Surgery, Gastroenterology and Oncology

|
|
Background: Spleen injury is the most common injury to the solid organ in the abdomen. Treatment changes in the last 100 years have been from splenectomy to splenic preservation to nonoperative management. Purpose: To evaluate predictive factors in the management of blunt splenic injuries.
Methods: This was a prospective study conducted in our hospital from December 2021 to December 2023, in which all patients with blunt splenic injuries were included. Patient outcomes, whether operative or conservative, were also recorded. Failure of conservative treatment was defined in our study as any patient managed surgically after 6 h of conservative management. All possible predictive factors were recorded and analyzed.
Results: The current study reviewed 88 patients with splenic injuries, with a mean age of 25 years. Nonoperative was the primary management in (54.4%) of patients, with a failure rate of 25%. Initial operative management associated with tachycardia (90.6%), hypotension (80.8%), injury severity score (ISS) >16 (96.2%), high AAST grade (61.6%), and extra-abdominal injuries (65.4%). On the other hand, the failure of nonoperative management associated with age less than 20 years (50%), female sex (66.7%), tachycardia (45.5%), hypotension (66.7%), ISS >16 P<0.001), high ASST grade P=0.001), and associated abdominal injury (66.7%).
Conclusion: Pedestrian injuries are the most common injury mechanism. A significant relationship exists between initial OM and hemodynamic instability, high ISS (>16), high-grade AAST (4,5), associated abdominal organ injury, and extra-abdominal injuries; however, GCS is not associated with their initial management type, whether operative or conservative. The factors related to FNOM include young age, female sex, hemodynamic instability, high-grade ASST, and associated abdominal injury, GCS, or extra-abdominal injury associated with NOM failure.
Introduction
Blunt abdominal trauma was reported in 6.2% of patients admitted to hospitals, 85% of them had solid organ injury, and splenic injury was reported in 33% of all abdominal injuries increasing in children with abdominal trauma to 44% (1).
Spleen is considered the most common solid organ injury in blunt abdominal trauma (2-4) although some studies have reported that the liver is the most commonly injured solid organ (1,5).
Until the middle of the 20th century, splenectomy was considered the standard treatment for splenic trauma, and after the discovery of the importance of the spleen for immune function and the risk of post-splenectomy infection (OPSI) in splenectomy patients, which carried a high mortality rate, the surgical practice shifted from splenectomy to splenic preservation surgery. In the 1980s, with the development of imaging techniques, nonoperative management (NOM) has gradually become the first option of treatment in hemodynamically stable patients with high success rates, decreasing rates of unnecessary laparotomies, and post-operative complications with preservation of splenic function (6-8). In 2003, the Eastern Association for the Surgery of Trauma (EAST) published guidelines for NOM of blunt splenic trauma (9), even though operative management (OM) is still the treatment of choice for hemodynamically unstable patients (10) or associated hollow viscus injury. Other factors that may affect the choice of treatment may include the grade of splenic trauma, injury severity score (ISS), and Glasgow Coma Scale (GCS) (11).
NOM may include either clinical observation or radiological intervention by angioembolization (AE), whereas OM may consist of either splenectomy or splenic preservation procedures (splenorrhaphy, partial splenectomy, and observation). Since then, many studies have discussed the role of NOM in treating blunt splenic trauma, and predictor factors in favor of NOM or OM.
The study aimed to evaluate predictor factors in the management of blunt splenic injury.
Methods
Study Design and Setting
This prospective study was carried out at a governmental Teaching Hospital from December 2021 to December 2023, where all patients with blunt splenic injuries were included.
Exclusion Criteria
1. Penetrating splenic injury;
2. All patients who died at the emergency unit;
3. Patients who present with delayed splenic rupture are the first to present with a lack of initial injury data;
4. Iatrogenic splenic injury.
Inclusion Criteria
Patients who met the inclusion criteria were reviewed for demographic information (sex, age), mechanism of injury, initial pulse rate (PR), systolic blood pressure (SPB), and shock index (SI) (PR ÷ SBP). ISS was calculated, and the grade of splenic injury was recorded for each patient depending on abdominal CT scan findings or operative findings (according to AAST: American Association for Surgery of Trauma grading for splenic trauma), GCS was recorded for each patient, and any associated abdominal injury or extra-abdominal injury.
Outcome and Follow-up
Patient outcomes, either OM or NOM (observation +resuscitation), were recorded. We followed each patient managed by NOM with at least every hour clinical examination with measurement of vital signs, measurement of hemoglobin, hematocrit, lactate, renal function test, and others including ultrasonography and repetition when necessary) failure of NOM (FNOM) was defined in our study as any patient managed by OM after 6 hours of NOM, types of OM (splenectomy, splenorrhaphy, observation) were recorded.
Ethical Approval
The scientific committee of the Department of Surgery, College of Medicine, Mustansiriya University (Reference number: 239, 26/5/2022).
Statistical Analysis
Data were entered, cleaned, and analyzed using SPSS version 26. The nominal variables are presented as frequencies and percentages, and the association between the dependent variables and other independent variables was determined using Pearson’s chi-square test and Fisher’s exact test, respectively. The numerical variables were tested for normality and presented as means with standard deviations and medians with interquartile ranges (25th–75th percentiles). A level of alpha of 5% or lower was considered significant.
