Surgery, Gastroenterology and Oncology
Official journal of the International Association of Surgeons, Gastroenterologists and Oncologists
|
|
Postoperative Movement of an Internal Stent Placed at the Anastomotic Site of Pancreaticojejunostomy During Pancreaticoduodenectomy
ABSTRACT
Purposes: This study aimed to investigate the postoperative movement of an internal stentplaced at the anastomotic site of pancreaticojejunostomy during pancreaticoduodenectomy.
Methods: Of the 70 patients who underwent pancreaticoduodenectomy using an internalstent at the anastomotic site of pancreaticojejunostomy between January 2014 andDecember 2019, 64 patients (91%) were included in this study. Stent fall from the anastomoticsite, stent excretion from the body, and stent migration into the pancreatic and bileduct, as well as stent-related complications were examined.
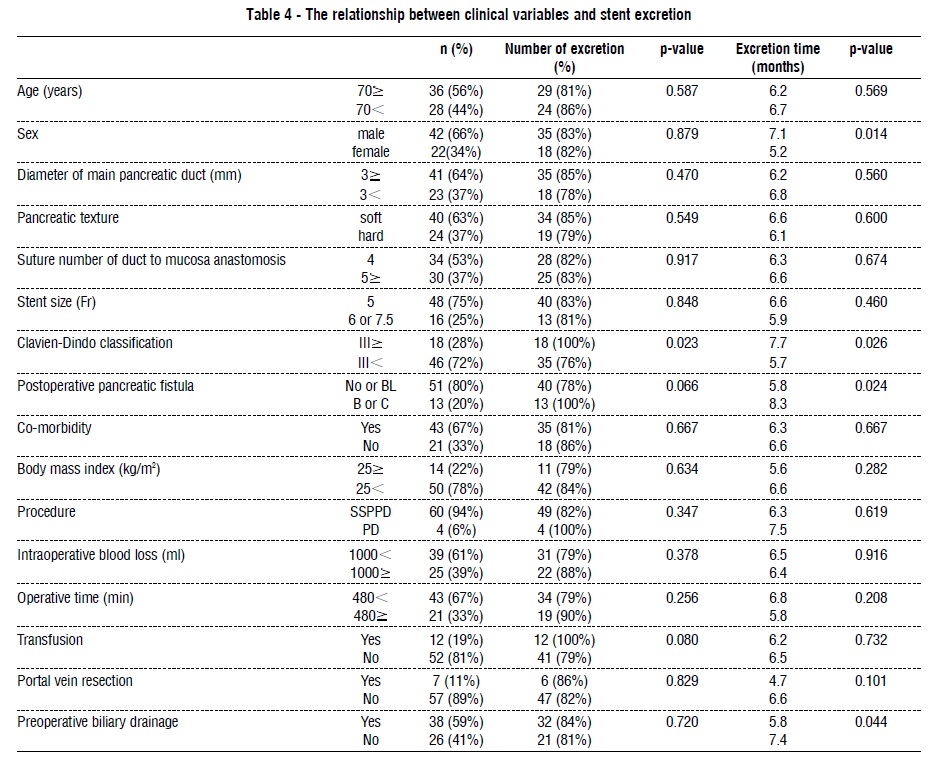
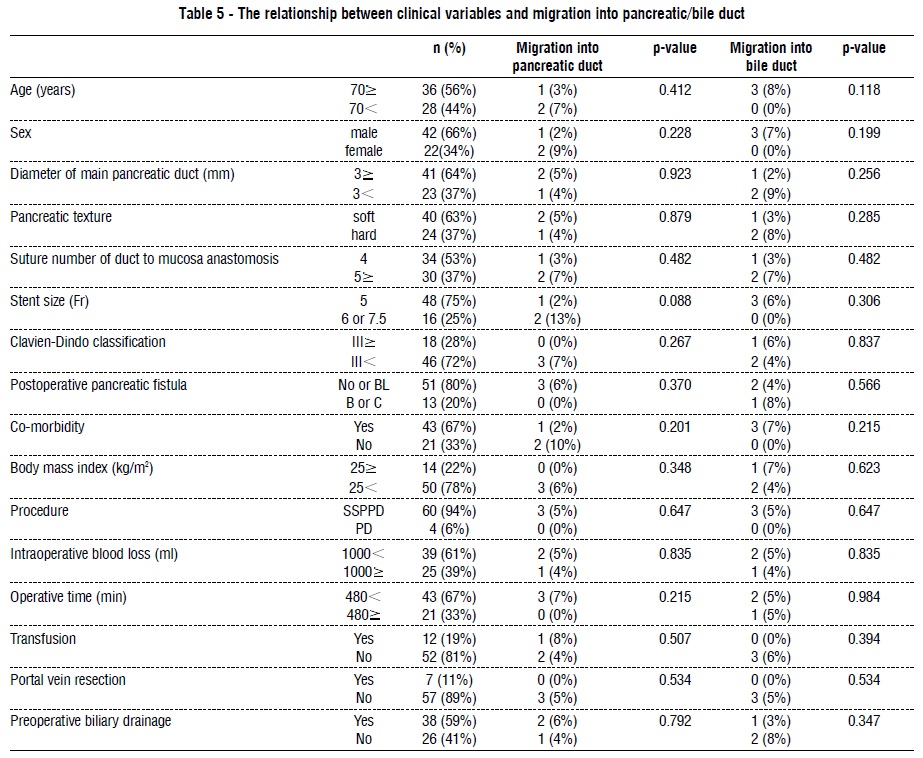
Results: The stent fall rate and excretion rate were 91% and 83%, respectively. Furthermore,migration rates into the pancreatic duct and bile duct were 5% each. There were nostent-related complications. Univariate analysis revealed that pancreatic texture and Clavien-Dindo classification differed significantly according to stent fall time (p=0.019, 0.045,respectively). Moreover, the Clavien-Dindo classification differed significantly according tothe number of stent excretions (p=0.023). Additionally, patient sex, Clavien-Dindo classification,postoperative pancreatic fistula, and preoperative biliary drainage differed significantlyaccording to stent excretion time (p=0.014, 0.026, 0.024, 0.044, respectively). Multivariateanalysis revealed that postoperative pancreatic fistula was an independent risk factor forexcretion time (p=0.047; HR 0.513, 95%CI; 0.266-0.992).
