Surgery, Gastroenterology and Oncology

|
|
Background: there is ongoing debate on the effectiveness of management of papillary thyroid cancer using prophylactic central lymph node dissection. In order to assess the effectiveness and safety of prophylactic central compartment lymph node removal in patients with papillary thyroid cancer, we conducted a randomized prospective study.
Material and Methods: we evaluated 40 candidates with papillary thyroid cancer with the ages between 20 and 70. In this parallel group randomized comparative study. There was no presence of lymph node or distant metastases, and the follow-up duration was between 18 and 22 months. Twenty of the forty patients who were recruited had total thyroidectomy alone (Group A), while the other twenty had total thyroidectomy together with ipsilateral central lymph node dissection as a prophylactic measure (Group B). The two groups were compared in terms of surgical completeness, postoperative complications, local recurrence, and cancer upstaging.
Results: there were four patients out of the total forty who experienced recurrence (3 in group A and 1 in group B). A statistical analysis revealed no discernible variations in the rates of locoregional recurrence (p = 0.292). Furthermore, there was no discernible difference in the occurrence of complications between the two groups. In group B, more patients were advanced to pN1.
Conclusions: in conclusion, prophylactic central neck dissection combined with total thyroidectomy in patients with papillary thyroid carcinoma who do not exhibit clinical evidence of lymph node metastases did not significantly differ in terms of surgery-related morbidity between the two groups, but it did not demonstrate any beneficial effect on the recurrence rate.
INTRODUCTION
1% of all malignancies are caused by thyroid cancer (1). Papillary thyroid carcinoma (PTC), which accounts for 80% of all thyroid malignancies, is the most prevalent type of thyroid cancer. Due to improved identification made possible by increasingly sophisticated imaging methods, its prevalence is rising quickly on a global scale (2). PTC is a slowly growing tumor with a good overall prognosis, with survival rates of 94%, 89%, and 87% at the 5-, 10-, and 20-years, respectively. Nonetheless, regional lymph node metastases are frequent, particularly in the lymph nodes located in the central compartment. Lymph node metastasis is related with greater loco regional recurrence and increased mortality and has been deemed an independent risk factor for lower survival rate (4,5).
Prior to surgery, over 35% of PTC patients had occult cervical lymph node metastases (LNM). The majority of PTC patients typically present with regional neck LNM (5). The central neck compartment is the main location where lymph nodes in PTC show metastasis (3).
Although there is a high probability of occult central nodal metastasis at the time of first surgery, it is difficult to determine in which cases these occult lymph node metastases require clearance. The percentage of clinical metastases that really affect patient outcomes is low (6).
Despite PTC's favorable prognosis, locoregional recurrence has been recorded in about 30% of patients. Poor prognosis, higher rates of morbidity and decreased survival are associated with recurrence (7).
Occult nodal metastases were seen in 50–65% of all differentiated thyroid tumors, including papillary microcarcinomas (3).
However, only around 30% of central neck (level VI) nodal involvement may be identified clinically or radiologically, making it difficult to identify lymph node metastases in the absence of pathological confirmation (8).
Patients with metastatic lymph nodes have a higher incidence of locoregional recurrence than do those without. Additionally, it is dependent on significant prognostic determinants such as the extrathyroidal extension and the extracapsular involvement of metastatic lymph nodes (7).
The anatomical position of cervical lymph nodes determines their classification (Levels I–VI). Nodes along the ipsilateral internal jugular vein (levels II, III, and IV or lateral compartment), nodes on the contralateral side, and finally ipsilateral pre- and paratracheal nodes (Level VI or central compartment) are the first nodes to develop nodal metastases from PTC. Skip metastases, despite being infrequent, can occur (9).
The American Thyroid Association statement on preoperative imaging for thyroid cancer surgery states that ultrasound is the most crucial test for assessing thyroid cancer (10).
Nevertheless, improved computed tomography and ultrasonography are not sensitive enough to detect CLNs since the latter are frequently tiny and hidden by the thyroid gland. The use of ultrasound imaging to predict CLNM in patients with PTC has been the subject of several research; nonetheless, up to 80% of false-negative results are obtained (10).
