Surgery, Gastroenterology and Oncology

|
|
Background: In patients with papillary thyroid carcinoma (N0), this study compared of unilateral versus bilateral prophylactic central neck dissection on postoperative complications. Also, patients were followed up on postoperative central lymph nodes histopathology to identify the incidence of occult central lymph nodes metastasis on each side independently.
Material and Methods: From April 2022 to April 2024, the study was carried out in Ain Shams University hospitals. Two groups (A & B) were created by randomly dividing fifty patients (simple randomization). Bilateral central neck dissection and a total thyroidectomy were performed on Group A. Group B underwent unilateral central neck dissection along with a total thyroidectomy.
Result: The findings showed that in terms of postoperative complications, there was no statistically significant difference between groups A and B. Nevertheless, group A had a statistically significant higher number of dissected LNs and positive LNs in pathology than group B. Furthermore, the positive LNs in pathology were greater in the patient group with T2 than T1 in both groups.
Conclusion: The current study shows no statistically significant difference in the postoperative complications between the two groups (bilateral PCND versus ipsilateral PCND). Furthermore, in the bilateral PCND group, CND revealed higher lymph nodes metastases. Bilateral PCND seems to be the proper, particularly if the tumor is larger than 2 cm. This is because it ensures that no contralateral lymph nodes are missed, reducing the likelihood of recurrence and the need for further surgery. Unilateral PCND may be better in patients with tumor less than 2 cm because to the low incidence of contralateral paratracheal node metastases.
INTRODUCTION
Thyroid cancer (TC) is becoming more commonplace globally. The majority of thyroid cancers are of the papillary thyroid carcinoma (PTC). Around 35% of patients with PTC had occult cervical lymph node metastases (LNM), which is a common presentation for the majority of these individuals (cN1) (1).
The removal of level VI LNs, which includes the bilateral paratracheal, prelaryngeal, and pretracheal LNs, is known as central neck dissection (CND). When preoperative evaluations of nodal metastases are negative, prophylactic CND is carried out (2).
In order to prevent the complications of reoperation and to provide sufficient staging to suggest further treatment alternatives, such as radioiodine ablation, prophylactic CND is advised (3).
Several authors have introduced a more limited (ipsilateral) central neck dissection, which includes the removal of prelaryngeal, pretracheal, and paratracheal LNs on the affected side only. This is because the main argument against the elective removal of central neck nodes is the risk of complications following prophylactic CND (4).
MATERIAL AND METHODS
Type of the study: Randomized Prospective study.
Required sample
50 patients divided randomly (simple randomization) into two groups (A) & (B). Each group is composed of patients who are diagnosed as papillary thyroid carcinoma and negative LNs metastasis by ultrasound. Group A underwent total thyroidectomy with bilateral central neck dissection. Group B underwent total thyroidectomy with unilateral central neck dissection.
Study settings
The study took place at Ain Shams University hospital from April 2022 till April 2024 (one year for data collection and other year for follow up) after approval of the ethical committee and obtaining an informed consent from all participants.
Inclusion criteria
Included patients were those who were primarily diagnosed with papillary thyroid carcinoma, clinically and radiologically node-negative, patients who were pathologically diagnosed with PTC, tumor size less than or equal 4 cm (T1 or T2) and without lateral neck lymph node metastasis.
Exclusion criteria
Exclusion criteria included; therapeutic central neck dissection or CND combined with the lateral neck dissection, patients with previous thyroid surgery and patients with advanced primary tumor (T3 or T4) and clinical evidence of lymph node metastasis.
All patients included in the study were subjected to clinical assessment, careful history taking, general condition assessment and local thyroid examination.
Specific preoperative investigations included; thyroid and neck ultrasound, thyroid Profile (free T3, free T4, TSH), fine needle biopsy ,plasma levels of parathyroid hormone (PTH) (reference range, 15-65 pg/ml), total calcium (reference range, 8.4–10.4 mg/dL) and indirect laryngoscope for proper assessment of any vocal cord abnormalities.
