accordingly, we contend that CNB, despite the relatively high false negative rate, is yet superior to other methods in diagnosing PT.
PTs mostly arise de novo, though extremely rare, some studies reported transformation from fibroadenoma to PT, (27). another study stated some evidence of Mg PT transformation from FA, without a proven mechanism (28). Some reports suggested that trauma, pregnancy, lactation, and disturbed estrogen activity might be linked to the transformation of FAs to PTs, they also denoted that breast epithelium growth factors such as Endothelin-1 might have a role (29). Recent genome studies identified shared MDM12 mutations between FAs and PTs, supporting the theory that these 2 lesions share a common origin (28,30). In our study, 11 PT patients had a history of fibro-adenoma, 5 of them had a confirmed pathology of malignant PT, and 4/11 cases experienced recurrence. Yet there was no definitive data about whether the PT tumor was FA transformation or a just concurrent finding.
The main primary treatment for PTs is surgical treatment, wide local excision (WLE), which involves tumor resection with a 1 cm free margin all around is the procedure recommended by the NCCN guidelines (31). As for patients with large aggressive tumors compared to their breast size, mastectomy might be necessary (32). However, in a systematic review by Shaban et al, in which 12 studies of 1700 patients were collected, the recurrence rates between 10 mm safety margin and 1 mm margin were almost equal (7.9%) and (5.7%) respectively (10).
In our cohort, Excision (enucleation), was the procedure used for benign PT cases (51 cases - 29.5%), while WLE (defined as 1mm-1cm surgical margin) was the procedure used for borderline and malignant PTs mainly, also for large rapidly growing benign tumors (91 cases-52.6%), mastectomy was only used in Mg PT cases, that are presented with large tumor size, as breast conservation could not be achieved (27 cases- 15.6%). The recurrence rate in the group treated by excision was 23.5%, while the group treated by WLE was 6.6%. So we denote a significant relation between wide margins and recurrence, standing with the studies that recommend wide safety margins for PT management. The recurrence rate in the mastectomy group was 29.6%, considering the aggressive behavior of the primary tumor in these cases also being histologically malignant.
Phyllodes tumors are notable for their potential to recur (20). PT recurrence is influenced by several factors including age, tumor size, surgical margins, and histological grade (33). Studies have shown that larger tumor size and positive surgical margins have higher chances of recurrence, also high- grade tumors with increased stromal cellularity and atypical features are more likely to have aggressive biological behavior and high recurrence rates. Post-surgical vigilant monitoring is crucial, as recurrence might occur even years after initial excision, mostly within two years (2). In our study, the recurrence rates of benign, borderline, and malignant PTs were 8 %, 22.5%, and 35.4% respectively. Larger tumors were associated with higher incidence of recurrence, most recurrences occurred within 2 years of the initial excision.
The recurrent cases were managed according to the site of recurrence. Cases with small-sized local recurrent tumors received wider local excision (10 cases), while those of relatively large recurrent tumors received simple mastectomy (8) with or without reconstruction as a surgical management, sometimes combined with RT (2 cases). As for cases with axillary local recurrence (2 cases) without evidence of breast local recurrence, they received axillary clearance, and modified radical mastectomy was only used in one case of both, breast and axillary LR. The rest of the cases lost follow up.
For DM cases (4 cases), chemotherapy was used in 3 of them, one case received combined chemotherapy and hormonal therapy as a systemic treatment.
Unlike the majority of breast tumors, that are known for their potential of axillary LN metastasis, phyllodes tumors have a less predictable pattern of lymphatic spread. They are known for their potential for local and distant spread rather than regional LN involvement. In fact, LN metastasis is relatively rare in phyllodes tumors (34). The presence of lymph node metastases in PT often signifies a more advanced or aggressive disease, but it remains an unusual finding compared to other breast cancers. The common route of metastasis for phyllodes tumors is hematogenous, mainly to the lungs and liver then to the bone (35). Axillary LN dissection is only indicated when LNs are proved to be positive, other than that, only free surgical margins is the primary management indicated (36).
In our study, almost all cases were LN-free and required no axillary surgery, only 5/175 were proved to be LN positive and received axillary LN dissection.
As for DM, 4 cases experienced DM, 3 to the lung, and one to the bone, one of the 3 lung DM cases had no local recurrence, and presented only with lung metastasis, and the bone DM case experienced axillary LR. All 4 cases were Mg PT, in both the primary lesion and the pathology of recurrence.
Till now, the benefit of adjuvant chemotherapy is not defined, however, the application of chest radiotherapy after surgery in borderline and malignant PTs has been shown to reduce the risk of LR (23,37). Belkacémi et al supported that theory, and also denoted that RT had no effect on the DFS and OAS (19).
In our study, 8 Mg PT cases received adjuvant chemotherapy, and 3 of them experienced LR with no DM. As for radiotherapy, 7 Mg PT cases received adjuvant RT, 3/7 cases experienced recurrence, one had breast LR, the second case had axillary LR without breast LR, and the third case had DM without evidence of LR. Therefore, we did not observe any additional benefit from using adjuvant therapy in the limited number of cases where it was applied.
