Surgery, Gastroenterology and Oncology

|
|
Objective: Patients with acute diverticulitis (AD) have an increased risk of underlying colorectal cancer (CRC), however those with uncomplicated AD may have the same underlying population risk. Despite evidence suggesting these patients may not require further endoscopy, published guidelines still recommended Colonoscopy as standard post-diverticulitis management. A practical approach to the definition of bowel wall thickening may improve negative predictability, a potential impediment to omitting colonoscopic followup.
Material and Methods: A 2-year (July 2016 – June 2018) retrospective study of patients admitted with CT confirmed acute diverticulitis was conducted. CT findings were categorised as ‘complicated’ or ‘uncomplicated’ and were correlated with the detection of cancer in subsequent Colonoscopy or follow-up. Bowel thickening was defined as any bowel thickening reported as such by the reporting Radiologist.
Results: Of a total of 431 patients, 67.7% (n=292) were seen to have had complicated AD on CT with complication features of bowel wall thickening (61.2%), perforation (13.7%), or an abscess (8.1%). Follow-up colonoscopic evaluation was conducted in 52.9% (n=228) of total cases of AD. Six patients were found to have colorectal cancer on Colonoscopy, all in complicated group although this was not statistically significant (p=0.18). Polyp detection rates were similar between groups. Radiologist-reported bowel wall thickening was a feature of all malignant diagnoses, and the only feature in 3 of the 6 patients.
Conclusion: The only CRC diagnoses were made in patients with complicated AD. There may be scope to safely decrease the number of Colonoscopies performed in AD patients and the use of Radiologist-reported bowel wall thickening may a practical improvement to local definitions of complicated diverticulitis.
INTRODUCTION
Acute diverticulitis (AD) accounts for a significant number of admissions in modern acute surgical units. Most of these admissions are for lower grade attacks (Hinchey grades 1 or 2) that often require conservative management (± antibiotics) or, at most, percutaneous drainage, and thus no histological confirmation of the diagnosis is made. As such, there is a high reliance on Computed Tomography (CT) to be confident of the diagnosis of AD rather than a perforated colorectal cancer (CRC). Many societies and guidelines recommend routine Colonoscopy following AD, citing a higher risk of underlying malignancy. However more recent literature raises the question as to whether this is appropriate or necessary for all AD patients (1-3). While the overall AD data supports there being an increased risk of CRC diagnosis in these patients, there may be low and high risk subsets that could allow some patients to forego screening Colonoscopy (4,5).
In Australia, colonoscopy access is getting increasingly more difficult with issues such as a blowout in waiting times with Covid-19, increasing uptake of the National Bowel Cancer Screening Programme (NBCSP), and an aging population. Australia and Aotearoa New Zealand have been labelled as the countries with the highest incidence of bowel cancer (6), hence the support and promotion of the NBCSP. A recent overhaul of Medicare billing numbers on Colonoscopy aims to decrease the number of inappropriately short interval surveillance Colonoscopies, in the hope that this helps alleviate pressure on the Colonoscopy waiting list (7). Thus, it is important to confirm a potential subset of AD patients that may not require a Colonoscopy, not only to decrease their individual management burden, but to decrease the delay for other patients who have a higher risk of CRC.
CT machines have continued to improve in quality and with a minimum of 64-slice scanner echnology now widely used, the fine detail visible has allowed certain CT signs to be used to define otential low risk categories. These signs include the presence or absence of free gas, abscess formation, fistula, obstruction, stricture, and irregular bowel wall thickening. Using these criteria, the proportion of patients considered high risk may range between 7- 38% (8,9). Perhaps the vast reduction in patients recommended for Colonoscopy, and the risk of even a low number of patients that could have a missed cancer has resulted in the lack of firm guidelines. There is also debate regarding the usefulness and inclusion of bowel wall thickening in the definition.
This study proposes using a practical definition of bowel wall thickening as reported by the reporting Radiologist to aid in the delineation of a high risk group that has a high sensitivity, giving the clinician more confidence that omitting Colonoscopy for low risk patients is safe. The aim of this study was to use this definition and elucidate if the presence of high risk CT signs led to an increased rate of CRC in an Australian single centre population and thus identify a local subset of patients for whom Colonoscopy could be safely foregone.