Surgical intervention
Under the guidance of a consultant surgeon, a single surgical team operated on each patient in this research. Using nearly identical surgical methods, all cases involved a total thyroidectomy. The procedure began with the patient under general anesthesia, endotracheal intubation, supine with the neck hyperextended and the table tilted 15 degrees head up. Then, a transverse incision was made, two fingerbreadths above the sternal notch, skin and platysma were incised, both upper and lower flaps were elevated, deep fascia was opened vertically in the midline, strap muscles were drawn back, the middle thyroid vein was then ligated, the superior pedicle was dissected, and the superior thyroid artery and vein were separately ligated and divided at the thyroid pole to prevent damage to the external laryngeal nerve. After the branches of the inferior thyroid artery were ligated at the capsular level, the mobilized gland was removed.
Fig. 1 shows the recurrent laryngeal nerve was located, identified, and carefully dissected throughout its whole path until it was revealed in the larynx. Also, the superior and inferior parathyroid glands were identified and preserved.
Figure 1 - Identification and preservation of recurrent laryngeal nerve and parathyroid gland during central neck dissection

Group (A) patients underwent total thyroidectomy, followed by bilateral dissection of paratracheal, pre-tracheal, and prelaryngeal nodes, which extended from the hyoid bone above, the brachiocephalic vein below, and the carotids on both sides. The dissected LNs of the central compartment were designated individually on each side. Fig. 2 shows dissection of level VI LNs of the neck.
Figure 2 - Central compartment neck dissection

In group (B), cases underwent total thyroidectomy with ipsilateral central compartment neck dissection (removal of prelaryngeal, pretracheal and paratracheal LNs on the affected side only). A suction drain was used in all patients of group A and group B. In both group harmonic scalpel was used for dissection of lateral area.
Postoperative assessment
Patients assessed postoperatively regarding:
1. Patients were followed up and assessed for hypoparathyroidism. Parathyroid hormone (PTH) levels were tested postoperatively (normal level: 15-65 pg/mL). Hypoparathyroidism (defined as a parathyroid hormone (PTH) level < 15 pg/ml permanent hypoparathyroidism if the decrease of intact parathyroid hormone persisted for > 6 months.
2. Hoarseness of voice accompanied by indirect laryngoscope to detect RLN palsy. Permanent RLN palsy was defined as vocal cord dysfunction persisting more than 6 months after the initial surgery while transient RLN palsy less than 6 months.
3. Patients followed up for chyle leakage.
4. Histopathology of central lymph nodes for patients who underwent unilateral CND and in case of bilateral CND: labelling of LNs of each side was done, to identify microscopic lymph node metastasis in each group separately.
Statistical analysis
Following collection, revision, coding, and entry, the data were loaded into IBM SPSS, a statistical package for social science, version 27. The ranges, standard deviations, and mean of the quantitative data were displayed. Quantitative variables were also shown as percentages and numbers. When the predicted count in any cell was less than 5, the Chi-square test and/or Fisher exact test were used to compare the qualitative data across the groups. The Independent t-test was used to compare two independent groups with quantitative data and a parametric distribution. The allowable margin of error was set at 5%, while the confidence interval was set at 95%. Thus, the following p-value was deemed significant:
• P-value > 0.05: Non-significant (NS);
• P-value < 0.05: Significant (S);
• P-value < 0.01: Highly significant (HS).
RESULTS
Regarding the age, sex, and medical history of the patients under study, there was no statistically significant difference between group A and group B, as indicated by the preceding table 1, where P-values varied from 0.313 to 0.889.
Table 2 shows comparison between group A (bilateral. PCND) and group B (ipsilateral PCND) regarding operative time and hospital stay among the studied patients. The results exhibit that there was no statistically significant increase in operative time and hospital stay in group A than group B with p-value = 0.226 and 0.433 respectively.