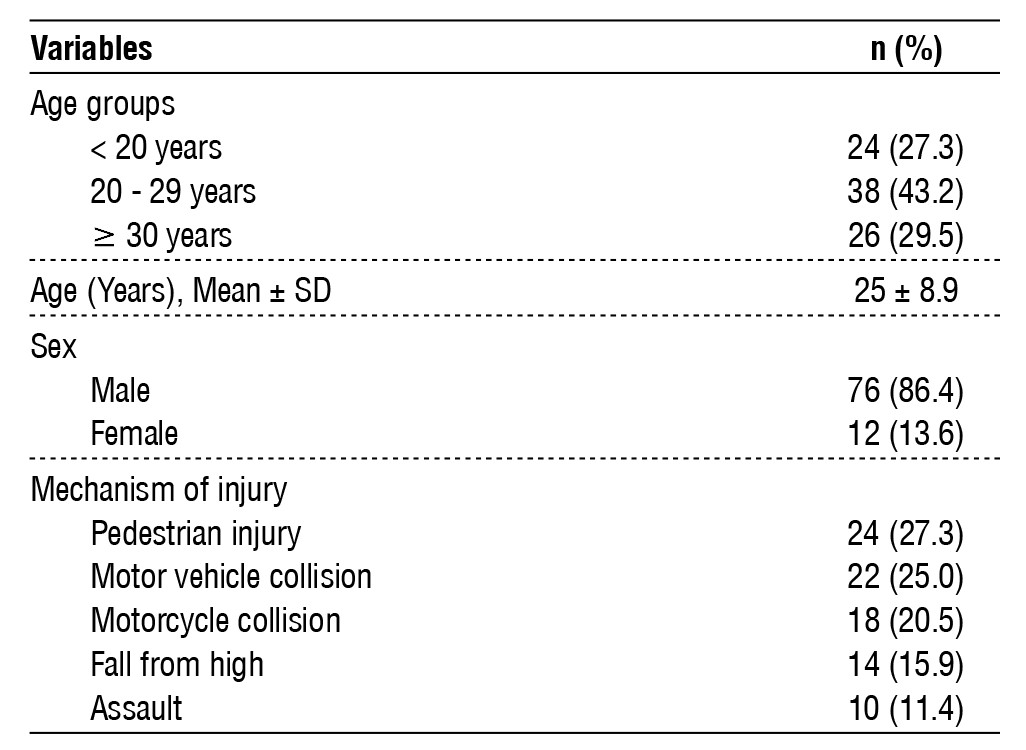
Table 1 - Demographics and mechanism of injury among the patients.
Results
The current study reviewed 88 patients with splenic injury, a mean age of 25 (± 8.9) years; 29.5% were 30 years or older, and 27.3% were younger than 20 years. The majority of patients were male. Pedestrian injuries were the most common 27.3%), and assault was reported in 10 (11.4%) cases. As shown in table 1.
Table 2 - Hemodynamic and shock parameters of the patients.
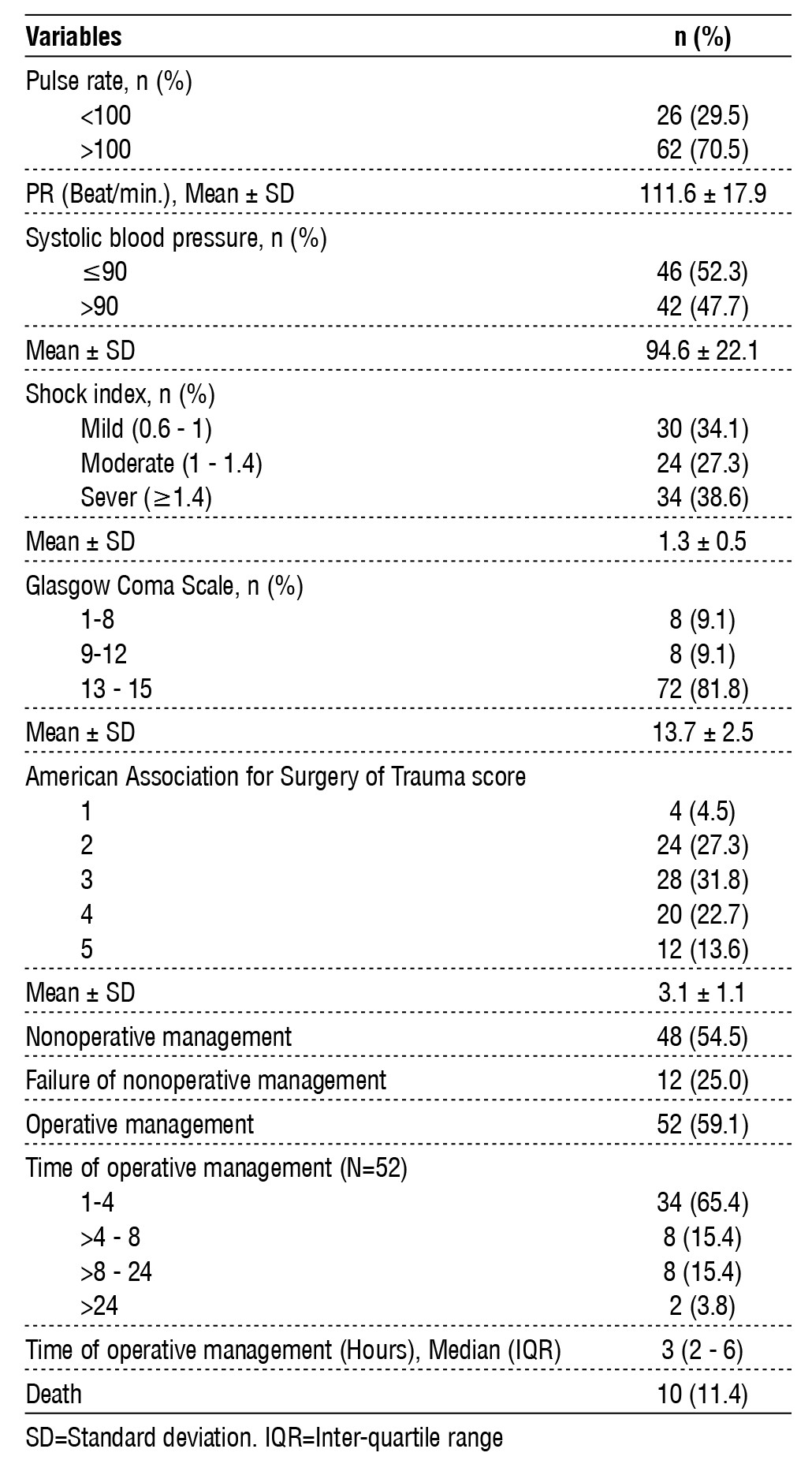
The hemodynamic condition of the patients was almost unstable, as tachycardia was found in 70.5% of patients and blood pressure was less than 90 mmHg in 46 (52.3%) of them. Moreover, only 34.1% had a mild shock, while mild and severe shock indices were found in 27.3% and 38.6% respectively. However, the GCS was higher than 12 in 72 (81.8%), and only 8 (9.1%) have less < 9 on the scale. More than two-thirds (68.2%) of the patients had 3+ an AAST score. Nonoperative was the primary management among 48 (54.4%) patients, but this method failed in 12 (25%) of them. Operative management was used for 52 (59.1%) patients in total (40 patients directly in addition to 12 patients who failed the conservative management method), and the operation time was within 4 h in 65.4% of them. In the end, 10 (11.4%) of the patients died (2 patients with NOM died due to severe head injury, while the other 8 patients who did OM died, 6 patients had multiple injuries including other abdominal organs like kidney, liver, mesentery, retroperitoneal hematoma, or pelvic fracture, all of whom had AAST score 5 and severe head injury, the other 2 patients had AAST score 4 and associated severe head injury (table 2).
