Surgery, Gastroenterology and Oncology

|
|
Background: Blunt abdominal trauma (BAT) is a common cause of intra-abdominal injury, with the spleen being the most frequently affected organ. In resource-limited settings, understanding injury patterns and management strategies is crucial for improving outcomes. Objective: To assess the prevalence, injury patterns, and clinical management of splenic injuries in patients with BAT.
Methods: A cross-sectional study was conducted at Al Nasiriya Teaching Hospital between April 1, 2024, and April 1, 2025. A total of 93 patients with splenic injury confirmed by imaging or surgical findings were included. Data on demographics, trauma mechanism, imaging findings, injury grade (AAST), associated injuries, and treatment approach were analyzed using SPSS version 26.
Results: The majority of patients were males (62.4%), with the highest prevalence observed in the 20-29 age group. Ultrasound was used in 60.2% of cases and CT in 35.5%. Grade 3 injuries were most frequent (38%), followed by Grade 2 (28%). Associated abdominal injuries occurred in 38.7%, mainly liver injuries (55.9%), while 40.9% had extra-abdominal injuries. Surgical intervention was performed in 92.5% of cases, and conservative management in 15%, primarily in low-grade injuries.
Conclusion: Splenic injury following BAT predominantly affects young males and often necessitates surgical intervention in low-resource settings. Broader adoption of non-operative management requires enhanced radiological and monitoring capacities.
INTRODUCTION
Blunt abdominal trauma (BAT) is a major contributor to trauma-related morbidity and mortality worldwide. It often results from motor vehicle collisions, falls, or assaults, and accounts for approximately 75% of abdominal injuries (1). Among intra-abdominal organs, the spleen is the most frequently injured due to its high vascularity and anatomical location in the left upper quadrant (2). The spleen plays vital hematologic and immunologic roles and is protected by splenic ligaments, including the gastrosplenic and splenorenal ligaments, although its friable parenchyma makes it susceptible to trauma (3). Splenic injury risk varies with age, trauma mechanism, and the degree of impact. Studies report a prevalence of splenic injuries ranging from 25% to 50% in patients with BAT (4,5), with a higher incidence in younger individuals due to increased exposure to high-energy trauma and reduced thoracic protection (6).
Splenic trauma may result from direct compression, such as seatbelt injuries, or from deceleration forces leading to vascular avulsion or parenchymal laceration (7). Clinical presentation may include abdominal pain, signs of hypovolemia, or referred shoulder pain (Kehr’s sign), indicating diaphragmatic irritation due to hemoperitoneum (8). Diagnosis often involves a physical examination alongside imaging, particularly Focused Assessment with Sonography for Trauma (FAST), which is a rapid and non-invasive technique, and contrast-enhanced computed tomography (CT), which remains the gold standard for grading injuries (9). CT allows classification based on the American Association for the Surgery of Trauma (AAST) system, ranging from Grade I (minor lacerations) to Grade V (shattered spleen or hilar vascular injury), which helps determine the optimal treatment approach (10,11).
Management has evolved from splenectomy to a preference for non-operative management (NOM) in hemodynamically stable patients, with success rates exceeding 90% in selected case (12).
However, in resource-limited settings, surgical intervention is still common due to lack of radiologic support and intensive care infrastructure. When surgery is necessary, splenic preservation techniques, such as partial splenectomy or splenic artery embolisation, are increasingly used to preserve immune function (13). Complications of splenic trauma include delayed rupture and overwhelming post-splenectomy infection (OPSI), emphasizing the importance of follow-up care and immunization against encapsulated organisms like Streptococcus pneumoniae and Haemophilus influenzae (14-16).
Epidemiological studies of splenic injuries are vital to guide resource allocation, improve management protocols, and support preventive strategies. This study was conducted to evaluate the prevalence, clinical characteristics, and outcomes of splenic injuries due to BAT in a tertiary care setting in southern Iraq.
METHODOLOGY
This prospective cross-sectional study was conducted at Al Nasiriya Teaching Hospital, a major referral center in southern Iraq, over one year from April 1, 2024, to April 1, 2025. The study included all patients presenting with blunt abdominal trauma who were diagnosed with splenic injury based on imaging (FAST or CT scan) or confirmed intraoperatively. Patients with penetrating injuries, pre-existing splenic pathology, or incomplete records were excluded.