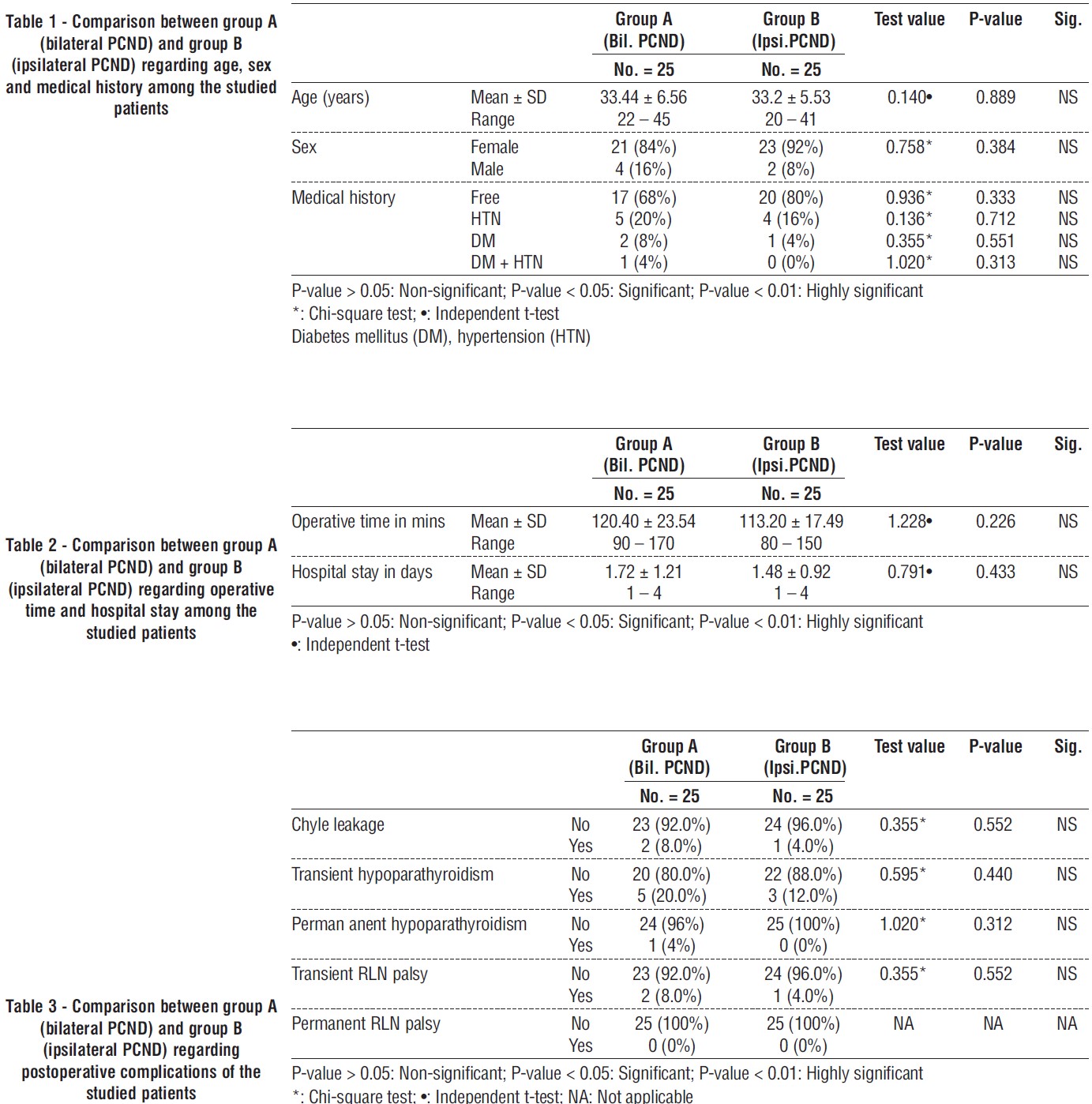
Comparison between group A (bilateral PCND) and group B (ipsilateral PCND) regarding postoperative complications of the studied patients were showed in table 3. The results exhibit that there was no statistically significant increase in chyle leak, transient hypopara-thyroidism, permanent hypoparathyroidism transient RLN palsy and permanent RLN palsy in group A than group B with p-value = 0.552, 0.440, 0.312 and 0.552 respectively.