Conclusions: We observed the safe removal and excretion of internal stents from patientswho underwent pancreaticoduodenectomy. Additionally, patients with postoperative pancreaticfistula had significantly later stent excretion time.Key words: internal stent, pancreaticoduodenectomy, pancreaticojejunostomy
INTRODUCTION
A pancreatic duct stent is often placed at the anastomotic site ofpancreaticojejunostomy during pancreaticoduodenectomy. Two types ofpancreatic duct stents exist internal and external. An internal stent is used with the theory that it falls from the anastomotic siteand is excreted spontaneously from the body becauseit is fixed with absorbent threads (1). However, it isunclear when the stent fall and excretion occur.Thus, we retrospectively examined the postoperativemovement of an internal stent placed at the anastomoticsite of pancreaticojejunostomy during pancreaticoduodenectomy.
METHODS
Patients and procedures
Between January 2014 and December 2019, 70patients underwent pancreaticoduodenectomy atKatsushika Medical Center The Jikei University, using aninternal stent at the anastomotic site of pancreaticojejunostomy.Of these, 64 patients (91%) were includedin this study as they could be followed-up for oversix months. Sub-stomach preserving pancreaticoduodenectomyand conventional pancreaticoduodenectomywere performed in 60 and 4 patients(94% and 4%), respectively. Reconstruction consistedof an end-to-side pancreaticojejunostomy, an endto-side hepaticojejunostomy, and an antecolic endto-side gastrojejunostomy according to Child’sprocedure (2). Duct-to-mucosa anastomosis ofpancreaticojejuno-stomy was performed with polydioxanonesutures (5-0 PDS PLUS®; Ethicon), followinga pancreatic parenchymal-jejunal seromuscularanastomosis with polypropylene sutures (3-0 PROLENE®; Ethicon) using the modified Blumgartmethod (3). The pancreatic duct stent was apolyvinyl catheter (MD-41515 pancreatic duct tube;Sumitomo Bakelite, Japan) with multiple side holesand a small knot. Using an internal stented method,a pancreatic duct stent was cut 4 cm in length andwas positioned with one half in the main pancreaticduct and the other half in the jejunal lumen. Thestent was fixed at the anastomotic site using thedorsal thread of the pancreaticojejunostomy. Thebile duct stent in hepaticojejunostomy was notroutinely used. The closed drains were placed nearthe sites of the pancreaticojejunal and hepaticojejunalanastomoses, and were promptly removedafter confirming the absence of intra-abdominalcomplications. All patients were administeredprophylactic antibiotics for at least three days postoperatively,postoperative prophylactic octreotidewas not routinely used. Food intake started threedays postoperatively after confirming the absence ofintra-abdominal complications.
Evaluation
We routinely performed abdominal computedtomography (CT) seven days postoperatively. After thepatient was discharged, a follow-up CT was performedevery three or four months. The fall of the stent fromthe anastomotic site of the pancreaticojejunostomyand excretion of the stent from the body wereconfirmed by CT examination. Serum amylase levelsand drainage fluid volume were measured on postoperativedays 1, 3, and 5. Postoperative pancreaticfistula was defined according to the International StudyGroup on Pancreatic Fistula (ISGPF) (4). The severity ofother early complications was categorized according tothe Clavien-Dindo classification (5). This study wasapproved by the Ethics Committee of the JikeiUniversity School of Medicine. The approval number is30-322(9343).
Statistical analysis
Univariate analyses were performed using theMann-Whitney U-test or Chi-square test. Multivariateanalyses were performed using a logistic regressionanalysis. All data were analyzed using JMP Pro version12 (SAS Institute Inc.). Statistical significance was set atp<0.05, and data are expressed as mean ± standarddeviation.
RESULTS
Patient characteristics and operative variables areshown in table 1. The mean postoperative follow-upperiod was 24.1 ± 15.3 months (6-69). There were 42males (66%) and 22 females (34%), mean age=68.9 ±11.3 (31-87); mean body mass index=22.2 ± 4.2 kg/m2(15.2-33.3). The primary diseases were pancreaticcarcinoma (n=21, 33%), bile duct carcinoma (n=18,28%), intraductal papillary mucinous neoplasm (n=10,16%), duodenal carcinoma (n=5, 8%), ampulla of Vatercarcinoma (n=3, 5%), transverse colon carcinoma withduodenal invasion (n=2, 3%), neuroendocrine tumor(n=2, 3%), chronic pancreatitis (n=1, 2%), mucinous cystneoplasm (n=1, 2%) and pancreatic duct adenoma(n=1, 2%). Forty-three patients (67%) had comorbidities,including hypertension (n=39, 61%), diabetes mellitus(n=18, 28%), hyperlipidemia (n=16, 25%), ischemic heartdisease (n=7, 11%), and respiratory disease (n=1, 2%).The mean diameter of the main pancreatic duct was2.7±1.8 mm (1-10). The pancreatic texture was soft andhard in 24 and 40 patients (38% and 62%), respectively.The stent size was 5, 6, and 7.5 Fr in 48, 13, and 3 patients (75%, 20% and 5%), respectively. The numberof duct-to-mucosa anastomosis sutures was four in 34patients (53%), five in 1 patient (2%), six in 1 patient(2%), eight in 24 patients, ten in 3 patients (5%), andtwelve in 1 patient (2%). The mean operation time was449 ± 70 min (294-616), and the mean intraoperativeblood loss was 1,043 ± 750 mL (222-3,862). Transfusionwas performed in 12 patients (19%), portal