A total of 93 patients were enrolled using convenience sampling based on trauma registry data and prior literature regarding the prevalence of splenic injuries. Data were collected from medical charts, imaging reports, operative notes, and follow-up records. Recorded variables included demographics, mechanism of injury, clinical findings, imaging modality, AAST injury grade, associated injuries, and management approach. Patient assessment followed Advanced Trauma Life Support (ATLS) protocols. Hemodynamically stable patients underwent CT scanning, while unstable patients were assessed by FAST and taken to surgery if necessary.
Operative procedures included splenectomy or spleen-preserving techniques depending on injury grade and patient condition. Conservative management was applied in stable cases with low-grade injuries and included ICU monitoring, bed rest, serial hemoglobin testing, and follow-up imaging.
Data were anonymized and entered into a secure electronic database. Ethical approval was obtained from the College of Medicine, University of Thi-Qar, and the Thi-Qar Health Directorate. Statistical analysis was conducted using SPSS version 26. Descriptive statistics were used for frequency distribution, while chi-square and t-tests were applied to compare categorical and continuous variables, respectively, with a significance level set at p < 0.05.
RESULTS
The study included a total of 93 patients with splenic injury.
Fig. 1 shows the age distribution of the patients. The majority of cases occurred in the age group of 20-29 years, followed by those aged 10-19 years and 30 to 39 years. Fewer cases were reported in the age groups above 40 years, with the lowest frequency in patients older than 50 years.
