Surgery, Gastroenterology and Oncology

|
|
Introduction: Cervical cancer (CC) continues to be a significant problem in Bulgaria, with very high morbidity and mortality. The reasons for this are manifold – besides the lack of
primary prevention and screening, there are also issues related to the treatment process. This study aims to collect results and analyses data on the initial management of CC, focusing on preoperative radiotherapy and its negative impact on the survival of patients with this type of cancer in Bulgaria.
Materials and methods: This is a retrospective population-based study of all patients with histologically confirmed CC registered in the Bulgarian National Cancer Registry (BNCR) between 01.01.2019 and 31.12.2022. Information on the types of initial treatment was collected. Patients whose first-line treatment was preoperative radiotherapy were analysed.
Results: A total of 3 193 women with CC were registered in the BNCR, of whom 169 had no data on histological diagnosis. In 232 of all other 3024 patients (7.26%), the first treatment modality was preoperative radiotherapy. A total of 129 patients from those 232 (4.04%) had evidence of subsequent surgery after preoperative radiotherapy, the remained 2792 were treated by other treatment modalities.
Conclusions: Preoperative radiotherapy has no routine designated place in the treatment of this particularly lethal for Bulgarian women cancer. Avoiding the combined use of surgery and preoperative radiotherapy means achieving improved oncological outcomes for cervical cancer in Bulgaria as early as 2024.
Introduction
Cervical carcinomas (CC) in Bulgaria continue to be a significant cancer disease, occupying the fourth place in morbidity and mortality among all cancer sites (1). The incidence of this oncological nosology is decreasing in developed countries but remains high in developing countries, with 604 000 new diagnoses and 340 000 deaths in 2020 (2). These figures suggest a 5.7% increase in the incidence and an 8.9% increase in mortality in 2018 alone (1).
The statistics concerning Bulgaria are alarming. According to the GLOBOCAN database for Bulgaria, the estimated age-standardised incidence rate of CC for 2020 is 18.3 per 100 000 (6), which is among the highest in Europe. Additionally, Bulgaria has the third highest age-standardised mortality rate (1), with a five-year survival rate that is at least 10% lower than the survival of patients in Western countries (3).
These results have multiple underlying causes, most of which have been the subject of numerous publications and discussions: the absence of sufficient primary prevention measures and the lack of a nationwide screening program (4).
This article aims to collect results and analyse data on the initial management of CC, focusing on preoperative radiotherapy and its negative impact on the survival of patients with this type of cancer in Bulgaria.
Materials and methods
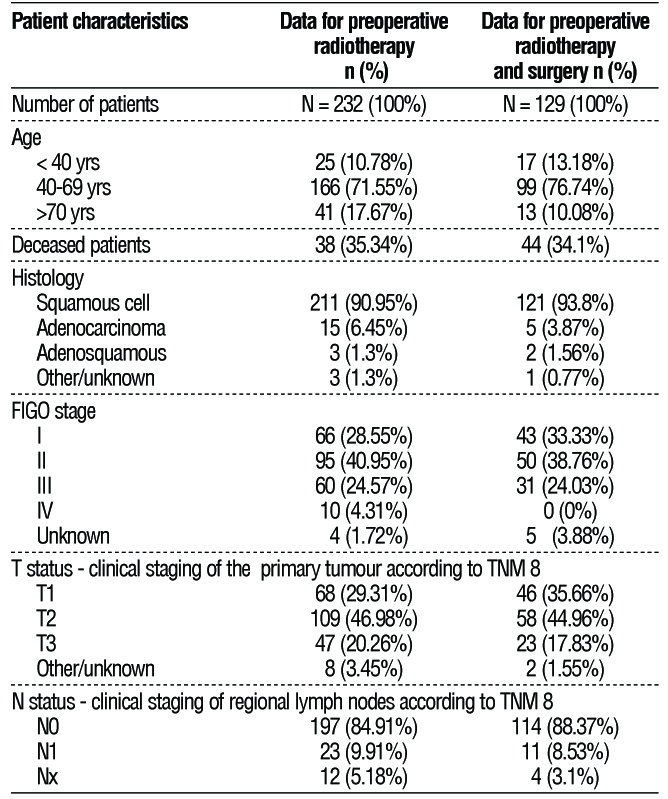
This is a retrospective population-based study of all patients with histologically confirmed CC registered in the Bulgarian National Cancer Registry (BNCR) between 01.01.2019 and 31.12.2022. All enrolled patients had a histologically confirmed diagnosis of cervical cancer. Information on the types of initial treatment (surgery, radiotherapy, radiation chemo-therapy or chemotherapy) was collected. Patients whose first-line treatment was preoperative radiotherapy were analysed. Study parameters and follow-up information about the cancer disease: clinical (age at diagnosis) and pathological characteristics of the cancer disease (histological type, T- and N-stage according to the Eighth Edition of TNM (5) and FIGO 2018 classification (6), differentiation grade (grading G). Data on patients treated with pre-operative radiotherapy and subsequent surgery were analysed. Patients were followed up until 01.04.2023 with information on the stage of cancer diagnosis, initial treatment and mortality. The information was obtained from the BNCR after formal authorisation.