veinresection in 7 patients (11%), and preoperative biliarydrainage in 38 patients (59%). The morbidity andmortality rates were 44% and 0%, respectively. Clavien-Dindo classification ( ) and postoperative pancreaticfistula (Grade B/C) occurred in 18 and 13 patients (28%and 20%), respectively. Reoperations were performedin 3 patients (5%) due to necrosis of the transversecolon, perforation of the transverse colon and internalhernia. The mean postoperative hospital stay was 25.2± 16.9 days (9-93). Postoperative movement of thestent is shown in table 2. The stent fell from the anastomoticsite in 58 patients (91%), while the stentremained in the anastomotic site in 6 patients (9%), one of whom died. The shortest stent fall time was on postoperativeday seven, and the stent fell within one yearin all patients. The mean stent fall time was 4.9 ± 2.0months. The stent was excreted from the bodies of 53patients (83%), while the stent remained in 11 patients(17%), four of whom died without excretion. The meanexcretion time was 6.4 ± 2.9 months. Meanwhile, stentswere excreted within six months and one year postoperativelyfrom 28 and 50 patients (44% and 78%),respectively. Stent migration into the pancreas occurredin 3 patients (5%): One had a stent that was spontaneouslyexcreted, one remained with a migrated stent,and one died with a migrated stent. Stent migrationinto the bile duct occurred in 3 patients (5%), all ofwhom subsequently were excreted spontaneously.There were neither stent-related complications (such aspancreatitis and cholangitis) postoperatively nor afterthe patients were discharged. Eleven patients (17%)had hyperamylasemia during follow-up; however, allwere asymptomatic.The relationship between clinical variables and postoperativeinternal stent movement is shown tables 3-5.Univariate analysis revealed that pancreatic texture andClavien-Dindo classification ( ) differed significantlyaccording to stent fall time (p=0.019, 0.045, respectively),Clavien-Dindo classification ( ) differed significantlyaccording to the number of stent excretions (p=0.023).Additionally, patient sex, Clavien-Dindo classification( ), postoperative pancreatic fistula, and preoperativebiliary drainage differed significantly according tostent excretion time (p=0.014, 0.026, 0.024, 0.044,respectively).Multivariate analysis revealed that postoperativepancreatic fistula was an independent risk factor forstent excretion time (p=0.047; HR 0.513, 95%CI; 0.266-0.992), as shown table 6.

Table 2 - The postoperative movement of internal stentmean±SD, or n (%) Stent fall from the anastomotic site 58 (91%) Fall time (months) 4.9±2.0 Fall within one month 1 (2%) Fall within six months 42 (66%) Fall within one year 58 (91%) Dead without fall 1 (2%) Stent excretion from the body 53 (83%) Excretion time (months) 6.4±2.9 Excretion within one month 0 Excretion within six months 28 (44%) Excretion within one year 51 (80%) Dead without excretion 4 (6%) Stent migration into pancreatic duct 3 (5%) Stent migration into bile duct 3 (5%) Postoperative pancreatitis 0 Postoperative high serum amylase 11 (17%)

DISCUSSION
Pancreaticoduodenectomy is a standard procedurefor peri-ampullary tumors. However, postoperativemorbidity and mortality rates remain higher in pancreaticoduodenectomy(40%-45%, 1.6%-3.6%, respectively)than in other procedures (6-8). Pancreaticoentericanastomosis in pancreaticoduodenectomy includespancreaticojejunostomy and pancreaticogastrostomy.While pancreaticogastrostomy is associated with lowerrates of postoperative pancreatic fistula than pancreaticojejunostomy(9,10), pancreaticogastrostomy is associatedwith an increased risk of postoperative intraluminalhemorrhage (11). Thus, pancreaticojejunostomy iscommonly performed worldwide.A pancreatic duct stent is commonly used to bridgepancreaticoenteric anastomosis because it diverts pancreaticjuice from the anastomosis site, decompressesthe remnant pancreas, and maintains the patency ofthe main pancreatic duct (12,13). Furthermore, pancreaticduct stents reduce the rate of postoperative pancreaticfistula (14-16). However, recent reports haveindicated that stenting and non-stenting methods arecomparable for preventing postoperative pancreatic fistula(17-19). Therefore, whether a pancreatic stentreduces postoperative pancreatic fistula remains controversial.Moreover, an internal stent is believed to bemore useful than an external stent because hospitalstay is shorter with use of former than latter. This isbecause the occurrence of injury during external stentremoval is sometimes related to pancreatitis or lateonsetstenosis of the pancreatic duct (1,20-22).Moreover, some stent-related complications(including small bowel perforation, cholangitis, liverabscess, pancreatitis, and osteomyelitis) are due toenterospinal fistula (12,13,23-26). For example, areport of death due to multiple organ failure followingbiliary obstruction was related to stent migration into the bile duct (13). Additionally, some reports describesmall bowel perforation due to pancreatic stents, oneof which occurred 19 years postoperatively (12,26).Therefore, long-term follow-up is necessary for patientswhose stents have not been excreted from the body.In our study, there were no stent-related complications.High serum amylase levels were found in 11patients (17%) postoperatively, but all patients wereasymptomatic. Therefore, the internal stented methodis considered safe.