Fig. 2 presents the gender distribution of the patients. Males constituted the majority of cases, accounting for 58 (62.4%) of the patients, while females represented 35 (37.6%).
Fig. 3 illustrates the imaging modalities used for diagnosing splenic injuries. The US was the most frequently used modality, applied in 56 (60.2%) of the cases. A CT scan was used in 33 (35.5%) of the patients, while Explorative laparotomy was used in 4 (4.2%).
Fig. 4 demonstrates the grades of splenic injury based on CT findings according to the AAST grading system. Grade 3 injuries were the most frequent overall, 30 (38%), followed by Grade 2, 26 (28%), Grade 4 18 (19.4%), Grade 1, 11 (11.85%), and Grade 5, 8 (8.6%).
Figure 1 - Age (in years) distribution of splenic injury patients Figure 2 - Gender distribution of splenic injury patients
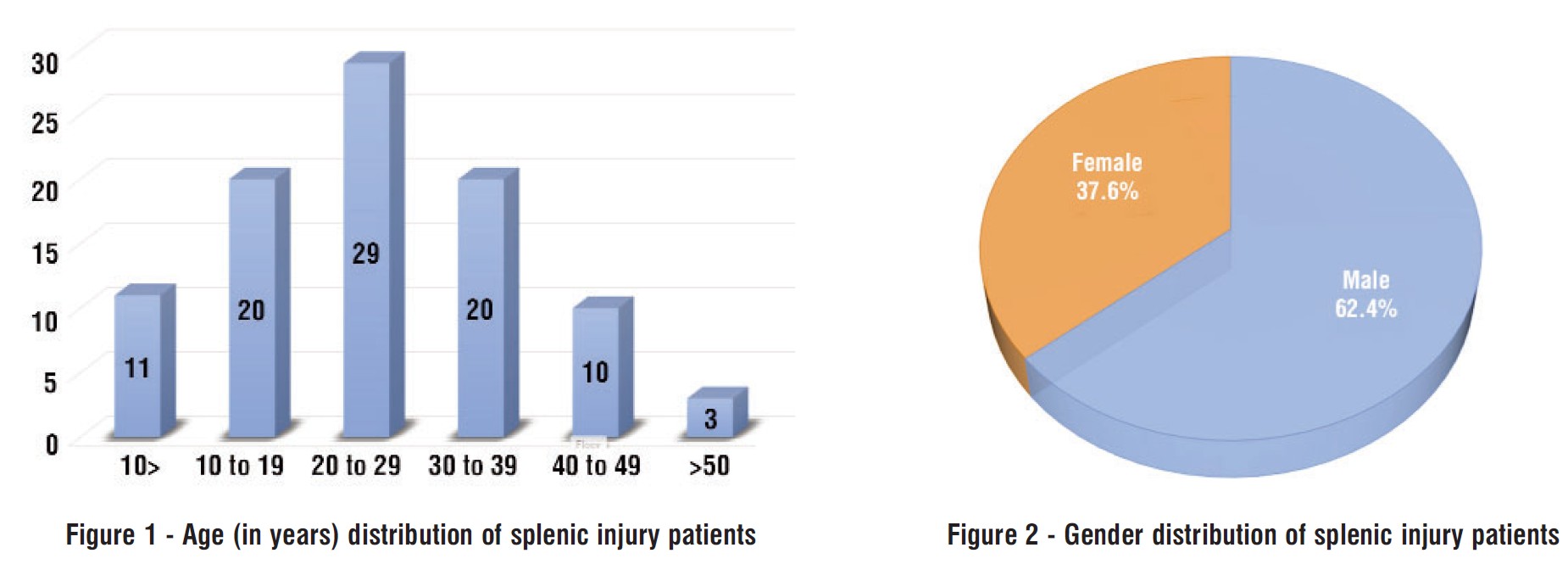
Figure 3 - Modalities used to diagnose the splenic injury
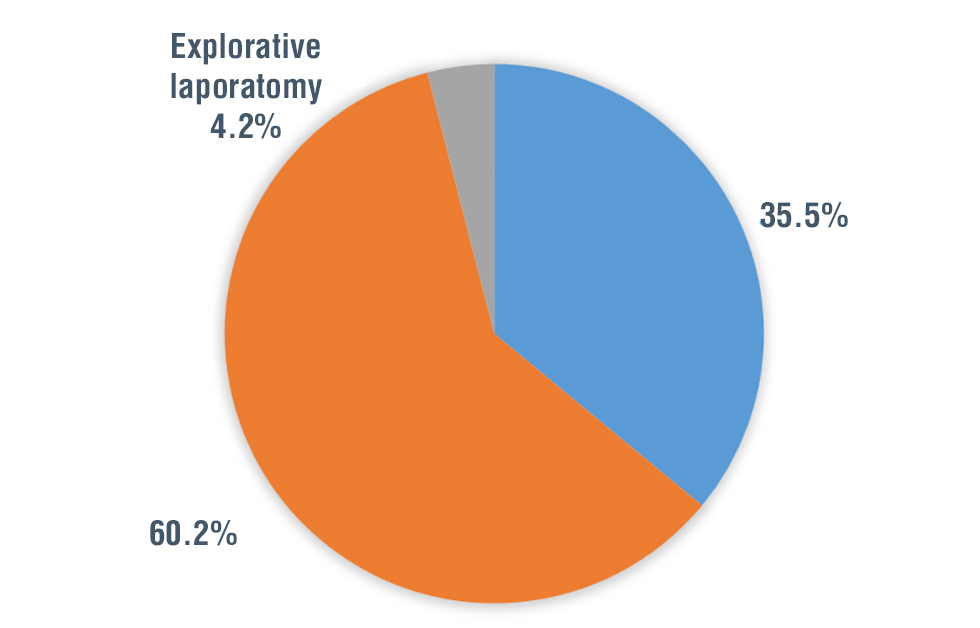 Table 1 - Associated injuries in splenic-injured patients Figure 4 - Grades of splenic injury based on CT scan findings according to the AAST grading system In a cohort of splenic-injured patients, 38.7% had associated abdominal injuries, with liver injuries being the most common (55.9%), followed by left kidney hematomas (29%), bowel injuries (20.4%), vascular injuries (11.8%), bladder injuries (10.8%), and urethral injuries (2.1%). Extra-abdominal injuries were present in 40.9% of patients, most frequently hemothorax and pneumothorax (33.4%), rib fractures (24.7%), and diaphragmatic injuries (6.5%). Notably, 25.8% of patients had no associated injuries. These findings highlight the high incidence of concomitant injuries in splenic trauma, emphasizing the need for thorough evaluation in such cases (table 1).