MATERIAL AND METHODS
This retrospective cohort study was conducted in a large metropolitan teaching hospital in Melbourne, Australia. A 2-year (July 2016 – June 2018) retrospective study of patients admitted with CT confirmed AD was conducted prior to the Covid-19 pandemic to allow for a 12 month follow up without the bias of the pandemic to confound the results. AD was categorised as ‘complicated’ and ‘uncomplicated’ with respect to certain CT features as reported by Consultant Radiologists. Complicated diverticulitis was defined by presence of at least one of the following features - wall thickening, abscess, perforation, fistula, obstruction, and stricture. Wall thickening was defined as positive identification and reporting of this by the reporting Radiologist. Perforation included localised/contained perforation and free/uncontained perforation.
Patient data was obtained from electronic patient records and analysed for demographics, relevant personal and family history, imaging, and endoscopic evaluation. Only those patients in whom a CT diagnosed AD were included. Colonoscopy reports were retrieved from hospital electronic records, including those performed elsewhere with imported results.
Presence of complicated and uncomplicated diverticulitis was correlated with the detection of neoplasia in subsequent Colonoscopy. The primary outcome measured was the incidence of colorectal malignancy on follow-up endoscopy. In addition, the diagnostic yield of Colonoscopy for advanced adenoma (AA) in diverticulitis was also determined. AA was defined as adenomas with size at least 10mm, histologically with at least 20-25% villosity and/or high grade dysplasia (10).
Descriptive statistics were prepared to summarize the overall cohort, and to compare complicated and uncomplicated AD. Differences between groups for categorical variables were assessed using chi-squared or Fishers Exact tests, while continuous variables were assessed using Student’s t-tests. Stata version 17.0 (StataCorp, College Station, Texas, USA) was used to conduct the statistical analysis with a p-value of less than 0.05 was considered to indicate statistical significance. Ethical approval was granted by the institutional Office of Research and Governance (ALR 37.2017).
RESULTS
A total of 431 patients were identified as having a clinically and CT diagnosed acute colonic diverticulitis. The mean age of patients was 58.7 years at time of diagnosis and there was an even gender distribution (table 1). In the majority of cases, AD was primarily located in the sigmoid colon. Approximately one-third (n = 139) of the total cases were uncomplicated, whereas two-thirds (n = 292) had complicated diverticulitis (fig. 1). Wall thickening was the most common finding in complicated diverticulitis, present in 90.4% of these patients. In contrast, 12% had an abscess and 20.2% had a perforation.
Figure 1 - Flow chart of patient identification and management

Table 1 - Demographics, n (%) unless otherwise indicated

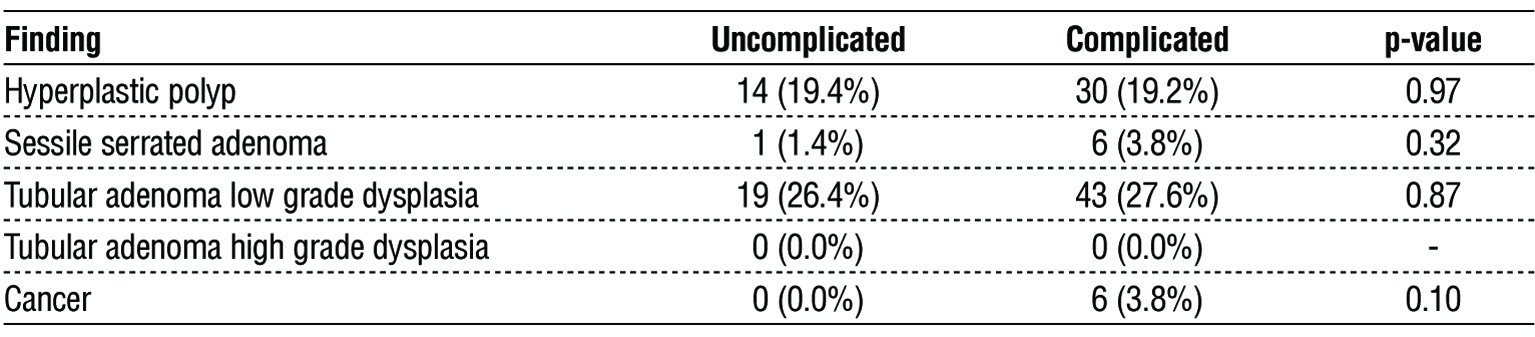
Of the 431 patients, 228 patients (52.9%) were known to have undergone endoscopic evaluation, within 1 year of their admission CT. The median time to Colonoscopy was 53.5 days (interquartile range, 35 to 126 days). 204 patients (89.5%) had a complete colonoscopic evaluation to the caecum, and histological results are shown in table 2. There was no statistical difference between groups in relation to any of the histological diagnoses, although there was a trend towards higher sessile serrated adenomata and cancer diagnoses in the complicated diverticulitis group. Of note, 6 patients were found to have an invasive malignancy in the complicated diverticulitis group. No CRCs were found in the 72 patients of the uncomplicated diverticulitis group that underwent Colonoscopy.