Data analysis
Clinicopathological characteristics were summarised by frequency and percentages. The last analysed patient was included before December 31st, 2021. The date of the last data collection was September 1st, 2023. Correlations between the following biomarkers and clinical parameters were measured: age and treatment method with a graphical statistics display. Multivariate analyses were also performed to assess the impact of disease stage, age at diagnosis, and type of treatment administered on the overall survival rate.
Table 1 - Characteristics of the patients included in the study
Results
A total of 3 193 women with CC were registered in the BNCR for the period 01/01/2019 – 31/12/2022, of whom 169 had no data on histological diagnosis. In 232 of all other 3024 patients (7.26%), the first treatment modality was preoperative radiotherapy. A total of 129 patients from those 232 (4.04%) had evidence of subsequent surgery after preoperative radiotherapy, the remained 2792 were treated by other treatment modalities. The minimum follow-up of patients was 10 months, with a median follow-up of 18 months.
Table 1 summarises the patients' baseline clinicopathological characteristics.
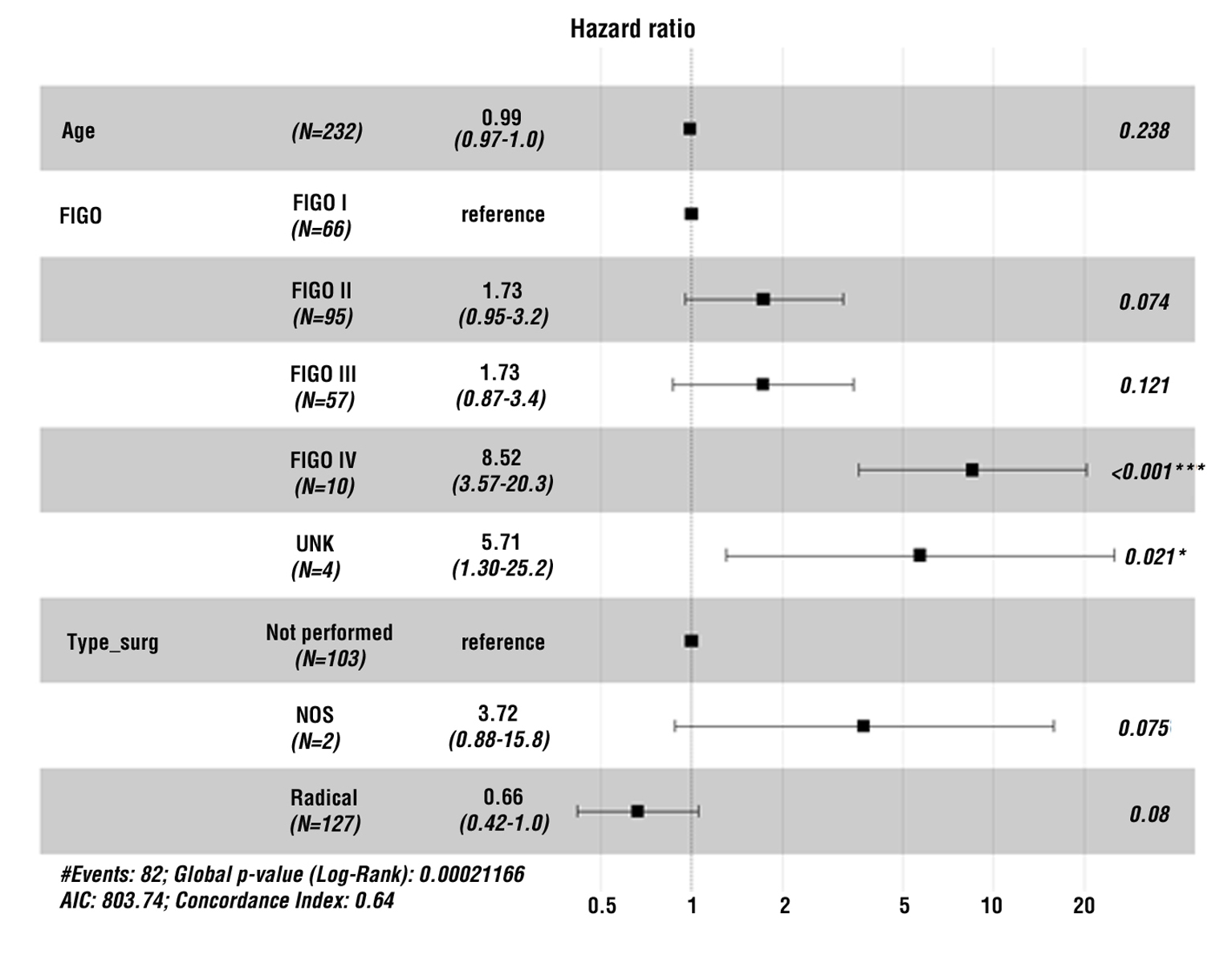
Analyses to assess the overall survival according to various parameters were also performed. Cox regression analysis was performed to assess the impact of disease stage (according to the FIGO staging system), as well as the type of treatment performed
(fig. 1).
Figure 1 - Summary of multivariate Cox regression analysis of overall survival as a function of three variables: age, FIGO stage, and type of surgery. Patients in FIGO stage IV have a statistically significant higher risk of lethality. On