Surgery, Gastroenterology and Oncology

|
|
Introduction: Intraductal papillary neoplasm of the bile duct (IPNB) is associated with better prognosis than biliary cancer after curative surgery.
Case report: We report a case of a 59-year-old woman who presented with an enlarging liver cyst with a mural nodule. Laboratory data indicated normal hepatobiliary function and tumor markers. Imaging revealed a lesion at liver segments 5 and 6, with dynamic computed tomography revealing slight enhancement of the nodule during the early phase, prolonged during the delayed phase.
Results: Magnetic resonance cholangiopancreatography revealed that the tumor was connected to segment 5 of the bile duct. Endoscopic retrograde cholangiopancreatography confirmed dilation of the bilateral intrahepatic bile duct owing to mucin obstruction from the tumor. Biopsy results were negative for malignancy, leading to a diagnosis of IPNB. Consequently, laparoscopic posterior segmentectomy and segment 5 resection were performed (operative duration: 433 min; intraoperative blood loss: 25 mL). Postoperative recovery was uneventful, and pathological examination indicated intestinal-type glandular epithelium with no invasive characteristics. The pathological diagnosis was IPNB without an invasive pattern. The surgical margin was clear, and no recurrence was observed 1 year postoperatively.
Conclusion: Although IPNB is rare and challenging to diagnose preoperatively, evaluation of horizontal tumor spread and laparoscopic hepatectomy are effective for noninvasive cases.
Introduction
Intraductal papillary neoplasm of the bile duct (IPNB) was not clearly classified until 2010 when the World Health Organization proposed an integrated classification that recognized IPNB as a distinct entity. IPNB accounts for 10-15% of all bile duct tumors (1). It is considered the counterpart of intraductal papillary mucinous neoplasm (IPMN) of the pancreas (P-IPMN). Treatment strategies for IPNB vary among different geographical locations. Although IPNB with an invasive pattern has a poor prognosis, aggressive surgical resection for IPNB is associated with a 5-year overall survival rate of approximately 50% (2,3).
Similar to IPMN, IPNB can be classified into intestinal, gastric, biliopancreatic, and acidophilic subtypes (4). It can also be categorized by location as intrahepatic, extrahepatic, and diffuse (4-6). Recently, biliary patho-logists in Japan and Korea have proposed subclassifying IPNB into types I and II based on growth morphology and atypia. The World Health Organization has adopted this subclassification in its 2019 revision (5th edition) and described its characteristics (4).
In this report, we present the case of a patient with a preoperative diagnosis of IPNB who underwent laparoscopic hepatectomy. We also present a review of the literature on IPNB.
Case Report
A 59-year-old woman presented to our hospital with an enlarging liver cyst comprising a mural nodule. The cyst was observed during a routine examination and followed up annually. The size of the cyst had increased over 2 years, and the mural nodule appeared within the cyst. Her medical history included hypothyroidism, acute appendicitis, and uterine fibroids. Laboratory test results indicated normal hepatobiliary enzymes and tumor markers, Child-Pugh grade A, liver damage grade A, and an indocyanine green retention rate at 15 min of 6.5%. Her family history was unremarkable.