Limitations
This study has several limitations that should be considered. First, as a retrospective cohort analysis conducted in a single institution, the findings may lack generalizability to broader populations. The relatively small sample size, particularly for cases receiving adjuvant therapy, limits the statistical power to draw definitive conclusions about the effectiveness of such treatments. Additionally, the absence of long-term follow-up data for some patients may underestimate late recurrences or distant metastases. Furthermore, the reliance on historical medical records may have introduced biases or inaccuracies in data collection or analysis of a unstandardized medical practice in the old cases.
CONCLUSION
Phyllodes tumors of the breast pose a significant clinical challenge due to their diverse biological behavior and high recurrence potential. Our study emphasizes the critical need for accurate preoperative diagnosis, attaining clear surgical margins, and maintaining rigorous long-term follow-up. While surgery remains the primary treatment modality, the effectiveness of adjuvant therapies requires further investigation. Prospective studies with larger sample sizes and extended follow-up are essential to confirm these findings and optimize management strategies for this rare condition.
Author’s Contributions
All authors have read and approved the manuscript. S.El , S.S , R. M.A , E.W, M.S.El are responsible for the data collection and editing, K.A , S.El , K.m.Ali , M.Z : writing and revision , O.H and M.S : data analysis, preparation and revision.
Acknowledgements
We acknowledge the contributions of the Surgical Oncology Department staff, and the entire department members, in Oncology Center of Mansoura University, who provided precious support and assistance throughout this study.
Competing Interests
No competing interests to be declared.
Funding
No funding was received for this manuscript
Consent to Participate
Human participant protocols followed in this study complied with the ethical standards mandated by the institutional review board, the 1964 Helsinki Declaration, including its subsequent revisions, and equivalent ethical guidelines. IRB number: R.24.06.2676.
Availability of Data and Materials
All data utilized in this study are accessible through the Mansoura University medical system (Ibn Sina Hospital management system) https://srv137.mans. edu.eg/mus/newSystem/.
REFERENCES
1. Piscuoglio S, Ky Ng C, Murray M, Burke KA, Edelweiss M, Geyer FC, et al. Massively parallel sequencing of phyllodes tumours of the breast reveals actionable mutations, and TERT promoter hotspot mutations and TERT gene amplification as likely drivers of progression. J Pathol. 2016;238(4):508-18.
2. Tan PH, Thike AA, Tan WJ, Myint Thu MM, Busmanis I, Li H, et al. Predicting clinical behaviour of breast phyllodes tumours: a nomogram based on histological criteria and surgical margins. J Clin Pathol. 2012;65(1):69-76.
3. Nielsen VT, Andreasen C. Phyllodes tumour of the male breast. Histopathology. 1987;11(7):761-2.
4. Sain B, Gupta A, Ghose A, Halder S, Mukherjee V, Bhattacharya S, et al. Clinico-Pathological Factors Determining Recurrence of Phyllodes Tumors of the Breast: The 25-Year Experience at a Tertiary Cancer Centre. J Pers Med. 2023;13(5):866.
5. Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ, eds. World Health Organization Classification of Tumours of the Breast. Lyon, France: IARC; 2012. World Health Organization Classification of Tumours; vol 4.
6. Yasir S, Gamez R, Jenkins S, Visscher DW, Nassar A. Significant histologic features differentiating cellular fibroadenoma from phyllodes tumor on core needle biopsy specimens. Am J Clin Pathol. 2014;142(3):362-9.
7. Yu CY, Huang TW, Tam KW. Management of phyllodes tumor: A systematic review and meta-analysis of real-world evidence. Int J Surg. 2022;107:106969.
8. Toussaint A, Piaget-Rossel R, Stormacq C, Mathevet P, Lepigeon K, Taffé P. Width of margins in phyllodes tumors of the breast: the controversy drags on - a systematic review and meta-analysis. Breast Cancer Res Treat. 2021;185(1):21-37.
9. Neron M, Sajous C, Thezenas S, Piperno-Neumann S, Reyal F, Laé M, et al. Surgical Margins and Adjuvant Therapies in Malignant Phyllodes Tumors of the Breast: A Multicenter Retrospective Study. Ann Surg Oncol. 2020;27(6):1818-1827.
10. Shaaban M, Barthelmes L. Benign phyllodes tumours of the breast: (Over) treatment of margins - A literature review. Eur J Surg Oncol. 2017;43(7):1186-1190.
11. Spitaleri G, Toesca A, Botteri E, Bottiglieri L, Rotmensz N, Boselli S, et al. Breast phyllodes tumor: A review of literature and a single center retrospective series analysis. Crit Rev Oncol Hematol. 2013; 88(2):427-36.
12. Zhou ZR, Wang CC, Yang ZZ, Yu XL, Guo XM. Phyllodes tumors of the breast: diagnosis, treatment and prognostic factors related to recurrence. J Thorac Dis. 2016;8(11):3361-3368.
13. Testori A, Meroni S, Errico V, Travaglini R, Voulaz E, Alloisio M. Huge malignant phyllodes breast tumor: A real entity in a new era of early breast cancer. World J Surg Oncol. 2015;13:81.