Fig. 3 shows comparison between group A (bilateral PCND) and group B (ipsilateral PCND) regarding post-operative complications. Chyle leak occurred in 2 (8%) and 1 (4%) in group A and B, respectively. Transient hypoparathyroidism was recorded in 5 (20%) and 3 (12%) for group A and B, respectively. Regarding permanent hypoparathyroidism, the patient's percentage was 1 (4%) and zero for group A and B, respectively. With respect, transient RLN palsy, the percentage of patients were 2 (8%) and 1 (4%) for group A and B, respectively. Also, permanent RNL palsy patients were zero in both groups.
Figure 3 - Comparison between group A (bilateral PCND) and group B (ipsilateral PCND) regarding incidence of chyle leakage, transient hypoparathyroidism, permanent hypoparathyroidism, transient RLN palsy and permanent RNL palsy

The results show that the number of dissected LNs and positive LNs in pathology were statistically significant in group A than group B with P value 0.030 and 0.031, respectively.
The number of dissected lymph nodes in group A (bilateral PCND) was greater than group B (ipsilateral PCND), 9 and 7.64 LNs, respectively. The results exhibit incidence of positive LNs in pathology in patients of group A (bilateral PCND) was greater than group B (ipsilateral PCND), 44 and 16 %, respectively.
Table 5 shows relation between size of tumor and presence of positive lymph nodes in pathology among the studied patients. The result reveals that there was positive LNs in pathology in group of T2 (> 2 cm but ≤ 4 cm) more than T1 (≤ 2 cm). The difference was statically significant between group of T1 and group of T2 where P-value was 0.011. The percentage of positive lymph nodes in pathology was greater in group of T2 than group of T1, 47.8% and 14.8%, respectively.
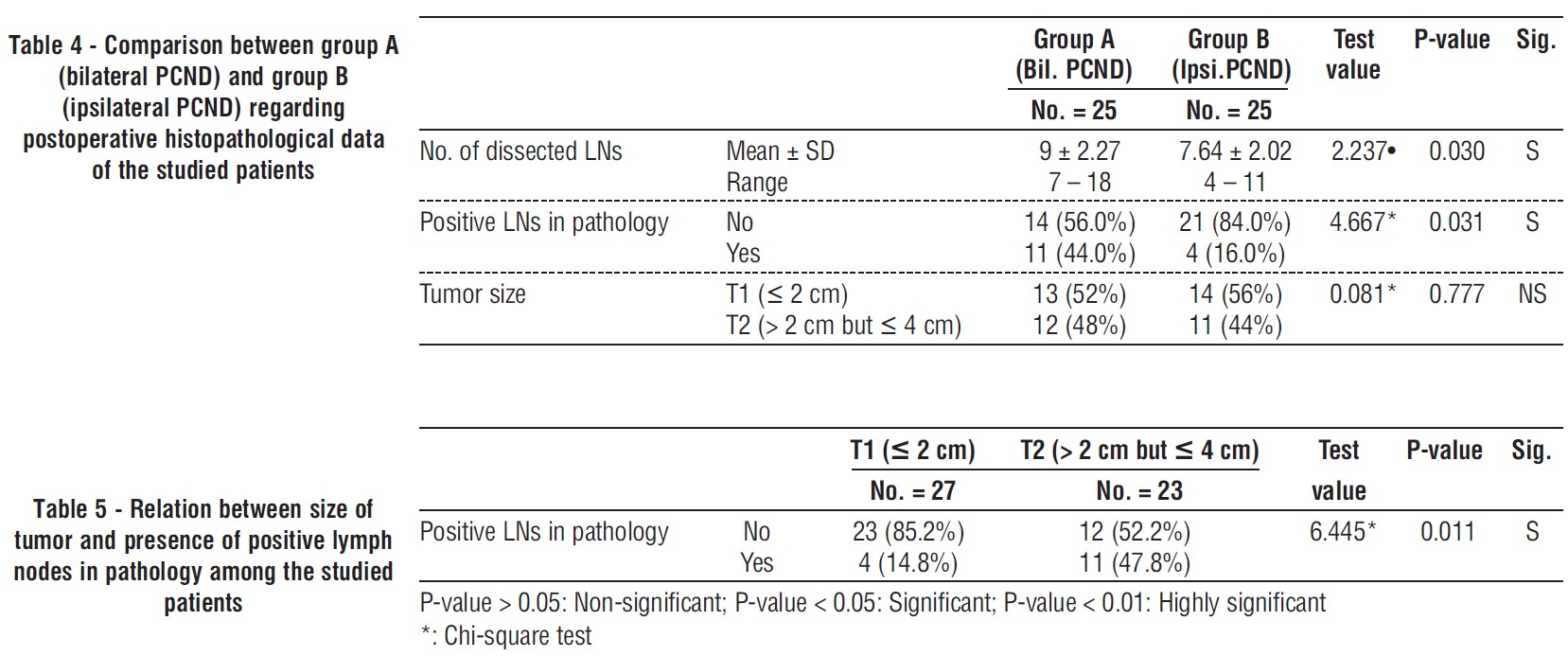
Table 6 shows relation of tumor size and presence of ipsilateral, contralateral positive LNs among group A (bilateral PCND). In group of T1, presence of ipsilateral positive LNs was more than presence contralateral positive LNs among group A (bilateral PCND), 3 and zero case, respectively. In group of T2, presence of ipsilateral positive LNs was more than presence contralateral positive LNs among group A (bilateral PCND), 8 and one case, respectively. There was statistically significant difference between group of T2 and T1, where the ipsilateral positive LNs were greater in group of T2 than group of T1, 8 and 3 cases, respectively and P-value was 0.028.
Table 6 - Relation of tumor size with presence of ipsilateral positive LNs and contralateral positive LNs among group A (bilateral PCND)
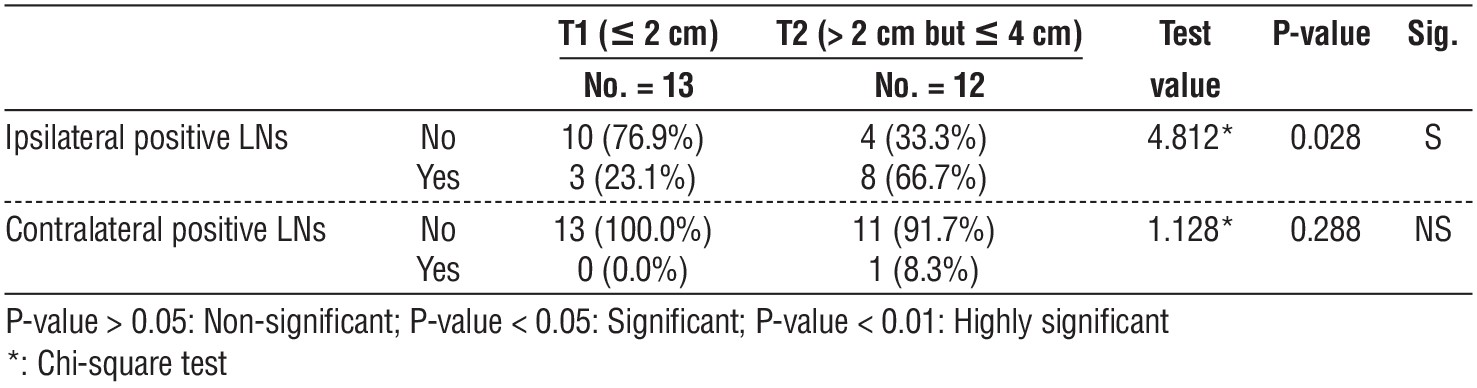
Table 7 - Presence of ipsilateral positive LNs and contralateral positive LNs among group A (bilateral PCND)
?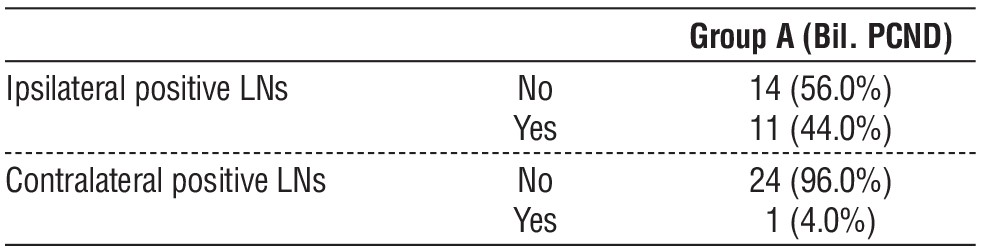
Table 7 shows presence of ipsilateral positive LNs and contralateral positive LNs among group A (bilateral PCND). The presences of ipsilateral positive LNs cases were more than contralateral positive LNs among group A (bilateral PCND), 11 and one, respectively.