Prophylactic central-compartment lymph node dissection (PCND) is performed on patients who do not show in preoperative imaging or during operation evidence of lymph node metastases (11).
According to all standards, individuals with PTC cN1 should have a total thyroidectomy along with therapeutic cervical lymph node dissection (5). However, the decision to conduct an elective CND in the absence of ultrasound-detectable lymph node metastases is still debatable because of the lack of data about the procedure's possible risks and benefits (3,6).
The opinions of those who support and oppose central node dissection differ, which makes it a
contentious procedure that is hard to standardize. Recurrence free survival has replaced overall survival in patient care with a disease specific mortality of less than 5% (8).
According to some research, PCND decreased local recurrence rates and disease-specific survival. Others, however, showed that PCND is associated with problems rather than improving long-term outcomes. Nonetheless, a number of skilled thyroid surgeons still favor doing PCND because central lymph node metastasis is hard to identify because of low sensitivity computed tomography and ultrasonography, and occult micro metastases is very prevalent (4).
This technique aims to remove diseased lymph nodes that are clinically undetectable in order to lower the incidence of disease recurrence and enable more precise pathologic staging of the central compartment lymph nodes (12).
Proponents of PCND favor its regular application due to its advantages, which include improved TNM staging, a reduction in local recurrence, and avoiding risk of surgical morbidity following a second procedure. However, opponents of the routine use of PCND argue that more research is needed to determine the clinical effect of occult micro metastases and that doing so could overstretch the disease and increase the risk of radioactive iodine ablation without demonstrating a reduction in recurrence or an increase in benefit survival (2).
Even in skilled hands, CND carries some danger because of the higher risk of hypoparathyroidism and damage to the recurrent laryngeal nerve (RLN) (12).
Because the extent of surgery has a significant impact on the frequency of surgical problems, it is often necessary to evaluate the possible dangers and lack of benefit against this overtreatment, which lowers local recurrence and reoperation (10).
As a result, given the unwarranted morbidity linked to the operation when considering the postoperative pathologic findings, routine use of CND should be carefully considered (12).
MATERIAL AND METHODS
Study Design
Patients with non-invasive PTC and no lymph nodes detected clinically, aged 20 to 70 years were included in this prospective randomized trial from among those who attended Ain Shams University Hospitals beginning in November 2022.
Inclusion criteria
Patients undergoing total thyroidectomy for Papillary Thyroid Carcinoma, Node negative patients clinically and by ultrasound, Diagnosis of Papillary thyroid carcinoma confirmed by pathology.
Exclusion criteria
Patients undergoing revision thyroid surgery, completion thyroidectomy. Therapeutic central or lateral neck dissection due to clinically positive lymph nodes. Bilateral tumors, tumor types other than PTC, follow-up period less than 1 year, and distant metastasis.
Patients not fit for surgery, Patient refusal to participate in the study. 40 patients were included fulfilling the inclusion and exclusion criteria. Prior to their enrollment in the trial, each participant gave their informed consent. A prospective approach was taken in gathering data from medical records. Patients were randomized at random (1:1) to one of two groups in this prospective comparative randomized study: Group 1 underwent a total thyroidectomy alone, and Group 2 received a total thyroidectomy together with prophylactic CND. The closed envelope approach was used to distribute patients.
Preoperative Data
Clinical assessment
History including personal history: age, sex, medical history: diabetes, hypertension, history of irradiation, symptoms of hypothyroidism or hyperthyroidism, surgical history: History of previous operations.
Clinical examination: vital data, examination of the neck: thyroid gland, cervical lymph nodes.
Pre-operative investigations: laboratory: CBC, thyroid function tests, liver and kidney function tests, calcium level, serum thyroglobulin, vocal cord assessment by laryngoscopy. Imaging: Neck ultrasound (TIRADS scoring), CT neck in cases of retrosternal extension. Fine needle biopsy.