Table 2 - Polyp detection and histological findings, n (%) unless otherwise indicated
All six cases of CRC detected on post-diverticulitis Colonoscopy (ie 6/228) were in the complicated diverticulitis group with specific features of these patients described in table 3. Of note, three patients were under 50 years old, and three patients were over 50 years old at the time of diagnosis; and five out of six patients were men.
Table 3 - Individual features of patients diagnosed with colorectal cancer

The reasons for no recorded Colonoscopy within 12 months of diagnosis of AD were recorded (table 4). A prior Colonoscopy (within 24 months), patient refusal and Colonoscopy done elsewhere were the most commonly documented reasons.
Table 4 - Reasons for lack of follow up colonoscopy

DISCUSSION
Patients admitted with diverticulitis may have an underlying CRC, which can simulate or be obscured by AD (11,12). The current gold standard of CT evaluation for diagnosis of diverticulitis may not conclusively distinguish it from cancer (13,14), forming the rationale for endoscopic evaluation. Multiple studies over the last two decades have investigated the yield of colonic evaluation after AD, resulting in heterogeneous conclusions (5,10,15). Multiple international guidelines recommend routine interval Colonoscopy after an episode of AD to exclude malignancy (16-18). Yet other international guidelines have challenged this recommendation and published conflicting advice (19), and others, such as the NICE guidelines, have conveniently ignored the issue although have approved the Royal College of Surgeons’ position of routine colonoscopy for all (20,21). More recent studies have suggested low risk groups, based on findings of complexity on CT, whereby routine Colonoscopy post-AD may be safely omitted, although in the case of the EAES and SAGES guidelines, there is acknowledgement that not all members will change their practice (4,5,9,22). This study has statistically failed to confirm such a group, however of note CRC was only found in patients with complicated AD, although almost half the patients did not undergo colonoscopic evaluation.
While the outcome of this study would suggest that all patients should still undergo routine Colonoscopy post-diverticulitis, the lack of statistical difference is likely confounded by a relatively small cohort of patients that underwent Colonoscopy. Simple power calculations using the results from this study, and with patients recruited into groups in a similar ratio, would suggest a sample size of over 500 patients undergoing Colonoscopy would be required to demonstrate a statistically significant result. While this may have potentially resulted in a type II error in detection rates, a review of comparable single centre studies with smaller or similar cohort sizes, some over longer periods, suggests relative credibility of results (23). The result of a 3.8% adenocarcinoma detection rate in the complicated group is still less than that reported by large population studies for Colonoscopies with other colorectal cancer risk symptoms which can be up to 4.1-5.1% (24,25). Thus, a higher powered study is still required to definitively answer the research question.