the other hand, it is evident that radical surgical intervention does not statistically significantly reduce the risk of lethality compared to patients who did not undergo surgery
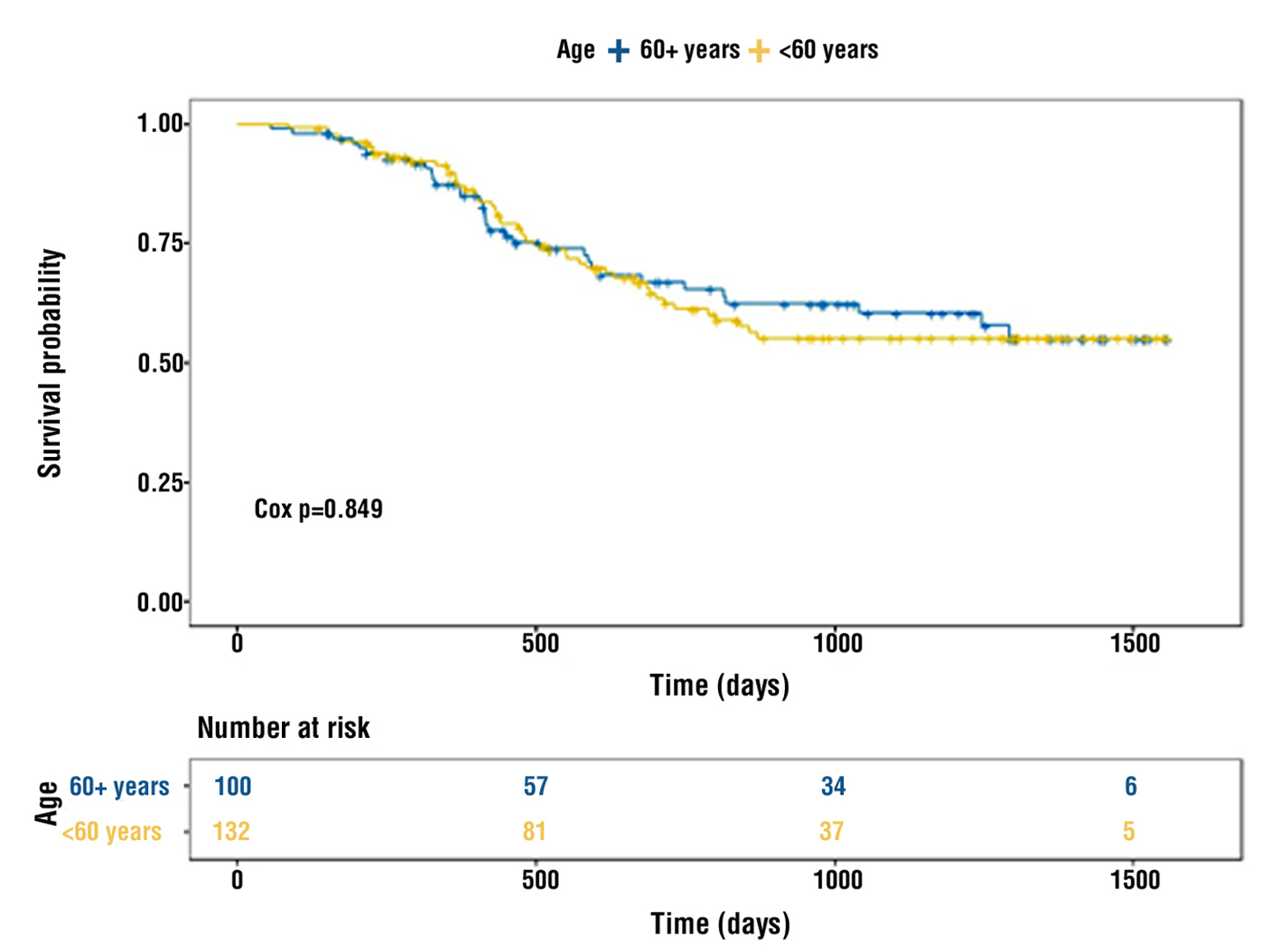
There was no statistical significance for the correlation between age at diagnosis (below and ≥ 60 years) and overall survival (Cox p = 0.849), and this is reflected in fig. 2.
Figure 2 - Overall survival according to age at diagnosis: under, at and over 60 years of age.
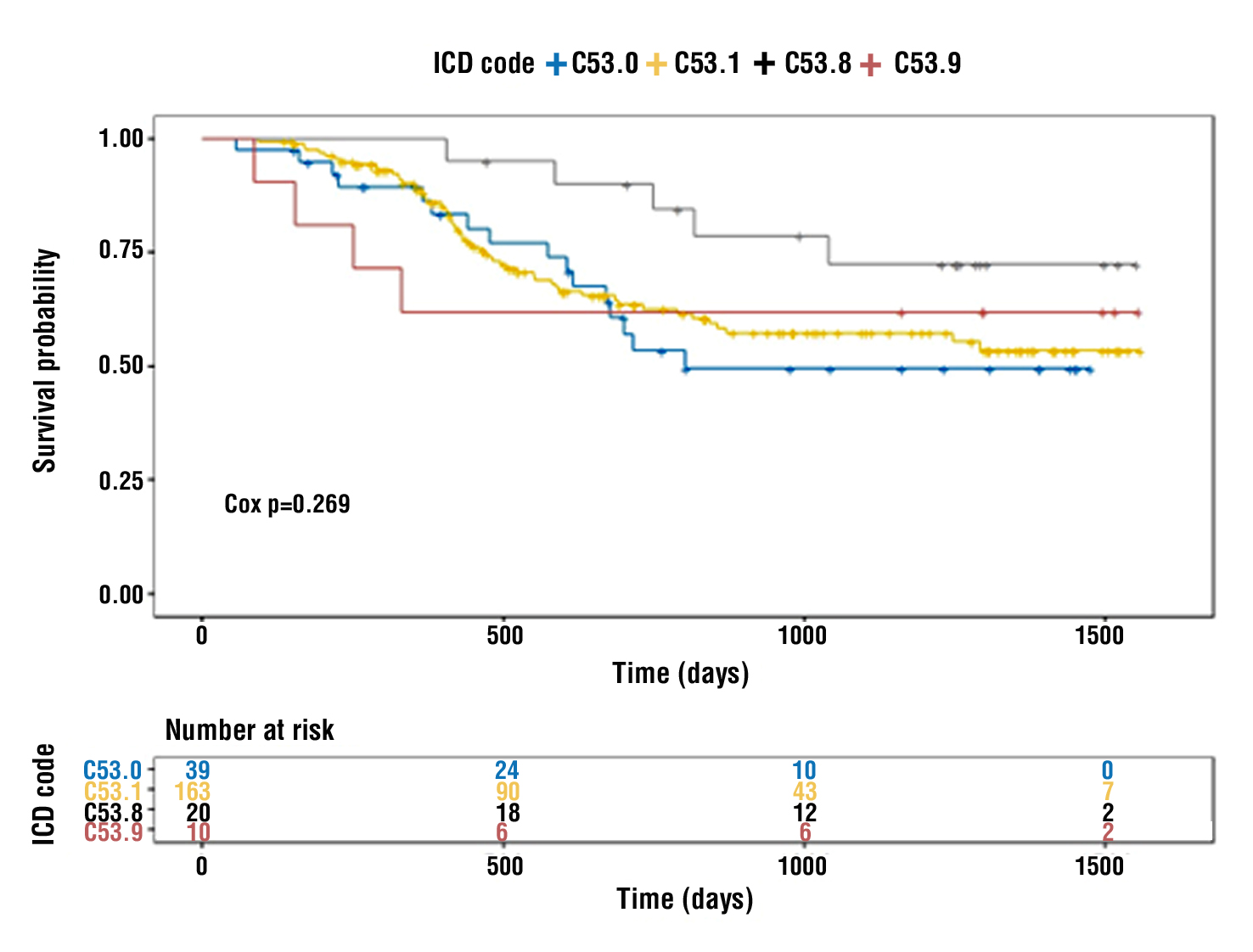
Survival according to the localisation of the oncological process is distributed according to the International Classification of Diseases, Tenth Revision (ICD-10), and there is no statistical significance (Cox p=0.269), which is reflected in fig. 3.