Table 1 - Associated injuries in splenic-injured patients Figure 4 - Grades of splenic injury based on CT scan findings according to the AAST grading system In a cohort of splenic-injured patients, 38.7% had associated abdominal injuries, with liver injuries being the most common (55.9%), followed by left kidney hematomas (29%), bowel injuries (20.4%), vascular injuries (11.8%), bladder injuries (10.8%), and urethral injuries (2.1%). Extra-abdominal injuries were present in 40.9% of patients, most frequently hemothorax and pneumothorax (33.4%), rib fractures (24.7%), and diaphragmatic injuries (6.5%). Notably, 25.8% of patients had no associated injuries. These findings highlight the high incidence of concomitant injuries in splenic trauma, emphasizing the need for thorough evaluation in such cases (table 1). 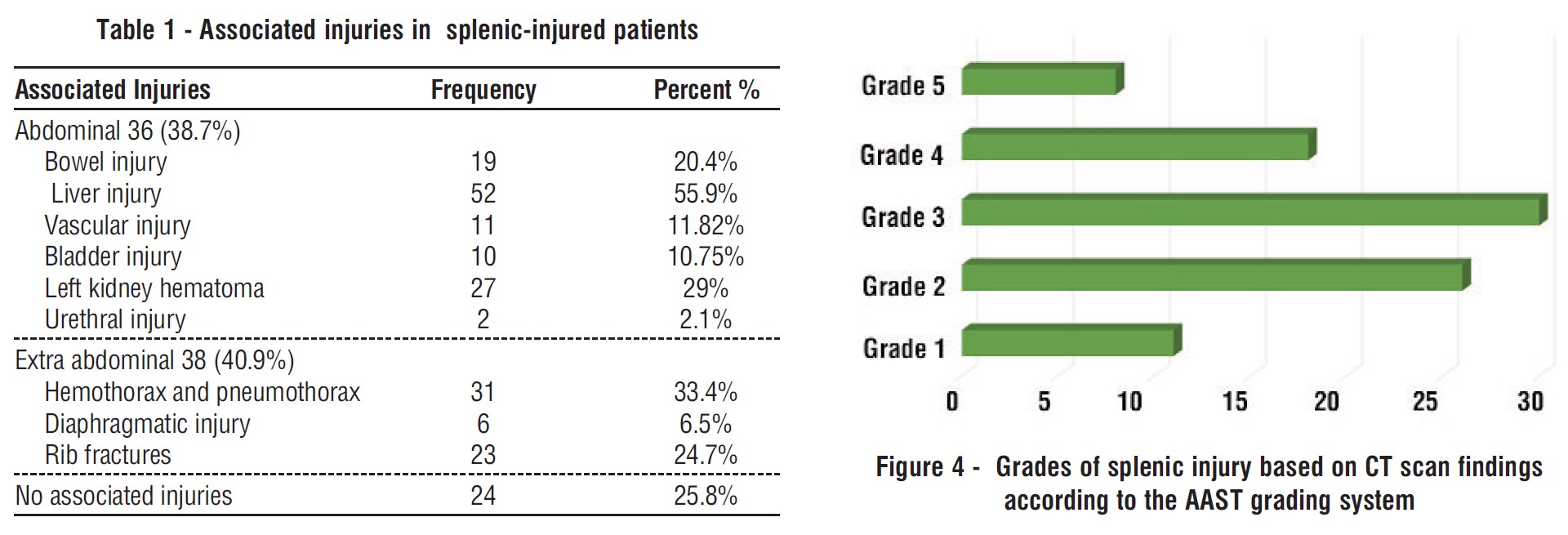
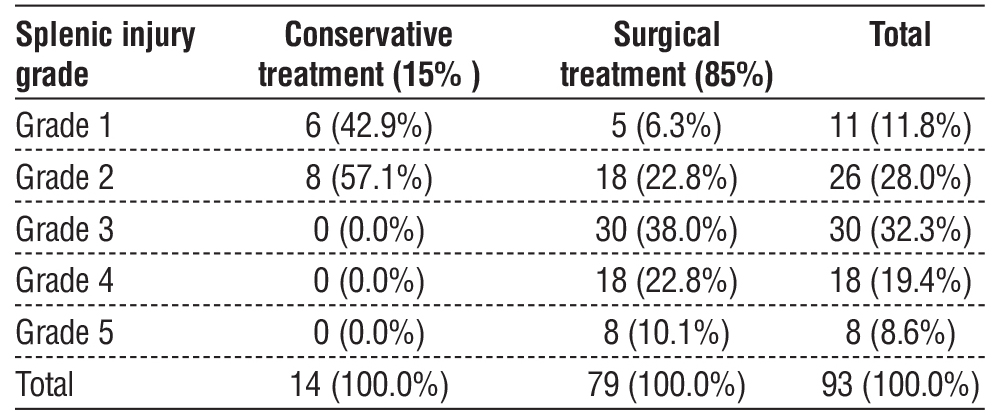
Table 2 presents the treatment modalities according to splenic injury grade. In a total of 93 patients with splenic injury, conservative treatment was employed in 15% of cases (n = 14), while surgical treatment was used in the remaining 85% (n = 79). Conservative management was limited to lower-grade injuries, with 42.9% of Grade 1 and 57.1% of Grade 2 injuries managed non-operatively. In contrast, all Grade 3, 4, and 5 injuries were treated surgically, comprising 38.0%, 22.8%, and 10.1% of the surgical cases, respectively. This distribution indicates a clear trend toward surgical intervention with increasing injury severity.