Wall thickening is a very common feature in AD and considered a high yield Colonoscopy indication (2). Although there is a lack of consensus on this being a true feature of complicated disease (26), it is notable that all CRC cases in this study were reported to have wall thickening on CT. Interestingly, 50% of these cases had no other complication factor reported on their CT scans. Multiple studies have considered various descriptions of concerning wall thickening, including irregular wall thickening (1), and wall thickening greater than 15 mm (3). With the continued improvement in definition with more modern CT scanners, perhaps it is not appropriate to have a size criterion which may become obsolete with time. With the lack of clarity on this issue, all patients with Radiologist-reported wall thickening were considered complicated diverticulitis for the purposes of this study rather than use a set size criterion, taking into account the highly honed skills of Radiologists with ever increasing improvement in the quality of scans. It, thus, relies on Radiologists reporting when they believe the thickening may be out of keeping with diverticulitis alone, and is worth mentioning. This created an easy and practical measure which is easily mass produced but may introduce bias depending on local Radiologist expertise and reporting standards. Furthermore, using this criteria appears to have drastically increased the proportion of patients considered complicated, with 67.7% of patients in this study considered so compared with literature figures of between 7- 38% (8, 9). Thus, the use of specific criteria such as wall thickening may have to be institution based rather than creating system wide rules across institutions, but doing so may include more patients requiring Colonoscopy and potentially increasing the safety window in an era when guidelines are still reticent to omit routine post-diverticulitis Colonoscopy. For those opposed to change, omitting Colonoscopy in a third of patients may seem more reasonable than omitting Colonoscopy for most patients. An inter-observer reliability study with Consultant Radiologists reporting on the size of bowel wall thickening and then comparing to the original report may further ascertain the accuracy and bias of using the subjective reporting of bowel wall thickening as we have suggested, and will be considered by our research group in the future.
A breakdown of positive Colonoscopies in complicated disease showed that among half of those with wall thickening that underwent endoscopic evaluation (141 of 264), 6 had cancer (4.2%). Other recognised features of complexity that have been linked to diverticulitis-mimicking CRC include diverticular perforation and abscess (3,4). These associations were replicated by this study, whereby 2 (5.1%) among 39 Colonoscopies in diverticular perforation harbored cancer. Of the complex criteria, a diverticular abscess was the highest risk feature with 3 (13.6%) among the 22 endoscopically evaluated abscess cases having an underlying cancer. Performing a Colonoscopy after diverticulitis which is complicated by perforation or abscess should remain mandatory.
Early detection of AA is also considered a major indication to perform Colonoscopy including in the AD population (27). Many recent studies found no statistical difference in AA detection rates between overall AD and the normal population (5,15). Other studies demonstrated equal rates in the uncomplicated AD subset and the normal population (10,22). Conversely, many studies cited a higher AA rate in complicated AD compared to uncomplicated AD and to normal population (8). A histological analysis of polyps in AD detected in this study revealed just over 3% to be AA, not far off from various recent literature reporting this to range from 3.9 – 10.6% in AD (4,8,10,23), and not significantly different to incidence of AA in normal population ranging from 3.28 – 7.7% (10,28). The data also highlighted an obvious, though statistically not significant, trend towards higher sessile serrated adenomata in complicated versus uncomplicated AD (n = 6 vs 1), in keeping with similar research as above. It is uncertain as to the pathophysiological connection between complicated AD and AA, however these comparisons are clearly worthwhile establishing to confirm the safety of excluding Colonoscopy in the uncomplicated cohort.
Of note, almost half of the patients identified in this study did not undergo Colonoscopy within 12 months of AD diagnosis. The highest group of these were patients who underwent Colonoscopy within the 24 months prior to diagnosis. This time period has been recommended in 2021 guidelines by the Victorian government through Safer Care Victoria (29). There is, however, no great evidence to support any particular time period which could be considered safe, and current guidelines would suggest 5 years is safe for standard surveillance Colonoscopy following a diagnosis and removal of a low grade adenoma. However, diverticular disease remains a known higher risk factor for missed/interval colon cancers(30). Future studies and guidelines may also like to explore additional features such as GP surveillance for ongoing symptoms, anaemia and/or with faecal occult blood tests in patients deemed suitable to omit Colonoscopy, for an added level of safety.
CONCLUSION
In conclusion, this study found no statistical difference in CRC detection between low and high risk groups based on CT findings, however it is notable that the only CRC diagnoses made were in patients with complicated AD and the possibility of a type II error is not excluded. Given the low diagnostic yield of Colonoscopy for advanced neoplasia in uncomplicated diverticulitis and considering the low but real risk of morbidity and mortality that invasive procedures carry, there may be scope to safely employ a more selective approach to Colonoscopy in uncomplicated diverticulitis. The novel use of Radiologist-reported bowel wall thickening may be a practical and useful positive predictive tool in the definition of complicated diverticulitis. This is also likely to help target colonoscopic resources to those at greatest risk of CRC.