Similarly, Yoshimi et al. reported that internal stentswere excreted in all patients by postoperative day 176(1). Moreover, Kadowaki et al. reported that stent fallrate was 75% with a mean fall time of 13.1 months,excretion rate was 61% with a mean excretion of 15months, and 41% of the stents were excreted withinone year (13). In comparison, our patients had a meanfall time of 4.9 months, and mean stent excretion timeof 6.4 months. Within one year, 91% of stents fell fromthe anastomotic site, and 80% of stents were excreted from the body. Multivariate analysis showed that thestent excretion time was significantly delayed in patientswith grade B/C postoperative pancreatic fistula. Webelieve this is because pancreatic fistula may enhanceintra-abdominal adhesion and reduce intestinalperistalsis due to inflammation.Furthermore, Kadowaki et al. reported that thestent migration rates into the remnant pancreas andbile duct were 18.6% and 7.0%, respectively (13). Inother reports, the migration rate into the bile duct wasbetween 1.4% and 16.8 % (23,24). In our study, themigration rates into the pancreas and bile duct wereboth 5%. However, because stent length, thread type,and evaluation period differed between our study andprevious studies, an exact comparison was difficult.We used CT images to evaluate stent fall andexcretion. However, as there is a time lag between CTimaging and confirmation of stent fall or excretion, theexact fall and excretion time remain unclear.Nonetheless, we show that internal stents are safe.However, there are some patients whose stentsremained fixed at the anastomotic site and migrate intothe remnant pancreas; therefore, careful follow-up isnecessary. Considering the risk of stent-relatedcomplications, no stented method is desirable, and thedevelopment of a bioabsorbable stent is expected.

CONCLUSION
We observed the safe removal and excretion of internalstents from patients who underwent pancreaticoduodenectomy.Additionally, patients with postoperativepancreatic fistula had significantly later stent excretiontime.
Acknowlegement
We would like to thank Editage (www.editage.com)for English language editing.
Disclosure statement
The authors have no conflicts of interest to declosure.
Ethical approval
This study was conducted in accordance with theDeclaration of Helsinki and ethical guidelines for clinicalstudy in Japan under approval of the institutionalreview board of Katsushika Medical Center JikeiUniversity. The approval number is 30-322(9343).
REFERENCES
1 Yoshimi F, Ono H, Asato Y, Ohta T, Koizumi S, Amemiya R, et al.Internal stenting of the hepaticojejunostomy and pancreaticojejunostomyin patients undergoing pancreaticoduodenectomy topromote earlier discharge from hospital. Surg Today. 1996;26(8):665-7.
2 Child CG. Pancreaticojejunostomy and other problems associatedwith the surgical management of carcinoma involving the head ofthe pancreas. Report of five additional cases of radical pancreaticoduodenectomy.Ann Surg. 1944;119(6):845-55.
3 Kleespies A, Rentsch M, Seeliger H, Albertsmeier M, Jauch KW,Bruns CJ. Blumgart anastomosis for pancreaticojejunostomyminimizes severe complications after pancreatic head resection. BrJ Surg. 2009; 97(7):741-50.
4 Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M,et al. The 2016 update of the International Study Group (ISGPF)definition and grading of postoperative pancreatic fistula: 11 yearsafter. Surgery. 2017;161(3):584-91.
5 Dindo D, Demartines N, Clavien PA. Classification of surgicalcomplication: a new proposal with evaluation in a cohort of 6336patients and results of a survey. Ann Surg. 2004;240(2):205-13.
6 Kimura W, Miyata H, Gotoh M, Hirai I, Kenjo A, Kitagawa Y, et al. Apancreaticoduodenectomy risk model derived from 8575 casesfrom a single-race population (Japanese) using a web-based dataentry system: Ann Surg. 2014;259(4):773-80.
7 Narayanan S, Martin A, Turrentine FE, Bauer TW, Adams RB,Zaydfudim VM. Mortality after pancreaticoduodenectomy: assessingearly and late causes of patient death. J Surg Res. 2018;231:304-8.
8 Cameron JL, He J. Two thousand consecutive pancreaticoduodenectomies.J Am Coll Surg. 2015;220(4):530-6.
9 Menahem B, Guittet L, Mulliri A, Alves A, Lubrano J. Pancreaticogastrostomyis superior to pancreaticojejunostomy for prevention ofpancreatic fistula after pancreaticoduodenectomy: an updated metaanalysisof randomized controlled trials. Ann Surg. 2015;261(5):882-7.
10 Ricci C, Casadei R, Taffurelli G, Pacilio CA, Beltrami D, Minni F.Is pancreaticogastrostomy safer than pancreaticojejunostomyafter pancreaticoduodenectomy? A meta-regression analysis ofrandomized clinical trials. Pancreatology. 2017; 17(5): 805-13.
11 Lyu Y, Li T, Cheng Y, Wang B, Chen L, Zhao S. Pancreaticojejunostomyversus pancreaticogastrostomy after pancreaticoduodenectomy:An up-to-date meta-analysis of RCTs applying the ISGPF(2016) criteria. Surg Laparosc Endosc Percutan Tech. 2018;28(3):139-46.
12 Ortega PM, Zozaya-Larequi G, Arredondo J, Martí-Cruchaga P,Bellver M, Sánchez-Justicia C, et al. Distal migration of a transanastomoticpancreatic stent resulting in bowel perforation 19 yearsafter pancreaticoduodenectomy: report of a case. Surg Today. 2015;45(3):374-7.
13 Kadowaki S, Miura F, Amano H, Toyota N, Wada K, Shibuya M, et al.Whereabouts of an internal short stent placed across the pancreaticojejunostomyfollowing pancreaticoduodenectomy. J HepatobiliaryPancreat Sci. 2012;19(5):566-77.
14 Poon RT, Fan ST, Lo CM, Ng KK, Yuen WK, Yeung C, et al. Externaldrainage of pancreatic duct with a stent to reduce leakage rate ofpancreaticojejunostomy after pancreaticoduodenectomy: a prospectiverandomized trial. Ann Surg. 2007;246(3):425-33.
15 Wang Q, He XR, Tian JH, Yang KH. Pancreatic duct stents atpancreaticoduodenectomy: a meta-analysis. Dig Surg. 2013;30(4-6):415-24.
16 Motoi F, Egawa S, Rikiyama T, Katayose Y, Unno M. Randomizedclinical trial of stent drainage of the pancreatic duct to reduce postoperativepancreatic fistula after pancreaticojejunostomy. Br J Surg.2012;99(4):524-31.