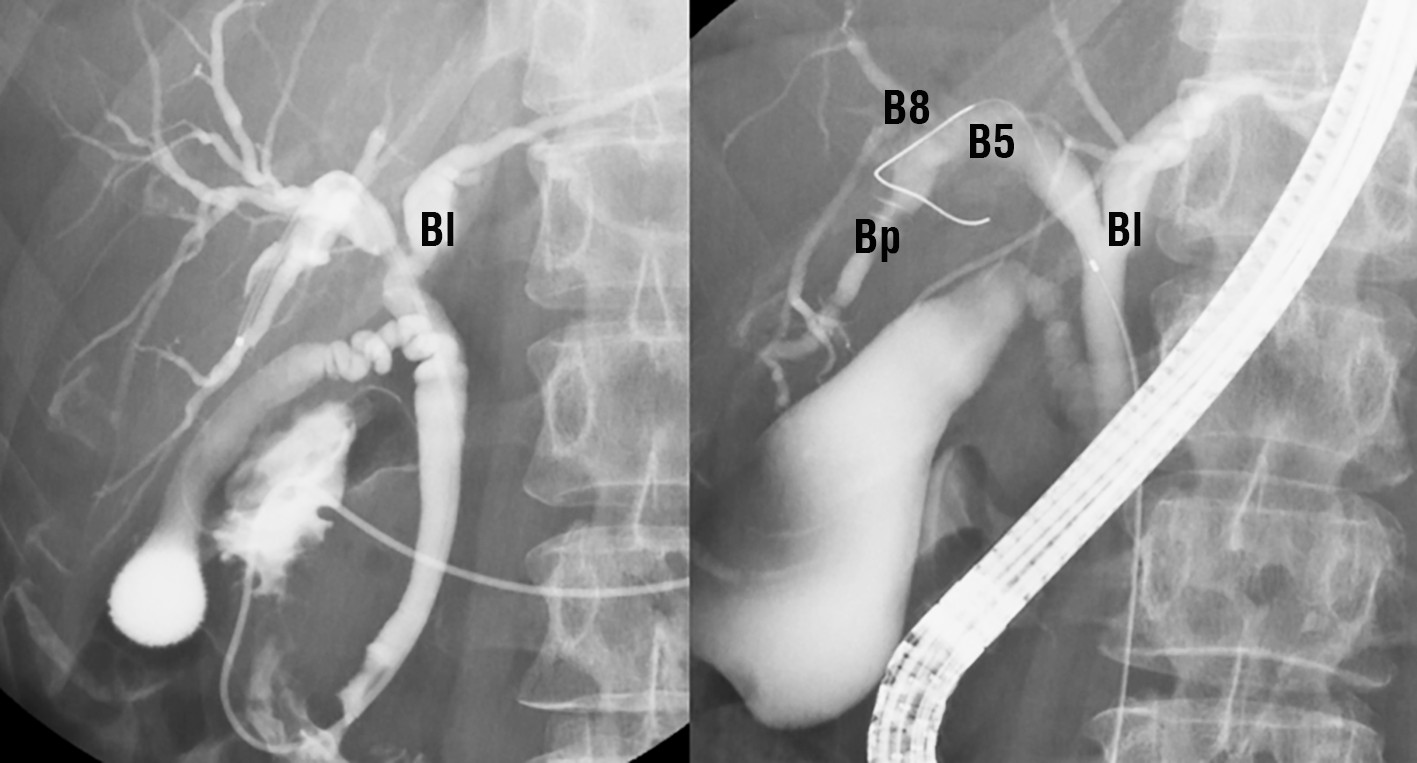
Abdominal ultrasonography identified a space-occupying lesion at liver segments 5 and 6, measuring 30 × 30 mm in diameter, with a mural nodule. Dynamic computed tomography indicated that the mural nodule inside the cyst was slightly enhanced during the early phase; this enhancement was prolonged during the delayed phase (fig. 1 a-c). Magnetic resonance cholangiopancreatography revealed that the tumor was connected to the biliary duct of segment 5 (fig. 2 a, b). Endoscopic retrograde cholangiopancreatography revealed that the intrahepatic bile duct was dilated owing to mucin produced by the tumor and that the tumor was connected to segment 5 of the biliary duct
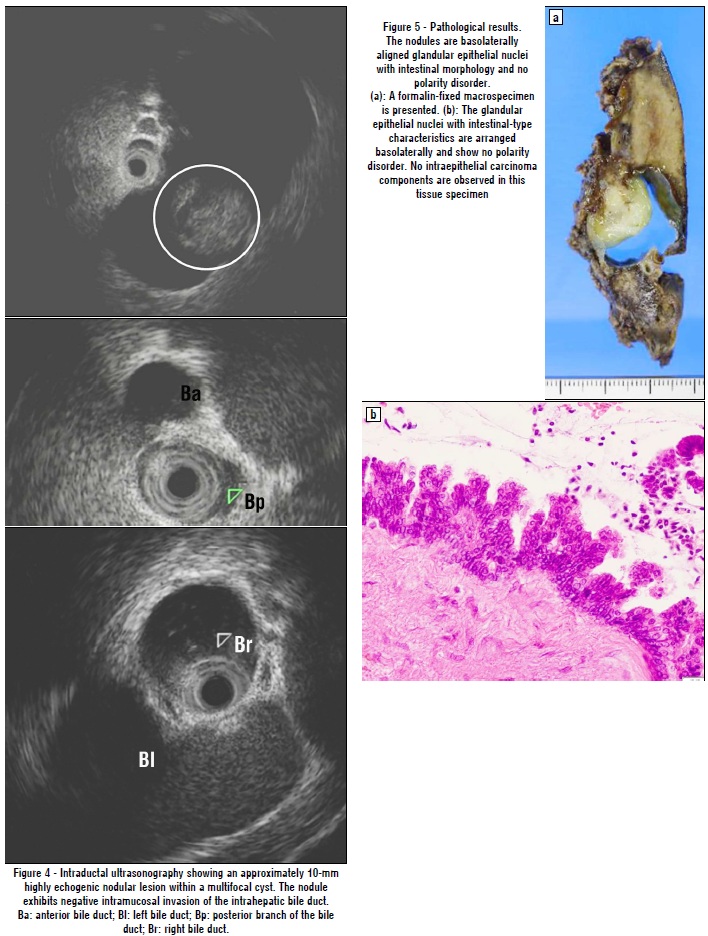
(fig. 3). A step biopsy of the liver hilum, branches of the anterior and posterior bile ducts, and right main bile duct demonstrated no malignancy. Intraductal ultrasonography revealed an approximately 10-mm highly echogenic nodular lesion within a multifocal cyst. The nodule exhibited no intramucosal invasion of the intrahepatic bile duct (fig. 4). Therefore, IPBN was diagnosed.