Statements and Declarations
The paper is not based on any previous conference presentations. The authors have no financial or other competing interests to declare.
Contributions
Conceptualisation and Supervision RH; Ethics RH; Data collection DM and NS; Statistics MT; Analysis - all; Writing draft DM; Specialist opinion NS and RH; Editing and approval of final manuscript - all.
REFERENCES
1.Langenfeld SJ. Evaluation and Medical Management of Uncomplicated Diverticulitis. Clin Colon Rectal Surg. 2021;34(2):86-90.
2.Modi RS, Singh H, Patel N, Matin A, Ringold DA. Bowel Wall Thickening on CT Scan Is a High Yield Colonoscopy Indication. Clinical Gastroenterology and Hepatology. 2012;10(3):330-1.
3.Sallinen V, Mentula P, Leppaniemi A. Risk of colon cancer after computed tomography-diagnosed acute diverticulitis: is routine colonoscopy necessary? Surg Endosc. 2014;28(3):961-6.
4.Meyer J, Orci LA, Combescure C, Balaphas A, Morel P, Buchs NC, et al. Risk of Colorectal Cancer in Patients With Acute Diverticulitis: A Systematic Review and Meta-analysis of Observational Studies. Clin Gastroenterol Hepatol. 2019;17(8):1448-56 e17.
5.Rottier SJ, van Dijk ST, van Geloven AAW, Schreurs WH, Draaisma WA, van Enst WA, et al. Meta-analysis of the role of colonoscopy after an episode of left-sided acute diverticulitis. Br J Surg. 2019;106(8):988-97.
6.Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359-86.
7.Lee See M, Lee A, Roberts R, Friedman RA, Hewett DG, Worthley DL. The clinical value of "exception item" colonoscopy (MBS item 32228). Med J Aust. 2022;216(2):94-5.
8.Azizian JM, Trieu H, Kovacs TO, Turkiewicz J, Hilder R, Palmer S, et al. Yield of Post-Acute Diverticulitis Colonoscopy for Ruling Out Colorectal Cancer. Tech Innov Gastrointest Endosc. 2022;24(3):254-61.
9.de Vries HS, Boerma D, Timmer R, van Ramshorst B, Dieleman LA, van Westreenen HL. Routine colonoscopy is not required in uncomplicated diverticulitis: a systematic review. Surg Endosc. 2014;28(7):2039-47.
10.Tehranian S, Klinge M, Saul M, Morris M, Diergaarde B, Schoen RE. Prevalence of colorectal cancer and advanced adenoma in patients with acute diverticulitis: implications for follow-up colonoscopy. Gastrointest Endosc. 2020;91(3):634-40.
11.Koo CH, Chang JHE, Syn NL, Wee IJY, Mathew R. Systematic Review and Meta-analysis on Colorectal Cancer Findings on Colonic Evaluation After CT-Confirmed Acute Diverticulitis. Dis Colon Rectum. 2020;63(5):701-9.
12.Soh NYT, Chia DKA, Teo NZ, Ong CJM, Wijaya R. Prevalence of colorectal cancer in acute uncomplicated diverticulitis and the role of the interval colonoscopy. Int J Colorectal Dis. 2018;33(7):991-4.
13. Gryspeerdt S, Lefere P. Chronic diverticulitis vs. colorectal cancer: findings on CT colonography. Abdom Imaging. 2012; 37(6):1101-9.
14. Singh S, Shuttleworth J, Alagoda U, Giucca A, Heylen A, Browning N, et al. Differentiating Colorectal Carcinoma From Diverticulitis With Computerised Tomography: Does Every Patient Need Follow-Up Colonoscopy After an Episode of Acute Diverticulitis? Cureus. 2020;12(12):e12027.
15. Mari A, Khoury T, Sbeit W. Post-Diverticulitis Colonoscopy Was Not Associated with Higher Colonic Adenoma and Carcinoma: A Multicenter Case-Control Study. Medicina (Kaunas). 2021;57(7).