17 Satoi S, Toyokawa H, Yanagimoto H, Yamamoto T, Hirooka S, Yui R,et al. Is a nonstented duct-to-mucosa anastomosis using the modifiedKakita method a safe procedure? Pancreas. 2010;39(2):165-70.
18 Usuba T, Misawa T, Ito R, Yoshida K, Hanyu N, Yanaga K. Safetyof non-stented pancreaticojejunostomy in pancreaticoduodenectomyfor patients with soft pancreas. Anticancer Res. 2016; 36(12):6619-23..
19 Xiong JJ, Altaf K, Mukherjee R, Huang W, Hu WM, Li A, et al.Systematic review and meta-analysis of outcomes after intraoperativepancreatic duct stent placement during pancreaticoduodenectomy.Br J Surg. 2012;99(8):1050-61..
20 Tani M, Kawai M, Hirono S, Ina S, Miyazawa M, Shimizu A, et al.A prospective randomized controlled trial of internal versusexternal drainage with pancreaticojejunostomy for pancreaticoduodenectomy.Am J Surg. 2010;199(6):759-64..
21 Kamoda Y, Fujino Y, Matsumoto I, Shinzeki M, Sakai T, Kuroda Y.Usefulness of performing a pancreaticojejunostomy with an internalstent after a pancreaticoduodenectomy. Surg Today. 2008;38(6):524-8..
22 Jang JY, Chang YR, Choi SH, Park SJ, Lee SE, Lim CS, et al.Randomized multicenter trial comparing external and internalpancreatic stenting during pancreaticoduodenectomy. Br J Surg.2016;103(6):668-75..
23 Hirono S, Kawai M, Yamashita Y, Okada K, Miyazaki M, Ueno M, etal. Successful removal of an internal pancreatic stent thatmigrated into the bile duct using double-balloon enteroscopy afterpancreaticoduodenectomy. Surg Today. 2018;48(2):167-74..
24 Park SH, Kim JH, Noh SY, Byun JH, Lee SS, Kim HJ, et al. Migrationof internal pancreaticojejunostomy stents into the bile ducts inpatients undergoing pancreaticoduodenectomy. J Gastrointest Surg.2015;19(11):1995-2002..
25 Munis A, Solomon B, Mazulis A, Laurie T. Osteomyelitis as a resultof pancreaticojejunostomy stent migration after Whipple procedure.ACG Case Rep J. 2018;5:e67..
26 Mari G, Costanzi A, Monzio N, Miranda A, Rigamonti L, Crippa J,et al. Small bowel perforation caused by pancreaticojejunalanastomotic stent migration after pancreaticoduodenectomy forperiampullary carcinoma. JOP. 2015;16(2):185-8.
Full Text Sources:
Abstract:
Views: 4135

Purposes: This study aimed to investigate the postoperative movement of an internal stentplaced at the anastomotic site of pancreaticojejunostomy during pancreaticoduodenectomy.
Methods: Of the 70 patients who underwent pancreaticoduodenectomy using an internalstent at the anastomotic site of pancreaticojejunostomy between January 2014 andDecember 2019, 64 patients (91%) were included in this study. Stent fall from the anastomoticsite, stent excretion from the body, and stent migration into the pancreatic and bileduct, as well as stent-related complications were examined.
Results: The stent fall rate and excretion rate were 91% and 83%, respectively. Furthermore,migration rates into the pancreatic duct and bile duct were 5% each. There were nostent-related complications. Univariate analysis revealed that pancreatic texture and Clavien-Dindo classification differed significantly according to stent fall time (p=0.019, 0.045,respectively). Moreover, the Clavien-Dindo classification differed significantly according tothe number of stent excretions (p=0.023). Additionally, patient sex, Clavien-Dindo classification,postoperative pancreatic fistula, and preoperative biliary drainage differed significantlyaccording to stent excretion time (p=0.014, 0.026, 0.024, 0.044, respectively). Multivariateanalysis revealed that postoperative pancreatic fistula was an independent risk factor forexcretion time (p=0.047; HR 0.513, 95%CI; 0.266-0.992).
Conclusions: We observed the safe removal and excretion of internal stents from patientswho underwent pancreaticoduodenectomy. Additionally, patients with postoperative pancreaticfistula had significantly later stent excretion time.Key words: internal stent, pancreaticoduodenectomy, pancreaticojejunostomy
INTRODUCTION
A pancreatic duct stent is often placed at the anastomotic site ofpancreaticojejunostomy during pancreaticoduodenectomy. Two types ofpancreatic duct stents exist internal and external. An internal stent is used with the theory that it falls from the anastomotic siteand is excreted spontaneously from the body becauseit is fixed with absorbent threads (1). However, it isunclear when the stent fall and excretion occur.Thus, we retrospectively examined the postoperativemovement of an internal stent placed at the anastomoticsite of pancreaticojejunostomy during pancreaticoduodenectomy.
METHODS
Patients and procedures
Between January 2014 and December 2019, 70patients underwent pancreaticoduodenectomy atKatsushika Medical Center The Jikei University, using aninternal stent at the anastomotic site of pancreaticojejunostomy.Of these, 64 patients (91%) were includedin this study as they could be followed-up for oversix months. Sub-stomach preserving pancreaticoduodenectomyand conventional pancreaticoduodenectomywere performed in 60 and 4 patients(94% and 4%), respectively. Reconstruction consistedof an end-to-side pancreaticojejunostomy, an endto-side hepaticojejunostomy, and an antecolic endto-side gastrojejunostomy according to Child’sprocedure (2). Duct-to-mucosa anastomosis ofpancreaticojejuno-stomy was performed with polydioxanonesutures (5-0 PDS PLUS®; Ethicon), followinga pancreatic parenchymal-jejunal seromuscularanastomosis with polypropylene sutures (3-0 PROLENE®; Ethicon) using the modified Blumgartmethod (3). The pancreatic duct stent was apolyvinyl catheter (MD-41515 pancreatic duct tube;Sumitomo Bakelite, Japan) with multiple side holesand a small knot. Using an internal stented method,a pancreatic duct stent was cut 4 cm in length andwas positioned with one half in the main pancreaticduct and the other half in the jejunal lumen. Thestent was fixed at the anastomotic site using thedorsal thread of the pancreaticojejunostomy. Thebile duct stent in hepaticojejunostomy was notroutinely used. The closed drains were placed nearthe sites of the pancreaticojejunal and hepaticojejunalanastomoses, and were promptly removedafter confirming the absence of intra-abdominalcomplications. All patients were administeredprophylactic antibiotics for at least three days postoperatively,postoperative prophylactic octreotidewas not routinely used. Food intake started threedays postoperatively after confirming the absence ofintra-abdominal complications.