The percentage of presence of ipsilateral positive LNs was more than contralateral positive LNs among group A (bilateral PCND), 44%and4%, respectively.
DISCUSSION
Approximately 80% of thyroid malignancies are papillary thyroid carcinoma. Localized PTCs have a highly favorable prognosis; almost 99% of patients survive for five years. PTC is a lymphotropic tumor, metastases to the neck nodes are a common presentation. In fact, up to 80% of cases have micrometastases, and 20-50% of individuals have involvement in the central neck compartment (5).
Management guidelines for patients with clinically apparent nodal disease are in agreement, however Prophylactic central neck dissection (PCND) in clinical nodal negative (cN0) PTC patients is still up for discussion (6).
As regard the demographic data of the current study, the average age of the patients was (33.32 ± 6.01), while in Kuo et al (7) the mean age of papillary carcinoma patients was (48.8 ± 15.7) years in a retrospective study of 1206 patients.
Also, the sex distribution in our study was 88% females and 12% males, which is close to Yildiz et al. (8) who demonstrated that thyroid cancer incidence was (17%) in males and (83%) in females in a retrospective study of 1885 patients.
Post-operative complications in this study revealed that chyle leak occurred in (6%) of all included patients, but it was higher in bilateral PCND than ipsilateral PCND, two and one case, respectively. This result was not statically significant and all patients responded to conservative management; low fat diet, orlistate and sandostatin.
According to Delaney et al. (9), the development of a Chyle leak is an uncommon but dangerous side effect of head and neck surgery, especially when a low-lying cancer is removed. It occurs in neck dissection about 2-8%.
Transient hypoparathyroidism in bilateral PCND was more than ipsilateral PCND; 5 versus 3 patients. But, it was not statistically significant. In addition, three patients had transient RLN palsy that improved on follow up after 5-6 weeks while no patients had permanent RLN palsy.
Several studies have shown that ipsilateral PCND has a lower complication rate compared to bilateral PCND and equal oncologic results, it may be sufficient for clinically node-negative PTC (10).
Ahn et al. (11) reported that all complications were transient, all patients with hypoparathyroidism had normal calcium test results within 6 months after surgery, and all patients with postoperative RLN injury had no hoarseness within 6 months after surgery.
Yoo et al. (12) found that the patients who received bilateral PCND had a higher incidence of transient hypoparathyroidism, but other than that, the complication rate was the same for both groups.
On studying data from the published literature, the majority of researches agree that ipsilateral PCND is associated with identical short-term oncologic results and a decreased risk of postoperative complications, such as temporary hypocalcemia (13).
However, the results of the current study exhibited that the number of dissected lymph nodes in bilateral PCND were greater than ipsilateral PCND, which was a statistically significant result. Additionally, postoperative pathological results, the number of positive lymph nodes was greater in bilateral PCND than ipsilateral PCND.
Similar results were obtained by Yoo et al. (12) who found that the mean number of lymph nodes removed and of metastatic lymph nodes was higher in the bilateral PCND group than the unilateral.
According to other research, routine bilateral PCND for PTC staging could enhance locoregional management and disease-free survival while lowering the risk of long-term consequences (14).
In a study conducted by Raffaelli et al. (15), 25% of the patients in this group who had bilateral PCND had bilateral central node metastases. This result is consistent with other released research that found 20-50% of cases had bilateral central node metastases. Also, they observed that one patient in the ipsilateral PCND group developed a contralateral recurrence that necessitated reoperation.