Table 2 - Type of treatment used for splenic injury by injury grade
DISCUSSION
Trauma remains a leading cause of both mortality and morbidity worldwide and is increasingly recognized as a global health epidemic. Among the various anatomical regions affected, the abdomen is one of the most commonly involved in traumatic injuries (17). Blunt abdominal trauma (BAT) and penetrating abdominal trauma together account for approximately 7–10% of trauma-related deaths, with splenic and hepatic injuries being major contributors due to their high risk of intra-abdominal hemorrhage and associated mortality rates reaching up to 42% (18). This study aimed to evaluate the demographic distribution, diagnostic approaches, injury severity, associated injuries, and management strategies in patients with splenic injuries secondary to BAT.
A strong male predominance (62.4%) was observed, with the highest incidence occurring in the 20–29-year age group. This finding aligns with previous studies, including a large series by Peitzman et al. (19), which reported a similar demographic trend—males aged 20–40 years—likely reflecting increased exposure to high-energy trauma mechanisms such as road traffic accidents and interpersonal violence.
Ultrasound was the most frequently utilized diagnostic modality (60.2%), followed by computed tomography (CT) at 35.5%, and laparotomy in a minority of cases (4.2%). This distribution is typical of resource-limited settings, where ultrasonography is often prioritized due to its accessibility, cost-effectiveness, and utility at the bedside—particularly in hemodynamically unstable patients (20). In contrast, in high-resource environments, CT imaging is employed in over 90% of trauma evaluations, as demonstrated in a large multicenter U.S. study (21), reflecting its widespread availability and the value of detailed injury characterization.
Grade 3 splenic injuries were the most commonly observed (38%), followed by Grades 2 and 4. This injury distribution is consistent with findings from the Eastern Association for the Surgery of Trauma (EAST) multi-institutional trial, which reported Grades 2 and 3 as the most prevalent (22). Notably, Grade 3 injuries often represent a clinical decision-making threshold, where the choice between operative and non-operative management becomes particularly complex—especially in settings with limited resources for continuous monitoring and advanced imaging.
Associated injuries were identified in 38.7% of blunt abdominal trauma (BAT) cases, with the liver being the most frequently involved organ (55.9%). This aligns with prior studies identifying the liver and spleen as the most commonly injured solid organs in BAT (23,24). Extra-abdominal injuries—such as rib fractures, hemothorax, and pneumothorax—were also commonly observed, reflecting the high-energy mechanisms typically involved. Similarly, Haan et al. (25) reported thoracic injuries in approximately one-third of patients with splenic trauma, emphasizing the importance of a comprehensive evaluation to detect concurrent injuries.
Surgical intervention was performed in 92.5% of cases, while conservative management was employed in only 15%, primarily in patients with low-grade injuries. All Grade 3 and higher injuries were managed operatively. These findings contrast with practices in high-resource settings, where non-operative management (NOM) is widely adopted for Grades 1–3, and even selectively for Grades 4–5. For example, Stassen et al. (26) reported NOM success rates exceeding 80% for Grades 1–3 in centers equipped with interventional radiology and intensive monitoring capabilities. The high rate of operative management in this study likely reflects local constraints, including limited access to CT imaging, blood products, and continuous observation facilities.