Evaluation
We routinely performed abdominal computedtomography (CT) seven days postoperatively. After thepatient was discharged, a follow-up CT was performedevery three or four months. The fall of the stent fromthe anastomotic site of the pancreaticojejunostomyand excretion of the stent from the body wereconfirmed by CT examination. Serum amylase levelsand drainage fluid volume were measured on postoperativedays 1, 3, and 5. Postoperative pancreaticfistula was defined according to the International StudyGroup on Pancreatic Fistula (ISGPF) (4). The severity ofother early complications was categorized according tothe Clavien-Dindo classification (5). This study wasapproved by the Ethics Committee of the JikeiUniversity School of Medicine. The approval number is30-322(9343).
Statistical analysis
Univariate analyses were performed using theMann-Whitney U-test or Chi-square test. Multivariateanalyses were performed using a logistic regressionanalysis. All data were analyzed using JMP Pro version12 (SAS Institute Inc.). Statistical significance was set atp<0.05, and data are expressed as mean ± standarddeviation.
RESULTS
Patient characteristics and operative variables areshown in table 1. The mean postoperative follow-upperiod was 24.1 ± 15.3 months (6-69). There were 42males (66%) and 22 females (34%), mean age=68.9 ±11.3 (31-87); mean body mass index=22.2 ± 4.2 kg/m2(15.2-33.3). The primary diseases were pancreaticcarcinoma (n=21, 33%), bile duct carcinoma (n=18,28%), intraductal papillary mucinous neoplasm (n=10,16%), duodenal carcinoma (n=5, 8%), ampulla of Vatercarcinoma (n=3, 5%), transverse colon carcinoma withduodenal invasion (n=2, 3%), neuroendocrine tumor(n=2, 3%), chronic pancreatitis (n=1, 2%), mucinous cystneoplasm (n=1, 2%) and pancreatic duct adenoma(n=1, 2%). Forty-three patients (67%) had comorbidities,including hypertension (n=39, 61%), diabetes mellitus(n=18, 28%), hyperlipidemia (n=16, 25%), ischemic heartdisease (n=7, 11%), and respiratory disease (n=1, 2%).The mean diameter of the main pancreatic duct was2.7±1.8 mm (1-10). The pancreatic texture was soft andhard in 24 and 40 patients (38% and 62%), respectively.The stent size was 5, 6, and 7.5 Fr in 48, 13, and 3 patients (75%, 20% and 5%), respectively. The numberof duct-to-mucosa anastomosis sutures was four in 34patients (53%), five in 1 patient (2%), six in 1 patient(2%), eight in 24 patients, ten in 3 patients (5%), andtwelve in 1 patient (2%). The mean operation time was449 ± 70 min (294-616), and the mean intraoperativeblood loss was 1,043 ± 750 mL (222-3,862). Transfusionwas performed in 12 patients (19%), portal veinresection in 7 patients (11%), and preoperative biliarydrainage in 38 patients (59%). The morbidity andmortality rates were 44% and 0%, respectively. Clavien-Dindo classification ( ) and postoperative pancreaticfistula (Grade B/C) occurred in 18 and 13 patients (28%and 20%), respectively. Reoperations were performedin 3 patients (5%) due to necrosis of the transversecolon, perforation of the transverse colon and internalhernia. The mean postoperative hospital stay was 25.2± 16.9 days (9-93). Postoperative movement of thestent is shown in table 2. The stent fell from the anastomoticsite in 58 patients (91%), while the stentremained in the anastomotic site in 6 patients (9%), one of whom died. The shortest stent fall time was on postoperativeday seven, and the stent fell within one yearin all patients. The mean stent fall time was 4.9 ± 2.0months. The stent was excreted from the bodies of 53patients (83%), while the stent remained in 11 patients(17%), four of whom died without excretion. The meanexcretion time was 6.4 ± 2.9 months. Meanwhile, stentswere excreted within six months and one year postoperativelyfrom 28 and 50 patients (44% and 78%),respectively. Stent migration into the pancreas occurredin 3 patients (5%): One had a stent that was spontaneouslyexcreted, one remained with a migrated stent,and one died with a migrated stent. Stent migrationinto the bile duct occurred in 3 patients (5%), all ofwhom subsequently were excreted spontaneously.There were neither stent-related complications (such aspancreatitis and cholangitis) postoperatively nor afterthe patients were discharged. Eleven patients (17%)had hyperamylasemia during follow-up; however, allwere asymptomatic.The relationship between clinical variables and postoperativeinternal stent movement is shown tables 3-5.Univariate analysis revealed that pancreatic texture andClavien-Dindo classification ( ) differed significantlyaccording to stent fall time (p=0.019, 0.045, respectively),Clavien-Dindo classification ( ) differed significantlyaccording to the number of stent excretions (p=0.023).Additionally, patient sex, Clavien-Dindo classification( ), postoperative pancreatic fistula, and preoperativebiliary drainage differed significantly according tostent excretion time (p=0.014, 0.026, 0.024, 0.044,respectively).Multivariate analysis revealed that postoperativepancreatic fistula was an independent risk factor forstent excretion time (p=0.047; HR 0.513, 95%CI; 0.266-0.992), as shown table 6.