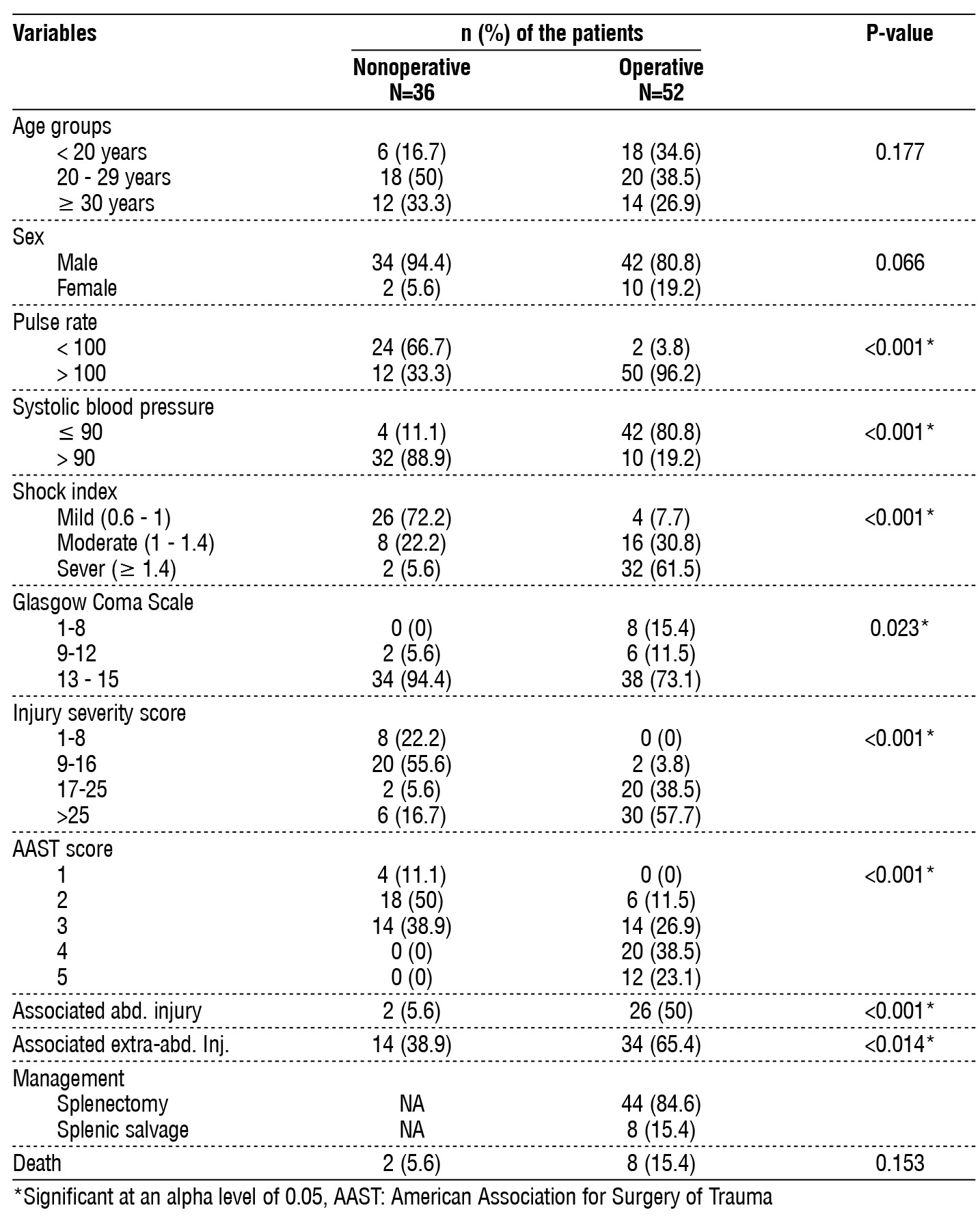
Patient age and sex were not associated with management type, whether operative or conservative. On the other hand, most patients who were managed operatively were hemodynamically unstable. Compared with the conservative group, patients who underwent surgery had shown prominent tachycardia (90.6% vs. 33.3%, p<0.001), and most of them were hypotensive (80.8% vs. 11.1%, p<0.001). shock index was mild in 72.2% of the patients managed conservatively compared to only 7.7% with operative management (p<0.001). None of the patients on nonoperative management had a GCS lower than 9, and only 2 (5.6%) had a scale of (9 -12) compared to 8 (15.4%) on a lower scale and 6 (11.5%) on a moderate scale among those operated for splenic injury, p=0.023). higher ISS (>16) was significantly associated with patients who underwent surgical intervention (96.2% vs. 22.3%, p<0.001). All 36 patients treated conservatively showed less than 3 on the AAST score, while 61.6% of the operated patients were associated with significantly higher scores, p<0.001). One-half of the 52 operated patients were found to have another associated abdominal organ injury, compared to only two (5.6%) of the patients on conservative treatment, p<0.001). The current study also showed a significant association of extra-abdominal injuries with the need for operative management 65.4% compared to 38.9% among those on conservative management, p=0.023. Splenectomy was performed in 44 (84.6%), while splenic salvage was possible in 8 (15.4%) of the patients who operated for splenic injury. Lastly, two patients (5.6%) in the patients on conservative management and 8 (15.4%) of the operated patients have died, with no significant association with the management type (table 3).