Figure 1 - Abdominal computed tomography findings. (a) and (b): A multilobular 30- × 30-mm tumor with adjacent lesions detected in liver segments 5 and 6. The arrows (®) indicate where the mural nodule inside the cyst is slightly enhanced during the early phase. This enhancement was prolonged during the delayed phase. (c): This image reveals dilatation of the right hepatic duct
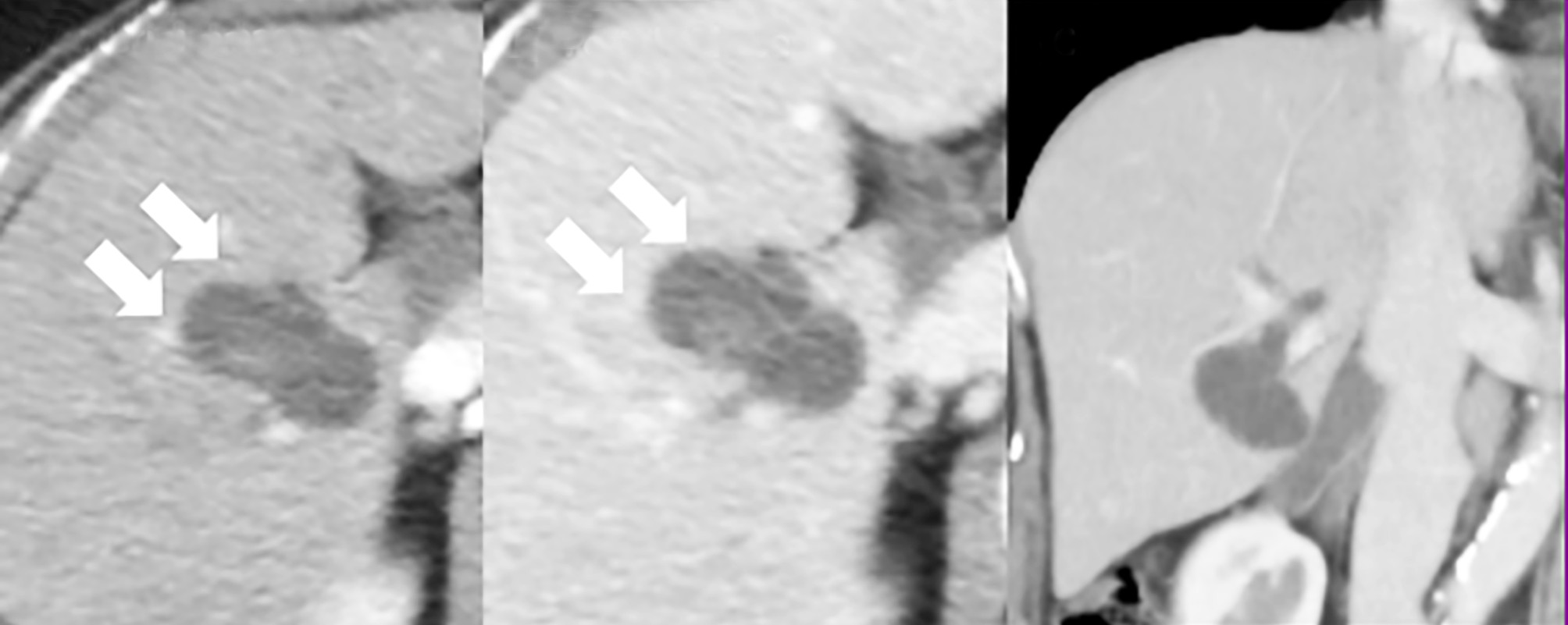
Figure 2 - Magnetic resonance cholangiopancreatography (MRCP). (a): MRCP shows a 30-mm multifocal cyst at segment 5 with a liquid reservoir inside. (b): Diffusion-weighted image (DWI) reveals a pale abnormal signal from the mural nodule within the cyst
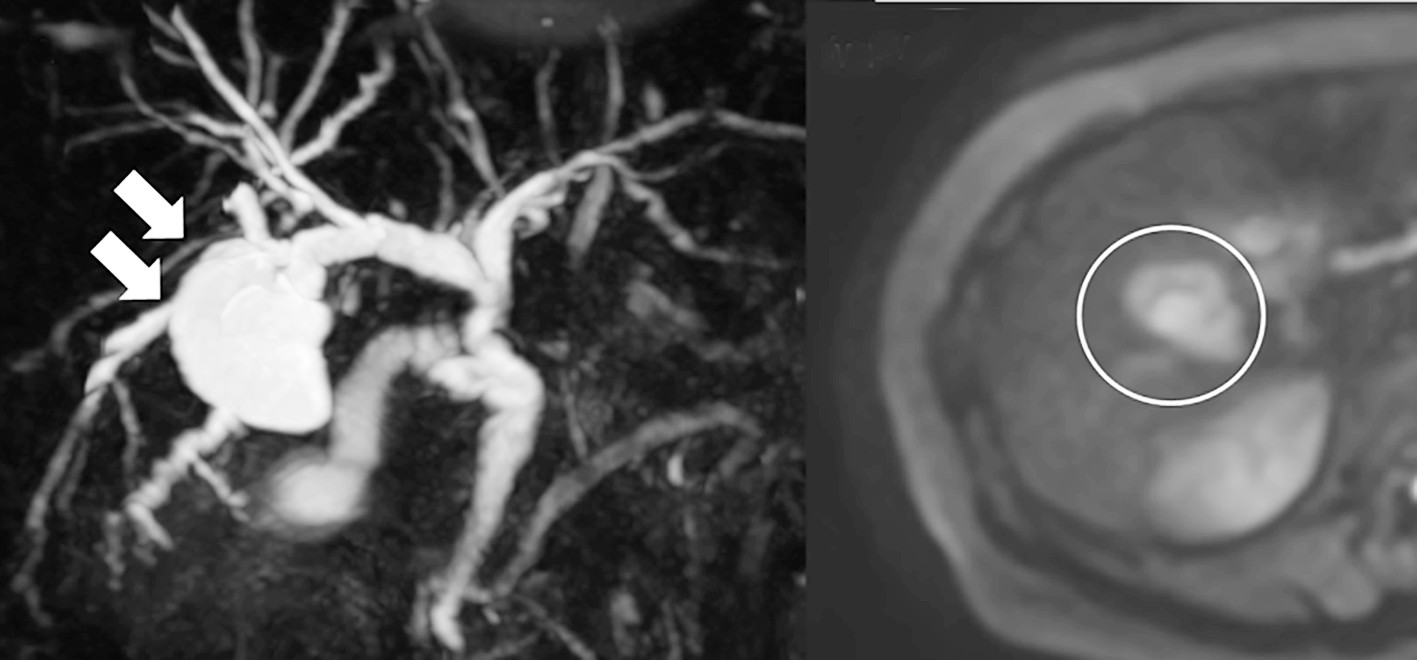
Figure 3 - Endoscopic retrograde cholangiopancreatography. (a) and (b): a cystic mass traversing the biliary duct of segment 5 (B5). No bile duct anomalies are observed. The results of step biopsy and bile cytology tests are negative for the left bile duct (Bl), B8, and posterior branch of the bile duct (Bp)
Accordingly, Laparoscopic posterior segmentectomy and anatomical resection of segment 5 were performed. The operative duration was 433 min, and the intraoperative blood loss was 25 mL. Pathological examination indicated that the tumor was lined with glandular epithelium with intestinal-type characteristics and that the nuclei were arranged baso-laterally while maintaining polarity (fig. 5). Intra-epithelial