Figure 3 - Overall survival according to localisation of carcinoma in the cervix: C 53.0 – endocervical carcinoma, C 53.1 – exocervical carcinoma, C 53.8 – carcinoma extending beyond one region of the cervix, C 53.9 – unspecified cervical carcinoma
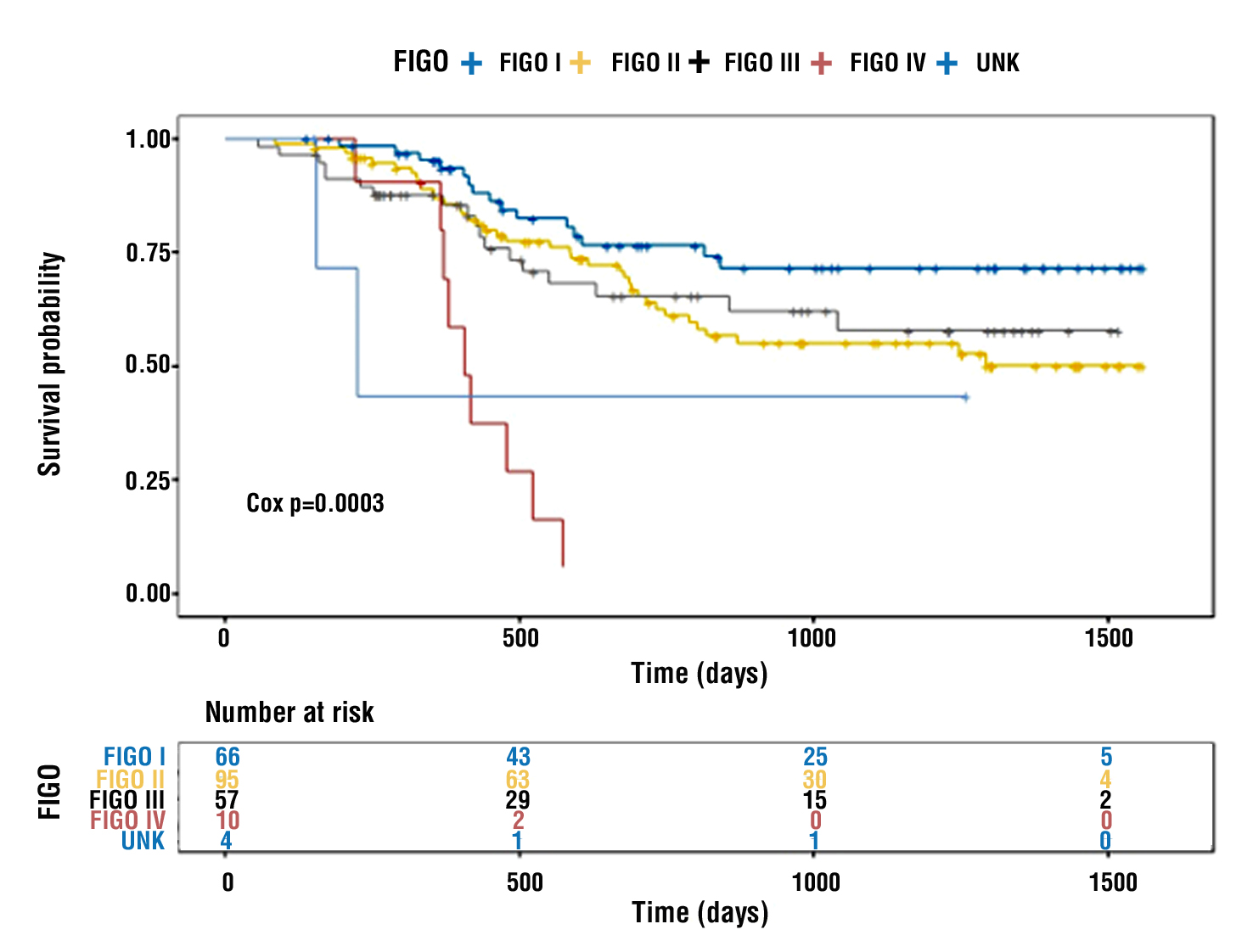
Stage at diagnosis had a statistically significant effect on overall survival (Cox p = 0.003), as shown in fig. 4.
Figure 4 - Overall survival according to disease stage (FIGO)
Statistical methods
All tests were implemented using R statistical environment for Windows (version 4.2.0). All plots were generated using R packages ggpubr (v. 0.4.0) and ggplot2 (v. 3.3.5).
Discussion
Radiotherapy is the primary treatment modality for cervical cancer, and together with radiation, chemotherapy, and surgery are the methods of definitive initial treatment. The goal of definitive treatment is a complete cure and is applied early in the course of cancer, especially in CC. Combining surgery with radiotherapy (regardless of whether or not concurrent chemotherapy is administered) results in a significant increase in complication rates. Therefore, the initial definitive approach (radiotherapy or surgery), rather than their combined sequential administration, is debated in the scientific literature (7,8). In the initial primary surgical treatment, adjuvant therapy is administered in the presence of residual disease (positive resection lines, residual metastatic lymph nodes, etc.) or risk factors for recurrence (tumour size greater than 4 cm, metastatic lymph nodes removed, deep stromal invasion, lymphovascular invasion), with combined radiochemotherapy being preferred (7). The opposite approach, initial radiation (chemotherapy) followed by surgery, leads to a significant increase in complication rates and does not improve overall survival.