Comparable trends have been reported in other Iraqi studies. Hatam et al. (27), for instance, documented surgical management in 81% of patients with splenic injuries, attributing the limited use of NOM to inadequate imaging infrastructure and ICU availability. These findings highlight the necessity of tailoring trauma care protocols to the capabilities and limitations of the local healthcare system.
Our findings underscore the importance of developing context-specific management protocols that consider both the severity of injury and the resources available within each institution. While high-resource centers are able to safely implement non-operative management (NOM) in up to 60–70% of splenic injury cases (28), operative intervention remains the standard approach in settings lacking the infrastructure for close hemodynamic monitoring, repeat imaging, and interventional radiology. Adapting management strategies to local capabilities is essential to optimize patient outcomes and ensure safe, effective trauma care.
CONCLUSION
This study confirms that splenic injuries resulting from blunt abdominal trauma (BAT) predominantly affect young adult males and are most frequently managed surgically in resource-limited settings. Grade 3 injuries were the most common and often required operative intervention. While global trends increasingly support non-operative management (NOM), its success is highly dependent on institutional resources, including access to advanced imaging, intensive care facilities, and trained clinical personnel. Expanding the use of NOM in such settings will require parallel investments in healthcare infrastructure, workforce development, and the implementation of standardized clinical protocols to ensure patient safety and optimize outcomes.
Author’s Contributions
All authors contributed to the study design, data analysis, and manuscript preparation. All approved the final version.
Competing Interests
The authors declare that there are no conflicts of interest related to this work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethics Approval and Consent to Participate
Ethical approval was granted by Ethical approval was obtained from the College of Medicine, University of Thi-Qar, and the Thi-Qar Health Directorate. Informed consent from the participants was waived due to the retrospective nature of the study.
Availability of Data and Materials
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
References
1. Patel P, Gadhavi J, Parmar H. A study of blunt and penetrating abdominal trauma, its various patterns of injuries, and its management. International Journal of Medical Science and Public Health. 2016;5(7):1309.
2. Perrotta G, Guerrieri E, Guerrieri M. Splenic trauma: Definition, classifications, clinical profiles and best treatments. Open Journal of Trauma. 2021;5(1):019-36.
3. Catalano OA, Soricelli A, Salvatore M. Spleen anatomy, function and development. Abdominal imaging: Springer; 2013. p. 1479-94.
4. Ismail A, Hassan-Ul-Haque M, Jamaluddin M, Tasneem B, Sagheer S, Khan RA. Intra-Abdominal Solid Visceral Injuries in Adult Patients Presenting with Blunt Abdominal Trauma. Annals of Abbasi Shaheed Hospital and Karachi Medical & Dental College. 2020;25(4):231-7.
5. Arshad R, Khan A, Bhatti SG, Chandio MMA, Nasir S, Khatti SN. Prevalence of splenic injury in the blunt abdomen trauma: a cross-sectional study. Pakistan Journal of Medical & Health Sciences. 2023;17(02):382.
6. Akinkuolie AA, Lawal OO, Arowolo OA, Agbakwuru EA, Adesunkanmi ARK. Determinants of splenectomy in splenic injuries following blunt abdominal trauma: trauma. S Afr J Surg. 2010; 48(1):15-9.
7. Lynn KN, Werder GM, Callaghan RM, Sullivan AN, Jafri ZH, Bloom DA. Pediatric blunt splenic trauma: a comprehensive review. Pediatr Radiol. 2009;39(9):904-16; quiz 1029-30.
8. Jabbour G, Al-Hassani A, El-Menyar A, Abdelrahman H, Peralta R, Ellabib M, et al. Clinical and radiological presentations and management of blunt splenic trauma: a single tertiary hospital experience. Med Sci Monit. 2017;23:3383-3392.
9. Miller LA, Mirvis SE, Shanmuganathan K, Ohson AS. CT diagnosis of splenic infarction in blunt trauma: imaging features, clinical significance and complications. Clin Radiol. 2004;59(4):342-8.