Indeed, our study revealed that T2 (> 2 cm but ≤ 4 cm) positive lymph nodes were shown to be more numerous (47.8 %) than T1 (≤ 2 cm).
The majority of studies agree that a tumor larger than 1 cm constituted a preoperative risk factor for metastases to central lymph nodes. These characteristics should be taken into account in relation to intra- or postoperatively acquired lymphovascular invasion, capsular invasion, and extrathyroidal extension (16).
A primary contention opposing PCND is the probability of post-operative complications. Despite the fact that PCND supporters have shown that, in the hands of skilled surgeons, it may be performed without additional morbidity or difficulties. Unilateral central neck dissection has become a viable alternative to bilateral central neck dissection in order to reduce the risk of PCND-related complications.Ipsilateral PCND seems to be a promising, intriguing, and safe substitute for bilateral PCND, particularly for small (stage 1) PTC (17).
According to the contralateral LNs metastasis in bilateral PCND group, there was one patient had
contralateral LNs metastasis (4%) among this group, who had tumor size > 2 cm but ≤ 4 cm (T2). And no patients had contralateral LNs metastasis in group of T1 (tumor size ≤ 2 cm).
Other authors found the similar result, rate of occult contralateral LNs metastasis was 4.2% in bilateral PCND group. They reported that there was a significant correlation between contralateral paratracheal lymph node metastasis and tumor size (> 4 cm) (12). Also, according to Lee et al. (18) 6.8% of the PTC patients had skipped metastasis to contralateral side.
Notably, though, in as many as one-fourth of the patients, ipsilateral central neck dissection may indicate a chance of missing contralateral metastases (15).
On pathologic examination, however, a significantly greater proportion of patients in the bilateral PCND group showed lymph node metastases. Finding such tiny node involvement could lead to more accurate tumor staging, even though its clinical significance is uncertain (15).
Dobrinja et al. (19) reported that PCND lowers the risk of local recurrence and increases long-term survival, improving chances of cure through improved TNM staging accuracy and more effectively RAI ablation therapy stratification Additionally, as preoperative imaging modalities are not always reliable when it comes to lymph nodes of the central compartment, PCND decreases the need for reoperation in central recurrence, which may be associated with increased morbidity.
To decrease the morbidity related to PCND, certain authors have proposed a more restricted ipsilateral central neck dissection as an alternative treatment for patients with unilateral PTC (13,15).
CONCLUSION
The present study demonstrates no statically significant difference regarding complication rate between the two groups (bilateral PCND versus ipsilateral PCND) as regard chyle leak, transient hypoparathyroidism, permanent hypoparathyroidism, transient RLN palsy and permanent RLN palsy. Moreover, prophylactic central compartment lymph node dissection detected more lymph node metastases in bilateral PCND group. Bilateral PCND seems to be the proper surgery for papillary thyroid carcinoma patients especially who have tumor size more than 2 cm, in terms of not missing any contralateral LNs and thus lowering the recurrence which require reoperation. Unilateral PCND might be appropriate for PTC patients who have tumor size less than 2 cm, given the low rate of contralateral paratracheal node metastasis.
Conflict of interest
There was no conflict of interest.
Ethical consideration
Approval was done through the ethical committeeof Ain Shams University.
REFERENCES
1. Viola D, Materazzi G, Valerio L, Molinaro E, Agate L, Faviana P, et al. Prophylactic central compartment lymph node dissection in papillary thyroid carcinoma: clinical implications derived from the first prospective randomized controlled single institution study. J Clin Endocrinol Metab. 2015;100(4):1316-24.
2. Xu S, Liu W, Zhang Z, Liu Y, Xu Z, Liu J. Routine prophylactic central neck dissection may not obviously reduce lateral neck recurrence for papillary thyroid micro carcinoma. ORL J Otorhinolaryngol Relat Spec. 2019;81(2-3):73-81.
3. Selberherr A, Riss P, Scheuba C, Niederle B. Prophylactic ‘‘First-Step’’ Central Neck Dissection (Level 6) Does Not Increase Morbidity After (Total) Thyroidectomy. Ann Surg Oncol. 2016;23(12):4016-4022.