carcinoma components were not observed. An immunohistochemical analysis revealed no estrogen receptors or progesterone receptors in the tumor. The pathological diagnosis was IPNB without an invasive pattern. The surgical margin was free from tumor invasion. The postoperative course was uneventful, and the patient was discharged 8 days postoperatively.
Discussion
Symptoms of IPNB, including abdominal pain and jaundice, vary among patients. Therefore, a precise preoperative diagnosis, which is important for ensuring optimal surgical treatment, can be difficult. The prognosis of IPNB is better than that of biliary cancer; however, progression to adenocarcinoma is associated with a poorer prognosis (7). Risk factors for recurrence in patients with IPNB include R1/R2 resection, lymph node metastasis, and invasive patterns (8). Additionally, the presence of invasive components in the surgical margin can affect recurrence (9). The presence of minimal dysplasia in the surgical margin is reportedly associated with a poor prognosis (7). In our case, the tumor did not invade the anterior branch of the biliary duct, as confirmed via a preoperative biliary biopsy. Instead, the tumor occupied the posterior segment, necessitating posterior segmentectomy and segment 5 resection for tumor-free margins. The surgical margin was pathologically free from tumor invasion. Other factors that predict the prognosis include MUC2 positivity, type I disease, and intestinal patterns (8), and our case was categorized as type I IPNB based on the immunohistochemical staining pattern.
Lymph node dissection is important for achieving a good long-term prognosis for intrahepatic cholangiocarcinoma (ICC) (10). Various studies have reported that lymph node metastasis negatively affects the recurrence-free survival of patients with ICC. However, Luvira et al. (10) concluded that routine lymph node dissection is not necessary for IPNB, as metachronous lesions in the remaining liver can affect survival, even in patients with nonmalignant IPNB. They also noted that IPNB has a low propensity for lymph node metastasis. Our patient did not undergo lymph node dissection because the preoperative diagnosis was IPNB without an invasive pattern. Considering the favorable prognosis of IPNB, routine lymph node dissection is unlikely to influence long-term outcomes. However, as discriminating between nonmalignant IPNB and IPNB with invasive patterns is difficult, further prospective studies are required to evaluate the effect of routine lymph node dissection on long-term prognosis.