10. Dixe de Oliveira Santo I, Sailer A, Solomon N, Borse R, Cavallo J, Teitelbaum J, et al. Grading abdominal trauma: changes in and implications of the revised 2018 AAST-OIS for the spleen, liver, and kidney. Radiographics. 2023;43(9):e230040.
11. Chen H, Unberath M, Dreizin D. Toward automated interpretable AAST grading for blunt splenic injury. Emergency radiology. 2023; 30(1):41-50.
12. Hildebrand DR, Ben-Sassi A, Ross NP, Macvicar R, Frizelle FA, Watson AJM. Modern management of splenic trauma. BMJ. 2014; 348:g1864.
13. Rosati C, Ata A, Siskin GP, Megna D, Bonville DJ, Stain SC. Management of splenic trauma: a single institution’s 8-year experience. Am J Surg. 2015;209(2):308-14.
14. Tahir F, Ahmed J, Malik F. Post-splenectomy sepsis: a review of the literature. Cureus. 2020;12(2):e6898.
15. Zhang J, Zhu G, Liu L, Xu S, Jia C. Delayed Traumatic Splenic Rupture as a Life-threatening Clinical Manifestation Treatable with Splenectomy: A Study of Twelve Cases and Literature Review. Ann Ital Chir. 2025;96(3):296-308.
16. Sinwar PD. Overwhelming post splenectomy infection syndrome -review study. Int J Surg. 2014;12(12):1314-6.
17. Batke M, Cappell MS. Adynamic ileus and acute colonic pseudo-obstruction. Med Clin North Am. 2008;92(3):649-70, ix.
18. Hildebrand F, Winkler M, van Griensven M, Probst C, Musahl V, Krettek C, et al. Blunt abdominal trauma requiring laparotomy: an analysis of 342 polytraumatized patients. European Journal of Trauma. 2006;32:430-8.
19. Peitzman AB, Heil B, Rivera L, Federle MB, Harbrecht BG, Clancy KD, et al. Blunt splenic injury in adults: Multi-institutional Study of the Eastern Association for the Surgery of Trauma. J Trauma. 2000; 49(2):177-87; discussion 187-9.
20. Richards JR, McGahan JP. Focused assessment with sonography in trauma (FAST) in 2017: what radiologists can learn. Radiology. 2017;283(1):30-48.
21. Achatz G, Schwabe K, Brill S, Zischek C, Schmidt R, Friemert B, et al. Diagnostic options for blunt abdominal trauma. Eur J Trauma Emerg Surg. 2022;48(5):3575-3589.
22. Peitzman AB, Heil B, Rivera L, Federle MB, Harbrecht BG, Clancy KD, et al. Blunt splenic injury in adults: multi-institutional study of the Eastern Association for the Surgery of Trauma. J Trauma. 2000;49(2):177-87; discussion 187-9.
23. Abo-Elhoda MF, Attia SM, Ahmed ME, Abdeldaiem KAE. Solid organs injuries in blunt abdominal trauma patients. The Egyptian Journal of Hospital Medicine. 2021;83(1):1477-83.
24. Latif A, Alim M, Khan B, Khan KA, Kumar J. Study of Spleen and Liver Injuries in Patients of Blunt Trauma Abdomen. Pakistan Journal of Medical & Health Sciences. 2022;16(03):320.
25. Haan JM, Bochicchio GV, Kramer N, Scalea TM. Nonoperative management of blunt splenic injury: a 5-year experience. J Trauma. 2005;58(3):492-8.
26. Stassen NA, Bhullar I, Cheng JD, Crandall ML, Friese RS, Guillamondegui OD, et al. Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S294-300.
27. Hatam HA, Nile AK, Abdulshaheed NA. Splenic Injuries atAl-Kadhimiya Teaching Hospital. AL-Kindy College Medical Journal. 2009;5(1):83-90.
28. Meira Júnior JD, Menegozzo CAM, Rocha MC, Utiyama E. Non-operative management of blunt splenic trauma: evolution, results and controversies. Rev Col Bras Cir. 2021;48:e20202777. English, Portuguese
Full Text Sources:
Abstract:
Views: 729

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.