16. Stollman N, Smalley W, Hirano I, Committee AGAICG. American Gastroenterological Association Institute Guideline on the Management of Acute Diverticulitis. Gastroenterology. 2015;149(7):1944-9.
17. Schultz JK, Azhar N, Binda GA, Barbara G, Biondo S, Boermeester MA, et al. European Society of Coloproctology: guidelines for the management of diverticular disease of the colon. Colorectal Dis. 2020;22 Suppl 2(S2):5-28.
18. Vennix S, Morton DG, Hahnloser D, Lange JF, Bemelman WA, Research Committee of the European Society of C. Systematic review of evidence and consensus on diverticulitis: an analysis of national and international guidelines. Colorectal Dis. 2014; 16(11):866-78.
19. Sartelli M, Catena F, Ansaloni L, Coccolini F, Griffiths EA, Abu-Zidan FM, et al. WSES Guidelines for the management of acute left sided colonic diverticulitis in the emergency setting. World J Emerg Surg. 2016;11:37.
20. National Institute for Health and Care Excellence (NICE). Diverticular disease: diagnosis and management 2019 [NG147:[Available from: https://www.nice.org.uk/guidance/ng147/chapter/recommendations.
21. Royal College of Surgeons. Commissioning guide: Colonic diverticular disease 2014 [Updated March 2017:[Available from: https://www.rcseng.ac.uk/search/#SearchTerm=diverticulitis.
22. Daniels L, Unlu C, de Wijkerslooth TR, Stockmann HB, Kuipers EJ, Boermeester MA, et al. Yield of colonoscopy after recent CT-proven uncomplicated acute diverticulitis: a comparative cohort study. Surg Endosc. 2015;29(9):2605-13.
23. Cerdan Santacruz C, Muriel Alvarez P, Roig Ferreruela G, Merichal Resina M, Pinillos Somalo AI, Mestres Petit N, et al. Interval colonoscopy following acute diverticulitis should not be discouraged yet: results from a retrospective cohort. Surg Endosc. 2021;35(12):6819-26.
24. Mangas-Sanjuan C, Santana E, Cubiella J, Rodriguez-Camacho E, Seoane A, Alvarez-Gonzalez MA, et al. Variation in Colonoscopy Performance Measures According to Procedure Indication. Clin Gastroenterol Hepatol. 2020;18(5):1216-23 e2.
25. Barret M, Boustiere C, Canard J, Arpurt J, Bernardini D, Bulois P, et al. Société Française d'endoscopie Digestive: factors associated with adenoma detection rate and diagnosis of polyps and colorectal cancer during colonoscopy in France: results of a prospective, nationwide survey. PLoS One. 2013;8:e68947.
26. Onur MR, Akpinar E, Karaosmanoglu AD, Isayev C, Karcaaltincaba M. Diverticulitis: a comprehensive review with usual and unusual complications. Insights Imaging. 2017;8(1):19-27.
27. Leaning M, McSweeney W, Dastouri D. Will a flexi-sig' do? A retrospective review of colonoscopies indicated by diverticulitis alone. Surg Endosc. 2022;36(5):2949-53.
28. Dube C, Yakubu M, McCurdy BR, Lischka A, Kone A, Walker MJ, et al. Risk of Advanced Adenoma, Colorectal Cancer, and Colorectal Cancer Mortality in People With Low-Risk Adenomas at Baseline Colonoscopy: A Systematic Review and Meta-Analysis. Am J Gastroenterol. 2017;112(12):1790-801.
29. Safer Care Victoria. Diagnostic colonoscopy for assessment after CT- diagnosed diverticulitis [updated 08 February 2021. Available from: https://www.safercare.vic.gov.au/clinical-guidance/non-urgent-elective-surgery/diagnostic-colonoscopy-for-assessment-after-CT-diagnosed-diverticulitis.
30. Bressler B, Paszat LF, Chen Z, Rothwell DM, Vinden C, Rabeneck L. Rates of new or missed colorectal cancers after colonoscopy and their risk factors: a population-based analysis. Gastroenterology. 2007;132(1):96-102.
Full Text Sources:
Abstract:
Views: 16542

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.