4. Koo B, Choi E, Yoon Y, Kim D, Kim E, Lim Y. Predictive factors for ipsilateral or contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma. Ann Surg. 2009;249(5):840-4.
5. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7-34.
6. Nixon IJ, Wang LY, Ganly I, Patel SG, Morris LG, Migliacci JC, et al. Outcomes for patients with papillary cancer who do not undergo prophylactic central neck dissection. Br J Surg. 2016;103(3):218-25.
7. Kuo SF, Chao TC, Chang HY, Hsueh C, Lin CL, Chiang KC, et al. Prognosis of papillary thyroid cancers with positive serum thyroglobulin antibody after total thyroidectomy. Asian J Surg. 2017; 40(3):186-192.
8. Yildiz SY, Berkem H, Yuksel BC, Ozel H, Kendirci M, Hengirmen S. The rising trend of papillary carcinoma in thyroidectomies: 14-years of experience in a referral center of Turkey. World J Surg Oncol. 2014;12:34.
9. Delaney SW, Shi H, Shokrani A, Sinha UK. Management of chyle leak after head and neck surgery: Review of Current Treatment Strategies. Int J Otolaryngol. 2017;2017:8362874.
10. Son YI, Jeong HS, Baek CH, Chung MK, Ryu J, Chung JH, et al. Extent of prophylactic lymph node dissection in the central neck area of the patients with papillary thyroid carcinoma: comparison of limited versus comprehensive lymph node dissection in a 2-year safety study. Ann Surg Oncol. 2008;15(7):2020-6.
11. Ahn JH, Kwak JH, Yoon SG, Yi JW, Yu HW, Kwon H, et al. A prospective randomized controlled trial to assess the efficacy and safety of prophylactic central compartment lymph node dissection in papillary thyroid carcinoma. Surgery. 2022;171(1):182-189.
12. Yoo HS, Shin MC, Ji Y B, Song C M, Lee S H, Tae K. Optimal extent of prophylactic central neck dissection for papillary thyroid carcinoma: Comparison of unilateral versus bilateral central neck dissection. Asian J Surg. 2018;41(4):363-369.
13. Calo PG, Conzo G, Raffaelli M, Medas F, Gambardella C, De Crea C, et al. Total thyroidectomy alone versus ipsilateral versus bilateral prophylactic central neck dissection in clinically node-negative differentiated thyroid carcinoma. A retrospective multicenter study. Eur J Surg Oncol. 2017;43(1):126-132.
14. Barczy?ski M, Konturek A, Stopa M, Nowak W. Prophylactic central neck dissection for papillary thyroid cancer. Br J Surg. 2013; 100(3):410-8.
15. Raffaelli M, De Crea C, Sessa L, Giustacchini P, Bellantone R, Lombardi CP. Can intraoperative frozen section influence the extension of central neck dissection in cN0 papillary thyroid carcinoma? Langenbecks Arch Surg. 2013;398(3):383-8.
16. Conzo G, Tartaglia E, Avenia N, Calò PG, de Bellis A, Esposito K, et al. Role of prophylactic central compartment lymph node dissection in clinically N0 differentiated thyroid cancer patients: analysis of risk factors and review of modern trends. World J Surg Oncol. 2016; 14:149.
17. McHenry CR. Prophylactic central compartment neck dissection for papillary thyroid cancer: the search for justification continues. Surgery. 2011;150(6):1058-60.
18. Lee YS, Shin SC, Lim YS, Lee JC, Wang SG, Son SM, et al. Tumor location-dependent skip lateral cervical lymph node metastasis in papillary thyroid cancer. Head Neck. 2014;36(6):887-91.
19. Dobrinja C, Troian M, Cipolat Mis, T, Rebez G, Bernardi S, Fabris B, et al. Rationality in prophylactic central neck dissection in clinically node-negative (cN0) papillary thyroid carcinoma: Is there anything more to say? A decade experience in a single-center. Int J Surg. 2017;41 Suppl 1:S40-S47.
Full Text Sources:
Abstract:
Views: 4372

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.