For this reason, it is not recommended as an approach, even for residual persistent disease, after initial definitive radiotherapy (7-17). A crucial principle guiding all therapeutic decisions – at every stage and time point, is the goal of avoiding the risk of combining the two modalities of surgery and radiotherapy. These data have been well-established for a considerable period of time – since 2012 (8,15,16), yet combined treatment is still applied in Bulgaria as a planned strategy rather than an exception.
There are not many studies available in the literature showing the effect of preoperative radiotherapy followed by surgery, and those that have been published usually report the pathological features of the tumour after treatment. Li et al. reported that the incidence of deep stromal invasion and lymphovascular invasion was reduced after preoperative radiotherapy. However, the incidence of lymphogenous metastasis, parametrial invasion, and resection-line involvement was not decreased (9). Gauci et al. followed 61 patients with preoperative radiotherapy and concluded that this method could be used in early-stage CC with poor prognostic markers (10). Zhang et al. compared two groups of patients – with preoperative radiotherapy followed by surgery and surgery alone, and concluded that there was no significant difference in complications, survival and operative time; preoperative radiotherapy did not improve postoperative pathology but significantly improved locoregional control (11). A weakness and peculiarity of most studies is that they compare preoperative radiotherapy with subsequent surgery versus surgery alone rather than preoperative radiotherapy with subsequent surgery versus radiotherapy alone. Another peculiarity is that most papers deal with preoperative radiotherapy in treating early CC, whereas in Bulgaria, it is mainly used in advanced cases. From the available data from Bulgaria and the above analyses, it is evident that the primary age group in which pre-operative radiotherapy is applied in Bulgaria is between 40 and 69 years of age – 71.6 – 76.7. The most frequent histology is squamous cell carcinoma – over 90% of cases, and preoperative radiotherapy is most often performed in FIGO stage 2 patients, respectively cT2, according to TNM 8 classification. Radiotherapy followed by surgery is administered at any stage of diagnosis, including FIGO 3, and in a significant percentage of cases without complete initial staging.
Evidence-based guidelines for the management of CC, including ESGO (7), ESMO (16) and NCCN (17), routinely recommend against preoperative radiotherapy and explicitly emphasise that the combination of radiotherapy and surgery should be avoided as initial treatment, regardless of the early stage of disease in CC. Unfortunately, the BNCR data for Bulgaria presented above show a significant difference. This strategy and the alarming data on the lowest overall survival confirm evidence-based medicine. One in three patients treated with preoperative radiotherapy and subsequent surgery die very quickly afterwards, with mortality rates in early CC exceeding 34%. It should be noted that the follow-up period is very short, and a longer follow-up, which will be the subject of a subsequent analysis and publication, would probably report similar and even worse results. A total of 82 women died during the follow-up, which is 35.34% of the total. When considering only the group of patients with data on subsequent surgical treatment, the number of deceased patients was 44 (34.1%).
It should also be noted that even when a patient with preoperative radiotherapy does not undergo subsequent surgical treatment but completes radiotherapy, the results are not good. This is due to the interruption of treatment for a reassessment of the patient, resulting in significantly worse overall survival.
Notably and encouragingly, the percentage of preoperative radiotherapy did decline during the study period, accounting for 7.26% of all registered cases and only 4.04% of registered cases for which information on subsequent surgical treatment was available during the period. In comparison, for the period 2015 – 2018, these figures were 11.86% and 7.2%, respectively (for this period, a total of 3 928 patients were registered, 466 underwent preoperative radiotherapy, and for 283, there was data on subsequent surgical treatment). A possible explanation, however, would be the incomplete registration of new cases in the last 4 years by the BNCR.
Conclusion
The treatment of early stages of cervical cancer aims at a cure, which is achieved by administering radical treatment – definitive radiation (chemo)therapy or surgery. A primary goal of treatment planning is to construct a therapeutic strategy that minimises the percentage of patients treated by the two methods sequentially. For this reason, baseline complete and adequate staging of the disease (systemic and loco-regional), as well as treatment in a multidisciplinary team experienced in gynecologic oncology with access to all treatment modalities, including radiotherapy, systemic treatment, and gynecologic oncology, may be factors of positive importance in improving survival of patients with cervical cancer in Bulgaria. Preoperative radiotherapy has no routine designated place in the treatment of this particularly lethal for Bulgarian women cancer, especially in advanced non-metastatic disease. Avoiding the combined use of surgery and preoperative radiotherapy means achieving improved oncological outcomes for cervical cancer in Bulgaria as early as 2024.