Table 2 - The postoperative movement of internal stent
DISCUSSION
Pancreaticoduodenectomy is a standard procedurefor peri-ampullary tumors. However, postoperativemorbidity and mortality rates remain higher in pancreaticoduodenectomy(40%-45%, 1.6%-3.6%, respectively)than in other procedures (6-8). Pancreaticoentericanastomosis in pancreaticoduodenectomy includespancreaticojejunostomy and pancreaticogastrostomy.While pancreaticogastrostomy is associated with lowerrates of postoperative pancreatic fistula than pancreaticojejunostomy(9,10), pancreaticogastrostomy is associatedwith an increased risk of postoperative intraluminalhemorrhage (11). Thus, pancreaticojejunostomy iscommonly performed worldwide.A pancreatic duct stent is commonly used to bridgepancreaticoenteric anastomosis because it diverts pancreaticjuice from the anastomosis site, decompressesthe remnant pancreas, and maintains the patency ofthe main pancreatic duct (12,13). Furthermore, pancreaticduct stents reduce the rate of postoperative pancreaticfistula (14-16). However, recent reports haveindicated that stenting and non-stenting methods arecomparable for preventing postoperative pancreatic fistula(17-19). Therefore, whether a pancreatic stentreduces postoperative pancreatic fistula remains controversial.Moreover, an internal stent is believed to bemore useful than an external stent because hospitalstay is shorter with use of former than latter. This isbecause the occurrence of injury during external stentremoval is sometimes related to pancreatitis or lateonsetstenosis of the pancreatic duct (1,20-22).Moreover, some stent-related complications(including small bowel perforation, cholangitis, liverabscess, pancreatitis, and osteomyelitis) are due toenterospinal fistula (12,13,23-26). For example, areport of death due to multiple organ failure followingbiliary obstruction was related to stent migration into the bile duct (13). Additionally, some reports describesmall bowel perforation due to pancreatic stents, oneof which occurred 19 years postoperatively (12,26).Therefore, long-term follow-up is necessary for patientswhose stents have not been excreted from the body.In our study, there were no stent-related complications.High serum amylase levels were found in 11patients (17%) postoperatively, but all patients wereasymptomatic. Therefore, the internal stented methodis considered safe.
Similarly, Yoshimi et al. reported that internal stentswere excreted in all patients by postoperative day 176(1). Moreover, Kadowaki et al. reported that stent fallrate was 75% with a mean fall time of 13.1 months,excretion rate was 61% with a mean excretion of 15months, and 41% of the stents were excreted withinone year (13). In comparison, our patients had a meanfall time of 4.9 months, and mean stent excretion timeof 6.4 months. Within one year, 91% of stents fell fromthe anastomotic site, and 80% of stents were excreted from the body. Multivariate analysis showed that thestent excretion time was significantly delayed in patientswith grade B/C postoperative pancreatic fistula. Webelieve this is because pancreatic fistula may enhanceintra-abdominal adhesion and reduce intestinalperistalsis due to inflammation.Furthermore, Kadowaki et al. reported that thestent migration rates into the remnant pancreas andbile duct were 18.6% and 7.0%, respectively (13). Inother reports, the migration rate into the bile duct wasbetween 1.4% and 16.8 % (23,24). In our study, themigration rates into the pancreas and bile duct wereboth 5%. However, because stent length, thread type,and evaluation period differed between our study andprevious studies, an exact comparison was difficult.We used CT images to evaluate stent fall andexcretion. However, as there is a time lag between CTimaging and confirmation of stent fall or excretion, theexact fall and excretion time remain unclear.Nonetheless, we show that internal stents are safe.However, there are some patients whose stentsremained fixed at the anastomotic site and migrate intothe remnant pancreas; therefore, careful follow-up isnecessary. Considering the risk of stent-relatedcomplications, no stented method is desirable, and thedevelopment of a bioabsorbable stent is expected.
CONCLUSION
We observed the safe removal and excretion of internalstents from patients who underwent pancreaticoduodenectomy.Additionally, patients with postoperativepancreatic fistula had significantly later stent excretiontime.
Acknowlegement
We would like to thank Editage (www.editage.com)for English language editing.
Disclosure statement
The authors have no conflicts of interest to declosure.
Ethical approval
This study was conducted in accordance with theDeclaration of Helsinki and ethical guidelines for clinicalstudy in Japan under approval of the institutionalreview board of Katsushika Medical Center JikeiUniversity. The approval number is 30-322(9343).
REFERENCES
1 Yoshimi F, Ono H, Asato Y, Ohta T, Koizumi S, Amemiya R, et al.Internal stenting of the hepaticojejunostomy and pancreaticojejunostomyin patients undergoing pancreaticoduodenectomy topromote earlier discharge from hospital. Surg Today. 1996;26(8):665-7.
2 Child CG. Pancreaticojejunostomy and other problems associatedwith the surgical management of carcinoma involving the head ofthe pancreas. Report of five additional cases of radical pancreaticoduodenectomy.Ann Surg. 1944;119(6):845-55.
3 Kleespies A, Rentsch M, Seeliger H, Albertsmeier M, Jauch KW,Bruns CJ. Blumgart anastomosis for pancreaticojejunostomyminimizes severe complications after pancreatic head resection. BrJ Surg. 2009; 97(7):741-50.
4 Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M,et al. The 2016 update of the International Study Group (ISGPF)definition and grading of postoperative pancreatic fistula: 11 yearsafter. Surgery. 2017;161(3):584-91.
5 Dindo D, Demartines N, Clavien PA. Classification of surgicalcomplication: a new proposal with evaluation in a cohort of 6336patients and results of a survey. Ann Surg. 2004;240(2):205-13.
6 Kimura W, Miyata H, Gotoh M, Hirai I, Kenjo A, Kitagawa Y, et al. Apancreaticoduodenectomy risk model derived from 8575 casesfrom a single-race population (Japanese) using a web-based dataentry system: Ann Surg. 2014;259(4):773-80.