Table 3 - Comparison of the patients according to management of splenic injury.
Failure of conservative treatment was significantly associated with patients’ age, as 50% of those younger than 20 years needed an operative treatment compared to 25% of those aged between 20 and 29 years, while no one of aged 30 years or older failed to be treated conservatively, p=0.018). Females also had a significantly higher failure rate of conservative treatment compared to males in the current study (66.7% vs. 19%, p=0.012). Hemodynamically unstable patients were significantly associated with a higher rate of conservative management failure, as 45.5% of patients with tachycardia required surgical intervention compared to only 7.7% among patients with a pulse rate of 100 beats per minute or less, p=0.003). Two-thirds of the hypotensive patients failed the conservative treatment compared to 11.1% of normotensive patients (p<0.001). Moreover, conservative treatment failure was significantly associated with higher shock index p=0.017), ISS (p<0.001), and AAST p=0.001). On the other hand, the GCS score was not related to the failure of conservative treatment. The associated Abdominal injury was also associated with a high 66.7% failure rate of conservative treatment, p=0.012). In contrast, associated extra-abdominal injuries were not associated with conservative treatment failure. Of the 12 patients who failed the conservative management, 66.7% needed splenectomy, while splenic salvage was possible in the rest. Ultimately, only two patients of the patients who were managed conservatively died (table 4).
Table 4 - Comparison of the patients with splenic injury who managed nonoperative ly and those who failed and turned for operation.
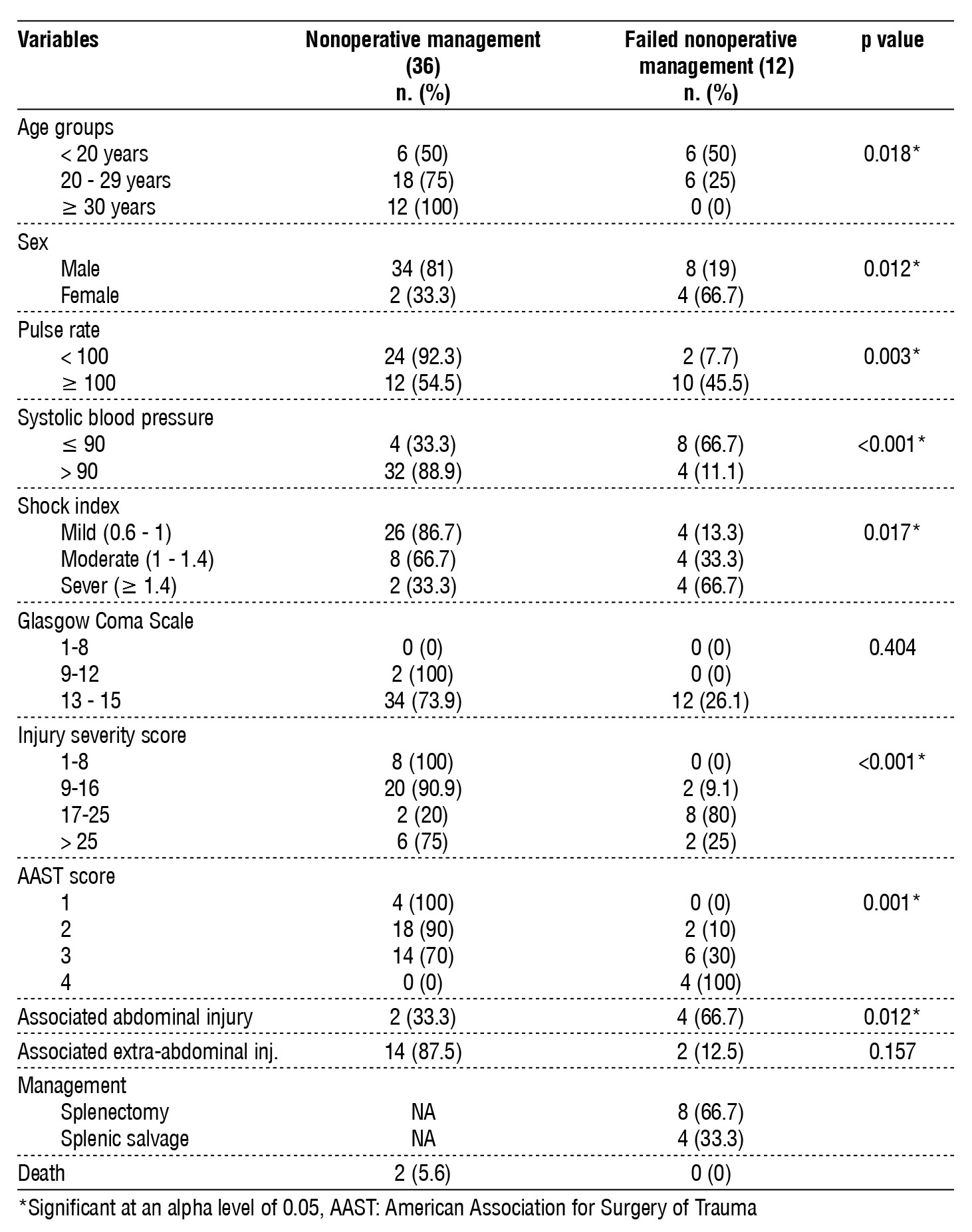
Table 5 - Associated abdominal and extra-abdominal injuries.