IPNB is usually associated with a higher pancreaticobiliary type than IPMN. Aoki et al. (11) reported the presence of high-grade dysplasia and invasive types in IPNB, whereas low-grade and intermediate-grade dysplasia were not observed. In the present case, the patient had intrahepatic type I IPNB and mucin hypersecretion. The prognosis of type I IPNB is similar to that of IPMN, and type II IPNB has a poorer prognosis than type I IPNB. Moreover, the expression of MUC5AC and MUC6 significantly affects the long-term prognosis of IPNB (11). Although the prognostic values of these mucins vary among studies, there is limited literature on the prognostic significance of MUC6 expression. Moreover, previous studies have shown inconsistent results regarding the clinical impact of MUC5AC expression on the surgical outcomes of ICC and pancreatic neoplasms, including P-IPMN. MUC5AC expression is strongly associated with a high American Joint Committee on Cancer tumor category, lymph node metastasis, and worse postoperative survival with ICC, as well as with decreased lymph node metastasis, decreased incidence of vascular invasion, and better postoperative survival with pancreatic neoplasms, including that of P-IPMN (12).
Recent advances in laparoscopic liver resection have led to improved postoperative outcomes, including fewer postoperative complications and shorter hospital stays, without increasing the blood loss volume and mortality (13). Malignancies, particularly colorectal liver metastasis (CRLM) and hepatocellular carcinoma (HCC), are the most common indications for laparoscopic major hepatectomy (LMH) (14). Considering oncological efficacy, LMH is associated with long-term survival rates comparable to those of open hepatectomy in CRLM and HCC cases (15-19). Matono et al. (20) reported the first case of branch-type IPNB after laparoscopic anatomical resection, although previous reports have described open hepatectomy for such cases. Laparoscopic hepatectomy results in a shorter post-operative hospital stay and lower intraoperative blood loss than open hepatectomy (21).
Patients with branch-type IPNB without an invasive pattern are good candidates for laparoscopic hepatectomy, and a precise horizontal tumor spread of the bile duct is important for achieving R0 resection. Accurate diagnosis of IPNB and thorough evaluation of tumor spread are crucial; laparoscopic hepatectomy may be the optimal option for noninvasive cases.
Author’s Contributions
MT and TA conceived the presented idea, developed the theory, and performed the computations. MI, MK, RH, KT, and TT provided encouragement to investigate specific aspects of the case and supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Conflict of Interest
The authors declare that they have no competing interests.
Ethical Statement
All procedures performed during this research were approved by the Ethical Committee of our institution.
Informed Consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Availability of Data and Materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
1. Ainechi S, Lee H. Updates on precancerous lesions of the biliary tract: biliary precancerous lesion. Arch Pathol Lab Med. 2016;140(11):1285-1289.
2. Abe T, Amano H, Shimamoto F, Hattori M, Kuroda S, Kobayashi T, al. Prognostic evaluation of mucin-5AC expression in intrahepatic cholangiocarcinoma, mass-forming type, following hepatectomy. Eur J Surg Oncol. 2015;41(11):1515-21.
3. Lluís N, Serradilla-Martín M, Achalandabaso M, Jehaes F, Dasari BVM, Mambrilla-Herrero S, et al. Intraductal papillary neoplasms of the bile duct: a European retrospective multicenter observational study (EUR-IPNB study). Int J Surg. 2023;109(4):760-771.
4. Nakanuma Y, Kakuda Y, Uesaka K. Characterization of intraductal papillary neoplasm of the bile duct with respect to the histopathologic similarities to pancreatic intraductal papillary mucinous
neoplasm. Gut Liver. 2019;13(6):617-627.
5. Fujita M, Wakui N, Yamauchi Y, Takeda Y, Sato T, Ueki N, et al. A case of branch duct type intraductal papillary neoplasm of the bile duct treated by open surgery after 11 years of follow-up. Mol Clin Oncol. 2013;1(6):965-969.
6. Kim JR, Jang KT, Jang JY, Lee K, Kim JH, Kim H, et al. Clinicopathologic analysis of intraductal papillary neoplasm of bile duct: Korean multicenter cohort study. HPB (Oxford). 2020; 22(8):1139-1148.