7 Narayanan S, Martin A, Turrentine FE, Bauer TW, Adams RB,Zaydfudim VM. Mortality after pancreaticoduodenectomy: assessingearly and late causes of patient death. J Surg Res. 2018;231:304-8.
8 Cameron JL, He J. Two thousand consecutive pancreaticoduodenectomies.J Am Coll Surg. 2015;220(4):530-6.
9 Menahem B, Guittet L, Mulliri A, Alves A, Lubrano J. Pancreaticogastrostomyis superior to pancreaticojejunostomy for prevention ofpancreatic fistula after pancreaticoduodenectomy: an updated metaanalysisof randomized controlled trials. Ann Surg. 2015;261(5):882-7.
10 Ricci C, Casadei R, Taffurelli G, Pacilio CA, Beltrami D, Minni F.Is pancreaticogastrostomy safer than pancreaticojejunostomyafter pancreaticoduodenectomy? A meta-regression analysis ofrandomized clinical trials. Pancreatology. 2017; 17(5): 805-13.
11 Lyu Y, Li T, Cheng Y, Wang B, Chen L, Zhao S. Pancreaticojejunostomyversus pancreaticogastrostomy after pancreaticoduodenectomy:An up-to-date meta-analysis of RCTs applying the ISGPF(2016) criteria. Surg Laparosc Endosc Percutan Tech. 2018;28(3):139-46.
12 Ortega PM, Zozaya-Larequi G, Arredondo J, Martí-Cruchaga P,Bellver M, Sánchez-Justicia C, et al. Distal migration of a transanastomoticpancreatic stent resulting in bowel perforation 19 yearsafter pancreaticoduodenectomy: report of a case. Surg Today. 2015;45(3):374-7.
13 Kadowaki S, Miura F, Amano H, Toyota N, Wada K, Shibuya M, et al.Whereabouts of an internal short stent placed across the pancreaticojejunostomyfollowing pancreaticoduodenectomy. J HepatobiliaryPancreat Sci. 2012;19(5):566-77.
14 Poon RT, Fan ST, Lo CM, Ng KK, Yuen WK, Yeung C, et al. Externaldrainage of pancreatic duct with a stent to reduce leakage rate ofpancreaticojejunostomy after pancreaticoduodenectomy: a prospectiverandomized trial. Ann Surg. 2007;246(3):425-33.
15 Wang Q, He XR, Tian JH, Yang KH. Pancreatic duct stents atpancreaticoduodenectomy: a meta-analysis. Dig Surg. 2013;30(4-6):415-24.
16 Motoi F, Egawa S, Rikiyama T, Katayose Y, Unno M. Randomizedclinical trial of stent drainage of the pancreatic duct to reduce postoperativepancreatic fistula after pancreaticojejunostomy. Br J Surg.2012;99(4):524-31.
17 Satoi S, Toyokawa H, Yanagimoto H, Yamamoto T, Hirooka S, Yui R,et al. Is a nonstented duct-to-mucosa anastomosis using the modifiedKakita method a safe procedure? Pancreas. 2010;39(2):165-70.
18 Usuba T, Misawa T, Ito R, Yoshida K, Hanyu N, Yanaga K. Safetyof non-stented pancreaticojejunostomy in pancreaticoduodenectomyfor patients with soft pancreas. Anticancer Res. 2016; 36(12):6619-23..
19 Xiong JJ, Altaf K, Mukherjee R, Huang W, Hu WM, Li A, et al.Systematic review and meta-analysis of outcomes after intraoperativepancreatic duct stent placement during pancreaticoduodenectomy.Br J Surg. 2012;99(8):1050-61..
20 Tani M, Kawai M, Hirono S, Ina S, Miyazawa M, Shimizu A, et al.A prospective randomized controlled trial of internal versusexternal drainage with pancreaticojejunostomy for pancreaticoduodenectomy.Am J Surg. 2010;199(6):759-64..
21 Kamoda Y, Fujino Y, Matsumoto I, Shinzeki M, Sakai T, Kuroda Y.Usefulness of performing a pancreaticojejunostomy with an internalstent after a pancreaticoduodenectomy. Surg Today. 2008;38(6):524-8..
22 Jang JY, Chang YR, Choi SH, Park SJ, Lee SE, Lim CS, et al.Randomized multicenter trial comparing external and internalpancreatic stenting during pancreaticoduodenectomy. Br J Surg.2016;103(6):668-75..
23 Hirono S, Kawai M, Yamashita Y, Okada K, Miyazaki M, Ueno M, etal. Successful removal of an internal pancreatic stent thatmigrated into the bile duct using double-balloon enteroscopy afterpancreaticoduodenectomy. Surg Today. 2018;48(2):167-74..
24 Park SH, Kim JH, Noh SY, Byun JH, Lee SS, Kim HJ, et al. Migrationof internal pancreaticojejunostomy stents into the bile ducts inpatients undergoing pancreaticoduodenectomy. J Gastrointest Surg.2015;19(11):1995-2002..
25 Munis A, Solomon B, Mazulis A, Laurie T. Osteomyelitis as a resultof pancreaticojejunostomy stent migration after Whipple procedure.ACG Case Rep J. 2018;5:e67..
26 Mari G, Costanzi A, Monzio N, Miranda A, Rigamonti L, Crippa J,et al. Small bowel perforation caused by pancreaticojejunalanastomotic stent migration after pancreaticoduodenectomy forperiampullary carcinoma. JOP. 2015;16(2):185-8.
Full Text Sources:
Abstract:
Views: 4135
Watch Video Articles
For Authors
Journal Subscriptions

Current Issue
Dec 2025
Supplements
Instructions for authors
Online submission
Contact
ISSN: 2559 - 723X (print)
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Open Access Statement
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Journal Metrics
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.