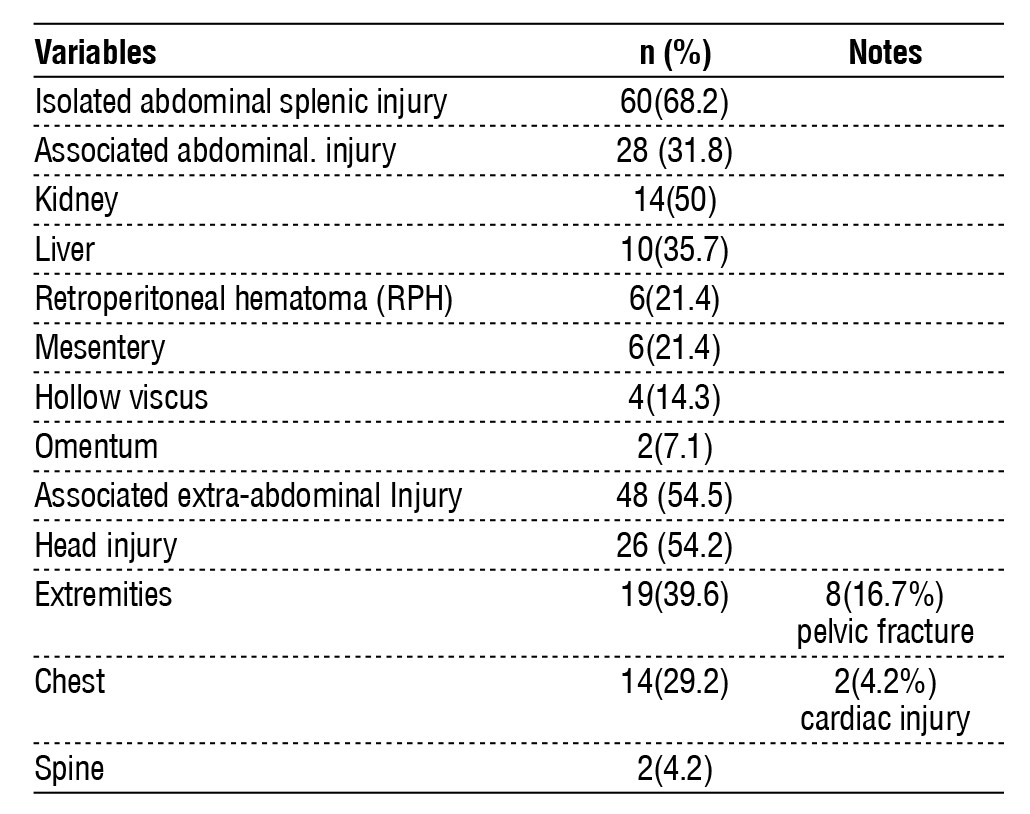
Isolated splenic injuries were reported in 68%, while associated abdominal injuries were reported in 31.8 %. The most common associated abdominal injury was the kidney in 50 %, followed by the liver in 35.7%, moreover, associated extra-abdominal injuries were found in 54.5% of patients, with head injuries most commonly reported extra-abdominal injury 54%. 2) followed by extremity injuries in 39.6%) (table 5). Fig. 1 showed a CT scan of abdomen of blunt splenic injury.
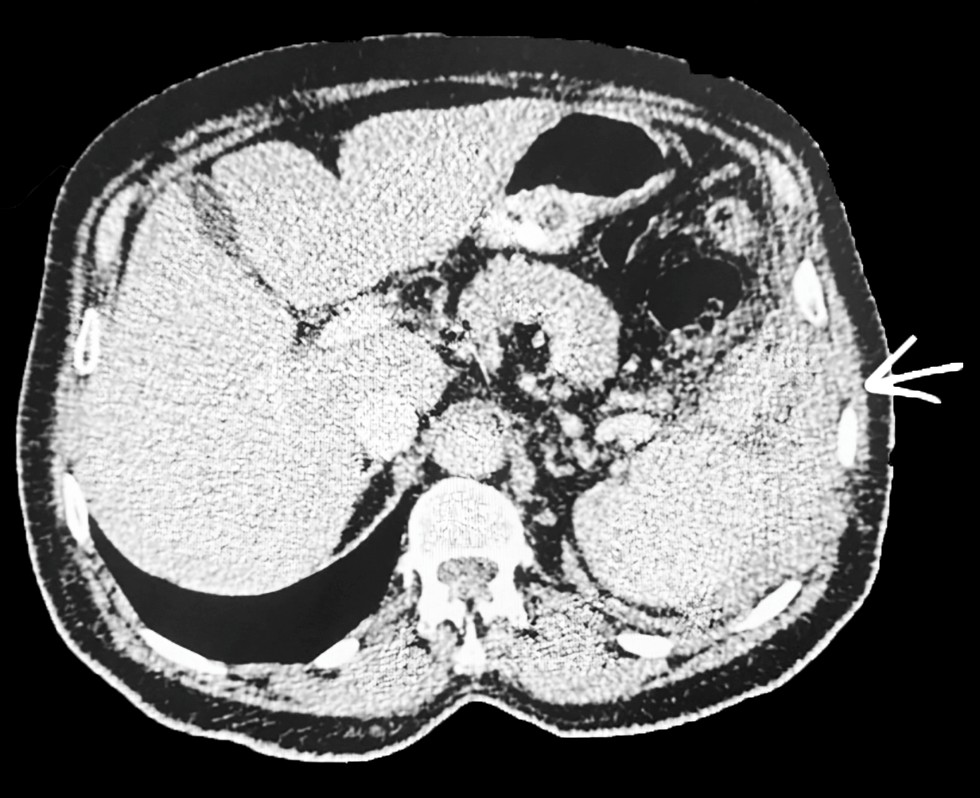
Figure 1 - 60-year-old male victim of MVA presented with left loin and hypochondrial pain, on examination: the patient is conscious, and oriented, BP 105/70, bruising on his left abdomen, abdomen soft, FAST shows free fluid in the pelvis, CT scan of abdomen deep laceration in the upper pole of the spleen, the patient treated conservatively successfully.
Discussion
Blunt abdominal trauma remains a major health problem, especially in developing countries, with splenic injury being the most common injured solid organ in the abdomen. Treatment changes in the last 100 years have been from splenectomy to splenic preservation of NOM when possible. The first successful splenectomy was performed by Reigner in 1893, and Bland-Sutton reported the first documented case of successful NOM (12,13). Most studies agree that the most important factors determining the feasibility of NOM are the patient's hemodynamic stability and other predictive factors that can affect the management (conservative versus surgical). With the increasing use of interventional radiology (angioembolization AE), OM substantially decreased, with a success rate of up to 93% for hemorrhage control and improved splenic salvage rates (14); however, we lack the facilities for AE in our center.