7. Jung G, Park KM, Lee SS, Yu E, Hong SM, Kim J. Long-term clinical outcome of the surgically resected intraductal papillary neoplasm of the bile duct. J Hepatol. 2012;57(4):787-93.
8. Bennett S, Marginean EC, Paquin-Gobeil M, Wasserman J, Weaver J, Mimeault R, et al. Clinical and pathological features of intraductal papillary neoplasm of the biliary tract and gallbladder. HPB (Oxford). 2015;17(9):811-8.
9. Igami T, Nagino M, Oda K, Nishio H, Ebata T, Yokoyama Y, et al. Clinicopathologic study of cholangiocarcinoma with superficial spread. Ann Surg. 2009;249(2):296-302.
10. Luvira V, Pugkhem A, Bhudhisawasdi V, Pairojkul C, Sathitkarnmanee E, Luvira V, et al. Long-term outcome of surgical resection for intraductal papillary neoplasm of the bile duct. J Gastroenterol Hepatol. 2017;32(2):527-533.
11. Aoki Y, Mizuma M, Hata T, Aoki T, Omori Y, Ono Y, et al. Intraductal papillary neoplasms of the bile duct consist of two distinct types specifically associated with clinicopathological features and
molecular phenotypes. J Pathol. 2020;251(1):38-48.
12. Harada F, Matsuyama R, Mori R, Kumamoto T, Morioka D, Taguri M, et al. Outcomes of surgery for 2010 WHO classification-based intraductal papillary neoplasm of the bile duct: case-control study of a single Japanese institution's experience with special attention to mucin expression patterns. Eur J Surg Oncol. 2019;45(5):761-768.
13. Kasai M, Cipriani F, Gayet B, Aldrighetti L, Ratti F, Sarmiento JM, et al. Laparoscopic versus open major hepatectomy: a systematic review and meta-analysis of individual patient data. Surgery. 2018; 163(5):985-995.
14. Dagher I, Gayet B, Tzanis D, Tranchart H, Fuks D, Soubrane O, et al. International experience for laparoscopic major liver resection. J Hepatobiliary Pancreat Sci. 2014;21(10):732-6.
15. Abu Hilal M, Di Fabio F, Syed S, Wiltshire R, Dimovska E, Turner D, et al. Assessment of the financial implications for laparoscopic liver surgery: a single-centre UK cost analysis for minor and major hepatectomy. Surg Endosc. 2013;27(7):2542-50.
16. Komatsu S, Brustia R, Goumard C, Perdigao F, Soubrane O, Scatton O. Laparoscopic versus open major hepatectomy for hepatocellular carcinoma: a matched pair analysis. Surg Endosc. 2016; 30(5):1965-74.
17. Medbery RL, Chadid TS, Sweeney JF, Knechtle SJ, Kooby DA, Maithel SK, et al. Laparoscopic vs open right hepatectomy: a value-based analysis. J Am Coll Surg. 2014;218(5):929-39.
18. Topal H, Tiek J, Aerts R, Topal B. Outcome of laparoscopic major liver resection for colorectal metastases. Surg Endosc. 2012; 26(9):2451-5.
19. Yoon YI, Kim KH, Kang SH, Kim WJ, Shin MH, Lee SK, et al. Pure laparoscopic versus open right hepatectomy for hepatocellular carcinoma in patients with cirrhosis: a propensity score matched analysis. Ann Surg. 2017;265(5):856-863.
20. Matono R, Ninomiya M, Morita K, Tomino T, Oshiro Y, Tomoyuki Yokota 4, et al. Branch-type intraductal papillary neoplasm of the bile duct treated with laparoscopic anatomical resection: a case report. Surg Case Rep. 2020;6(1):103.
21. Franken C, Lau B, Putchakayala K, DiFronzo LA. Comparison of short-term outcomes in laparoscopic vs open hepatectomy. JAMA Surg. 2014;149(9):941-6.
Full Text Sources:
Abstract:
Views: 2374

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.