Conflict of interest
The authors declare no conflict of interest.
Funding
Bulgarian National Science Fund: MeMoMi: Mechanisms of Modulating the immune response in the tumor and its Microenvironment for development of prognostic groups and optimizing the treatment algorithm in patients with cancer of the uterine cervix.
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Medical University Pleven (protocol code 656/29.06.2021).
References
- Arbyn M, Weiderpass E, Bruni L, de Sanjosé S, Saraiya M, Ferlay J, Bray F. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8(2):e191-e203.
2.Cancer Today. Available online: https://gco.iarc.fr/today/fact-sheets-cancers (accessed on 3 February 2023).
3.Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikši? M et al; CONCORD Working Group. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37?513?025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018; 391(10125):1023-1075.
4.Yordanov A, Vasileva-Slaveva M, Galai N, Faraggi D, Kubelac MP, Tripac-Iacovleva I et al. Cancer of the Cervix in Bulgaria: Epidemiology of a Crisis. Healthcare 2023; 11(3):318.
5.https://qxmd.com/calculate/calculator_771/cervical-cancer-tnm-staging (accessed on 20 April 2023)
6.Salib MY, Russell JHB, Stewart VR, Sudderuddin SA, Barwick TD, Rockall AG et al. 2018 FIGO Staging Classification for Cervical Cancer: Added Benefits of Imaging. Radiographics 2020;40(6): 1807-1822.
7.Cibula D, Raspollini MR, Planchamp F, Centeno C, Chargari C, Felix A et al. ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer - Update 2023. Int J Gynecol Cancer. 2023;33(5):649-666.
8.Geetha P, Nair MK. Laparoscopic, robotic and open method of radical hysterectomy for cervical cancer: a systematic review. J Min Access Surg 2012; 8:67–73
9.Li W, Liu P, Zhao W, Yin Z, Lin Z, Bin X et al. Effects of preoperative radiotherapy or chemoradiotherapy on postoperative pathological outcome of cervical cancer--from the large database of 46,313 cases of cervical cancer in China. Eur J Surg Oncol. 2020;46(1):148-154
10.Gauci PA, Kee DLC, Thamphya B, Schiappa R, Delotte J, Chand-Fouche ME et al.Preoperative high-dose-rate brachytherapy for high-risk early-stage cervical cancer: Long-term clinical outcome analysis. Brachytherapy. 2022;21(3):273-282
11.Zhang T, Kong W, Li F, Song D, Liu T, Han C et al. Effect of preoperative radiotherapy on stage IB2 and IIA2 cervical cancer: A retrospective cohort study. Int J Surg 2016;30:63-7
12. Arbyn M, Weiderpass E, Bruni L, de Sanjosé S, Saraiya M, Ferlay J et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8(2):e191-e203
13. Dyba T, Randi G, Bray F, Martos C, Giusti F, Nicholson N et al. The European cancer burden in 2020: Incidence and mortality estimates for 40 countries and 25 major cancers. Eur J Cancer. 2021;157:308-347.
14. Das M. WHO launches strategy to accelerate elimination of cervical cancer. Lancet Oncol. 2021;22:20–1.
15. Cibula D, Pötter R, Planchamp F, Avall-Lundqvist E, Fischerova D, Haie Meder C et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/ European Society of Pathology Guidelines for the Management of Patients With Cervical Cancer. Int J Gynecol Cancer. 2018;28(4): 641-655.
16. Marth C, Landoni F, Mahner S, McCormack M, Gonzalez-Martin A, Colombo N; ESMO Guidelines Committee. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017 Jul 1;28(suppl_4):iv72-iv83.
17. NCCN Clinical practice guidelines v1.2024 (accessed on 3 February 2024).
Full Text Sources:
Abstract:
Views: 3417

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.