In our study, the age majority of patients were below 30 years (70.5%), with a mean age of presentation at 25 years, male patients were (86.4%). Pedestrian injury was the most common mechanism of injury (27.3%), followed by motor vehicle collision (MCV) (25%), and motorcycle collision (MCC) (20.5%). Haan et al. showed the mean age of patients was 32 years, and 76% were male; however, they showed the main mechanisms of injury were MVC (84%), followed by assaults (6%), falls from high (FFH) 4%), and 2% were pedestrian injuries (15). In line with our study, Farndon et al. showed the median age of the patients was 25 years, but they showed sports injury (46.3%) was the most common mechanism of injury, followed by MVC (33.8%) (16).
In our study, most of the patient's hemodynamically unstable, as tachycardia was found in 70.5% of patients, SBP was less than 90 mmHg in 46 (52.3%) patients, and severe shock indices were found in 38.6%. Patients. Lavanchy in A multicenter registry-based study including patients with splenic injuries entered into the Swiss Trauma Registry from 2015 to 2018 showed 23.9% of patients had SBP ≤ 100 mmHg and 38.5% had PR ≥ 100 bpm (17). We observed a high rate of hemodynamic instability in our patient sample.
Nonoperative was the primary management among 48 (54.4%) patients, but this method failed in 12 (25%) of them. Operative management was used for 52 (59.1%) patients (40 patients directly and 12 patients who failed the conservative management method). At the end, 10 (11.4%) of the patients died. The study of 6 years between 1988 and 1993 on Management Outcomes of Splenic Injury included 1255 patients, showing 40% of patients were treated NOM, with an Overall mortality of (12.7%) (18). Velmahos et al. in their study showed failed NOM in 33% of patients with blunt splenic injuries (19). While Peitzman, in a multi-institutional study that included 1488 patients with splenic injury shows 54.8% of patients were successfully managed with NOM, with a failure rate of 10.8%. The high failure rate of NOM in our patients is probably due to the lack of a radiological intervention facility at our center (20).
Our study showed that patient age and sex were not associated with initial management type, whether operative or conservative. On the other hand, most patients who were managed operatively were hemo-dynamically unstable. Compared with the conservative group, patients who underwent surgery had shown prominent tachycardia (90.6% vs. 33.3%, p<0.001), and most of them were hypo-tensive (80.8% vs. 11.1%, p<0.001). Shock index was mild in 72.2% of the patients managed conservatively compared to only 7.7% with operative management (p<0.001). None of the patients on nonoperative management had a GCS lower than 9, and only 2 (5.6%) had a scale of (9-12) compared to 8 (15.4%) on a lower scale and 6 (11.5%) on a moderate scale among those operated for splenic injury, p=0.023).
Most studies show a significant association between hemodynamic instability and initial OM (10,20-22). In a retrospective study that included 126 patients with solid organ abdominal injuries, including those of the spleen, the authors showed that the main indication for immediate OM is hemodynamic instability. Neither the presence of head injury nor age contraindicated NOM (23). In line with our study, Lavanchy et al. showed that SBP ≤ 100 mmHg was an independent factor for successful NOM. However, they showed that GCS ≤ 8 was a risk factor for NOM (17).
Higher ISS (>16) was significantly associated with patients who underwent surgical intervention (96.2% vs. 22.3%, p<0.001). All 36 patients treated conservatively showed less than 3 on the AAST score, while 61.6% of the operated patients were associated with significantly higher scores, p<0.001. Similarly, most studies have shown that high ISS and higher AAST scores are associated with a high rate of initial OM (19,24-27). Peitzman et al. showed successful NOM correlated with the grade of splenic injury (75 % in grade I, 70 % in grade II, 49.3 % in grade III, 16.9 % in grade IV, and 1.3 % in grade V) (20). Olthof et al. reported a systematic review from 1995 to 2011, which included 25 prognostic factors showing a significant relationship between ISS of 25 or higher and splenic injury grade of 3 or greater as predictive factors for failure of NOM (27).
We showed a significant association between surgical OM and intra-abdominal injuries, where 50% of operated patients were found to have another associated abdominal injury, compared to only two (5.6%) of the patients receiving conservative treatment, in addition to extra-abdominal injuries related to the need for operative management 65.4% compared to 38.9% among those on conservative management).
Velmahos et al. showed that an abdominal Abbreviated Injury Scale (AIS) score of 3 or more was associated with a high rate of OM (19), and Jeremitsky et al. demonstrated that a mean (AIS score of 3.9 was related to a high rate of OM (28). Frandon et al. reported in their study that 68.4% had at least one other organ injury, including 57.4% with an associated thoracic injury with a high rate of OM in Hollow viscus injury followed by limb fracture and left thoracic injury (lung, ribs) (16).
The current study showed that failure of conservative treatment was significantly associated with patients’ age, as 50% of those younger than 20 years needed an operative treatment compared to 25% of those aged between 20 and 29 years, while no patient the aged of 30 years or older failed to be treated conservatively, P=0.018). Females also had a significantly higher failure rate of conservative treatment than males in the current study (66.7% vs. 19%, p=0.012). In contrast, many other studies have shown a high NOM failure rate related to older age (19,24,29). The difference is probably because our patients' sample was mostly young, with only 26 (29.5%) patients older than 30 years, in addition, the younger age group may sustain high energy level trauma due to an active lifestyle.
In our study, hemodynamically unstable patients were significantly associated with a higher rate of
conservative management failure, as 45.5% of patients with tachycardia required surgical intervention compared to only 7.7% among patients with a pulse rate of 100 beats per minute or less, p=0.003). Two-thirds of the hypotensive patients failed the conservative treatment compared to 11.1% of normotensive patients, p<0.001). In addition, conservative treatment failure was significantly associated with higher shock index p=0.017) and injury severity (p<0.001). Similarly, many studies have demonstrated a correlation between hemo-dynamic instability and FNOM (27,28,30).