14. Chua CL, Thomas A. Cystosarcoma phyllodes tumors. Surg Gynecol Obstet. 1988;166(4):302-6.
15. Amerson JR. Cystosarcoma phyllodes in adolescent females. A report of seven patients. Ann Surg. 1970;171(6):849-56.
16. Kim YJ, Kim K. Radiation therapy for malignant phyllodes tumor of the breast: an analysis of SEER data. Breast. 2017;32:26-32.
17. Atalay C, K?naæ V, Çelebio?lu S. Analysis of patients with phyllodes tumor of the breast. Ulus Cerrahi Derg. 2014;30(3):129-32.
18. Ravindhran B, Rajan S. Predictive factors of early recurrence in patients with phyllodes tumor of the breast. Eur J Breast Health. 2020;17(1):10-14.
19. Belkacémi Y, Bousquet G, Marsiglia H, Ray-Coquard I, Magné N, Malard Y, et al. Phyllodes tumor of the breast. Int J Radiat Oncol Biol Phys. 2008;70(2):492-500.
20. Karim RZ, Gerega SK, Yang YH, Spillane A, Carmalt H, Scolyer RA, et al. Phyllodes tumours of the breast: a clinicopathological analysis of 65 cases from a single institution. Breast. 2009;18(3):165-70.
21. Liu XF, Zhang JX, Zhou Q, Chen F, Shao ZM, Lu C. A clinical study on the resection of breast fibroadenoma using two types of incision. Scand J Surg. 2011;100(3):147-52.
22. Fiks A. Cystosarcoma phyllodes of the mammary gland - Müller's tumor. For the 180th birthday of Johannes Müller. Virchows Arch A Pathol Anat Histol. 1981;392(1):1-6.
23. Tan BY, Acs G, Apple SK, Badve S, Bleiweiss IJ, Brogi E, et al., Phyllodes tumours of the breast: a consensus review. Histopathology. 2016;68(1):5-21.
24. Ward ST, Jewkes AJ, Jones BG, Chaudhri S, Hejmadi RK, Ismail T, Hallissey MT. Ward et al. The sensitivity of needle core biopsy in combination with other investigations for the diagnosis of phyllodes tumours of the breast. Int J Surg. 2012;10(9):527-31.
25. Pezner RD, Schultheiss TE, Paz IB. Malignant phyllodes tumor of the breast: local control rates with surgery alone. Int J Radiat Oncol Biol Phys. 2008;71(3):710-3.
26. Mishra SP, Tiwary SK, Mishra M, Khanna AK. Phyllodes tumor of breast: a review article. ISRN Surg. 2013:2013:361469.
27. Mitus J, Blecharz P, Jakubowicz J, Reinfuss M, Walasek T, Wysocki W. Phyllodes tumors of the breast. The treatment results for 340 patients from a single cancer centre. Breast. 2019;43:85-90.
28. Tan J, Ong CK, Lim WK, Young Ng CC, Thike AA, Ng LM, et al. Genomic landscapes of breast fibroepithelial tumors. Nat Genet. 2015;47(11):1341-5.
29. Mitus JW, Blecharz P, Jakubowicz J, Reinfuss M, Walasek T, Wysocki W. Phyllodes tumors of the breast. The treatment results for 340 patients from a single cancer centre. Breast. 2019;43:85-90.
30. Yoshida M, Sekine S, Ogawa R, Yoshida H, Maeshima A, Kanai Y, et al. Frequent MED12 mutations in phyllodes tumours of the breast. Br J Cancer. 2015;112(10):1703-8.
31. Network NCC. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Breast Cancer. 2022.
32. Yom CK, Han W, Kim SW, Park SY, Park IA, Noh DY. Reappraisal of conventional risk stratification for local recurrence based on clinical outcomes in 285 resected phyllodes tumors of the breast. Ann Surg Oncol. 2015;22(9):2912-8.
33. Zhang Y, Kleer CG. Phyllodes Tumor of the Breast: Histopathologic Features, Differential Diagnosis, and Molecular/Genetic Updates. Arch Pathol Lab Med. 2016;140(7):665-71.
34. Adesoye T, Neuman HB, Wilke LG, Schumacher JR, Steiman J, Greenberg CC. Current Trends in the Management of Phyllodes Tumors of the Breast. Ann Surg Oncol. 2016; 23(10):3199-205.
35. Acar T, Tarcan E, Hac?yanl? M, Kamer E, Peækersoy M, Seyran Yi?it, et al. How to approach phyllodes tumors of the breast? Ulus Cerrahi Derg. 2015;31(4):197-201.
36. Salvadori B, Cusumano F, Del Bo R, Delledonne V, Grassi M, Rovini D, et al. Surgical treatment of phyllodes tumors of the breast. Cancer. 1989;63(12):2532-6.
37. Gnerlich JL, Williams RT, Yao K, Jaskowiak N, Kulkarni SA. Utilization of radiotherapy for malignant phyllodes tumors: analysis of the National Cancer Data Base, 1998-2009. Ann Surg Oncol. 2014;21(4):1222-30.
Full Text Sources:
Abstract:
Views: 1945

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.