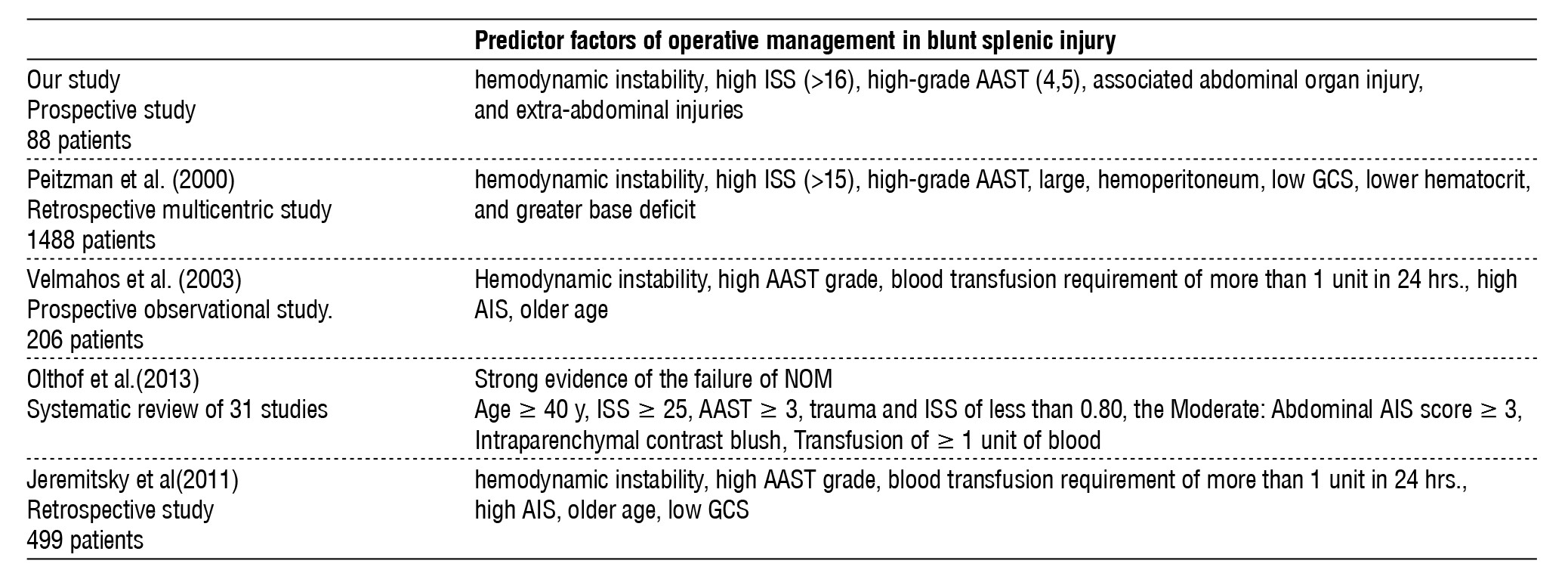
ISS and AAST levels were significantly associated with FOM. On the other hand, the GCS score was not related to the failure of conservative treatment. An ISS of 25 or higher is significantly associated with FNOM and has been supported in many studies (27,28,31). Moreover, GCS scores did not demonstrate a significant relationship with FNOM in many studies (24,27,32). However, Jeremitsky et al. showed a relationship between FNOM and GCS, where patients with FNOM had lower GCS scores than patients with successful NOM (28). Peitzman et al. showed FNOM progressively increased with the grade of splenic injury: 4.8% (I), 9.5% (grade II), 19.6% (III), 33.3% (IV), and 75.0% (grade V). Laparotomy was ultimately performed in 25.0% (grade I), 30.0% (grade II), 50.7% (grade III), 83.1% (IV), and 98.7% (V). Grade I and grade II splenic injuries are associated with a high likelihood of successful NOM (20). In addition, many studies support a high failure rate of NOM with high-grade splenic injury (grades 4 and 5) and a high rate of early laparotomy (21,33,34) (table 6).
Table 6 - Compares the predictor factors of operative management in blunt splenic injury with other studies.
Conclusion
Most patients were below 30 years, with a mean age of presentation of 25 years. Pedestrian injury was the most common mechanism of injury. In most of the patients, the hemodynamically unstable presentation times. Non-operative management was the primary treatment among 54.4% of patients, but this method failed in 25% of them. Operative management was used for 59.1% of patients (40 patients directly operated on + 12 patients who failed the conservative management method). At the end, 11.4% of the patients died. Our study shows a significant relationship between initial OM and hemodynamic instability, high ISS (>16), high-grade AAST (4,5), associated abdominal organ injury, and extra-abdominal injuries; however, the patients’ age and sex were and GCS not associated with their initial management type, whether operative or conservative. In our study, we show factors related to FNOM that include the young age group, female gender, hemodynamic instability, high-grade ASST, and associated abdominal injury; neither GCS nor extra-abdominal injury is related to the failure of NOM.
Conflict of Interest
Author declare no any conflict.
References
1. Wiik Larsen J, Søreide K, Søreide JA, Tjosevik K, Kvaløy JT, Thorsen K. Epidemiology of abdominal trauma: An age- and sex-adjusted incidence analysis with mortality patterns. Injury. 2022;53(10): 3130-3138.
2. Novack JC, Whitton EL, Smith RN, Sciarretta JD, Nguyen J. Abdominal Wall Evisceration Coupled With Iliac Vascular Injury After Blunt Trauma. Cureus. 2023;15(2):e34917.
3. Feliciano DV. Abdominal Trauma Revisited. Am Surg. 2017;83(11): 1193-1202.
4. Schroeppel TJ, Croce MA. Diagnosis and management of blunt abdominal solid organ injury. Curr Opin Crit Care. 2007;13(4): 399-404.
5. Raza M, Abbas Y, Devi V, Prasad KV, Rizk KN, Nair PP. Nonoperative management of abdominal trauma - a 10 years review. World J Emerg Surg. 2013;8:14.
6. Zeng S, Wang W, Chen W, Xiao J. Clinical comparative study of laparoscopic partial splenectomy and open partial splenectomy. Wideochir Inne Tech Maloinwazyjne. 2024;19(2):211-222.
7. Ransom KJ, Kavic MS. Laparoscopic splenectomy following embolization for blunt trauma. JSLS. 2008;12(2):202-5.
8. Leppäniemi A. Nonoperative management of solid abdominal organ injuries: From past to present. Scand J Surg. 2019;108(2):95-100.
9. Brillantino A, Iacobellis F, Festa P, Mottola A, Acampora C, Corvino F, et al. Nonoperative Management of Blunt Liver Trauma: Safety, Efficacy and Complications of a Standardized Treatment Protocol. Bull Emerg Trauma. 2019;7(1):49-54.
10. Fodor M, Primavesi F, Morell-Hofert D, Haselbacher M, Braunwarth E, Cardini B, et al. Nonoperative management of blunt hepatic and splenic injuries-practical aspects and value of radiological scoring systems. Eur Surg. 2018;50(6):285-298.
11. Yiannoullou P, Hall C, Newton K, Pearce L, Bouamra O, Jenks T, et al. A review of the management of blunt splenic trauma in England and Wales: have regional trauma networks influenced management strategies and outcomes? Ann R Coll Surg Engl. 2017;99(1):63-69.
12. Gauer JM, Gerber-Paulet S, Seiler C, Schweizer WP. Twenty years of splenic preservation in trauma: lower early infection rate than in splenectomy. World J Surg. 2008;32(12):2730-5.
13. Demetriades D, Hadjizacharia P, Constantinou C, Brown C, Inaba K, Rhee P, Salim A. Selective nonoperative management of penetrating abdominal solid organ injuries. Ann Surg. 2006;244(4):620-8.
14. Watson GA, Hoffman MK, Peitzman AB. Nonoperative management of blunt splenic injury: what is new? Eur J Trauma Emerg Surg. 2015;41(3):219-28.
15. Haan JM, Bochicchio GV, Kramer N, Scalea TM. Nonoperative management of blunt splenic injury: a 5-year experience. J Trauma. 2005;58(3):492-8.
16. Frandon J, Rodiere M, Arvieux C, Vendrell A, Boussat B, Sengel C, et al. Blunt splenic injury: are early adverse events related to trauma, nonoperative management, or surgery? Diagn Interv Radiol. 2015; 21(4):327-33.
17. Lavanchy JL, Delafontaine L, Haltmeier T, Bednarski P, Schnüriger B; Swiss Trauma Registry. Increased hospital treatment volume of splenic injury predicts higher rates of successful nonoperative
management and reduces hospital length of stay: a Swiss Trauma Registry analysis. Eur J Trauma Emerg Surg. 2022; 48(1):133-140.
18. Ko A, Radding S, Feliciano DV, DuBose JJ, Kozar RA, Morrison J, et al. Near Disappearance of Splenorrhaphy as an Operative Strategy for Splenic Preservation After Trauma. Am Surg. 2022;88(3):429-433.
19. Velmahos GC, Toutouzas KG, Radin R, Chan L, Demetriades D. Nonoperative treatment of blunt injury to solid abdominal organs: a prospective study. Arch Surg. 2003;138(8):844-51.
20. Peitzman AB, Heil B, Rivera L, Federle MB, Harbrecht BG, Clancy KD, et al. Blunt splenic injury in adults: Multi-institutional Study of the Eastern Association for the Surgery of Trauma. J Trauma. 2000; 49(2):177-87.
21. Alabbasi T, Nathens AB, Tien H. Blunt splenic injury and severe brain injury: a decision analysis and implications for care. Can J Surg. 2015;58(3 Suppl 3):S108-17.
22. Leone RJ Jr, Hammond JS. Nonoperative management of pediatric blunt hepatic trauma. Am Surg. 2001;67(2):138-42.
23. Sartorelli KH, Frumiento C, Rogers FB, Osler TM. Nonoperative management of hepatic, splenic, and renal injuries in adults with multiple injuries. J Trauma. 2000;49(1):56-61; discussion 61-2.
24. Renzulli P, Gross T, Schnüriger B, Schoepfer AM, Inderbitzin D, Exadaktylos AK, et al. Management of blunt injuries to the spleen. Br J Surg. 2010;97(11):1696-703.
25. McIntyre LK, Schiff M, Jurkovich GJ. Failure of nonoperative management of splenic injuries: causes and consequences. Arch Surg. 2005;140(6):563-8.
26. Gonzalez M, Bucher P, Ris F, Andereggen E, Morel P. Traumatisme de la rate: facteurs prédictifs d'échec du traitement non-opératoire (Splenic trauma: predictive factors for failure of nonoperative management). J Chir (Paris). 2008;145(6):561-7.
27. Olthof DC, Joosse P, van der Vlies CH, de Haan RJ, Goslings JC. Prognostic factors for failure of nonoperative management in adults with blunt splenic injury: a systematic review. J Trauma Acute Care Surg. 2013;74(2):546-57.
28. Jeremitsky E, Kao A, Carlton C, Rodriguez A, Ong A. Does splenic embolization and grade of splenic injury impact nonoperative management in patients sustaining blunt splenic trauma? Am Surg. 2011;77(2):215-20.
29. Duchesne JC, Simmons JD, Schmieg RE Jr, McSwain NE Jr, Bellows CF. Proximal splenic angioembolization does not improve outcomes in treating blunt splenic injuries compared with splenectomy: a cohort analysis. J Trauma. 2008;65(6):1346-51.
30. Koide Y, Okada T, Yamaguchi M, Sugimoto K, Murakami T. The Management of Splenic Injuries. Interv Radiol (Higashimatsuyama). 2023;9(3):149-155.
31. Myers JG, Dent DL, Stewart RM, Gray GA, Smith DS, Rhodes JE, et al. Blunt splenic injuries: dedicated trauma surgeons can achieve a high rate of nonoperative success in patients of all ages. J Trauma. 2000;48(5):801-5.
32. Velmahos GC, Zacharias N, Emhoff TA, Feeney JM, Hurst JM, Crookes BA, et al. Management of the most severely injured spleen: a multicenter study of the Research Consortium of New England Centers for Trauma (ReCONECT). Arch Surg. 2010;145(5):456-60.
33. Berg RJ, Inaba K, Okoye O, Pasley J, Teixeira PG, Esparza M, et al. The contemporary management of penetrating splenic injury. Injury. 2014;45(9):1394-400.
34. Tsugawa K, Koyanagi N, Hashizume M, Ayukawa K, Wada H, Tomikawai M, et al. New insight for management of blunt splenic trauma: significant differences between young and elderly. Hepato-gastroenterology. 2002;49(46):1144-9.
Full Text Sources:
Abstract:
Views: 7548

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.