Intervention and Postoperative Management
Patients were divided into 2 groups, one group undergoing total thyroidectomy alone, and the other group undergoing total thyroidectomy with ipsilateral prophylactic central neck dissection.
Prelaryngeal, pretracheal, and paratracheal lymph nodes (LNs) constitute the central compartment lymph nodes (Level VI).
Surgical anatomy of the central neck compartment is composed of level VI and level VII. This is bounded superiorly by the hyoid bone, laterally by the carotid arteries, anteriorly by the superficial layer of the deep cervical fascia, and posteriorly by the pre-vertebral layer of the deep cervical fascia. The inferior border of the central compartment is defined as the brachicephalic artery. This region includes the pre-laryngeal (Delphian), pre-tracheal, paralaryngeal and para-tracheal lymph nodes. Level VII contains the anterior superior mediastinal lymph nodes found below the level of the upper border of the sternal manubrium and above the brachiocephalic artery.
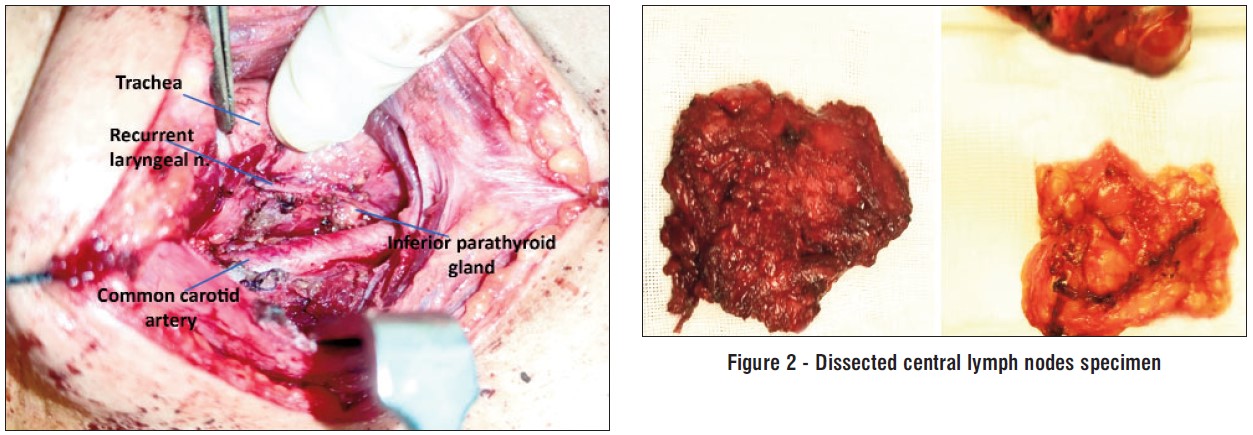
CND starts with identification of the RLN identification, dissection along its whole course in the tracheo-esophageal groove, then a lateral to medial dissection of the paratracheal lymph nodes is done. The carotid artery forms the lateral border of the dissection, with attention to potential lymph nodes posterior to the common carotid. During the dissection, the parathyroid glands are identified and preserved. When dissection of the specimen reaches medial to the RLN, it is pulled away from the trachea while the tissues are retracted upwards so that mediastinal contents are raised and removed together with the specimen.
Expert endocrine surgeons carried out each operation.
Histopathological data (tumor size, extra thyroidal extension, lymphovascular, number of recovered LN, metastasis) were evaluated when the pathologic results were confirmed.
If required, patients received treatment with radioactive iodine (RAI) ablation. Tumor size > 4 cm or any of the risk variables extrathyroidal extension, lymph node metastases, aggressive histological types, or residual disease were indications for RAI adjuvant treatment.
Figure 1 - Right central neck lymph node dissection
Follow up
After surgery, patients came to the outpatient clinic for follow-up visits two weeks, one, three, six, twelve, and eighteen months later. Clinically signs of recurrent laryngeal nerve injury (hoarseness, respiratory), signs of hypocalcemia: (paresthesia, tetany) were monitored.
Post-operative Lab. tests: serum calcium, para-thyroid hormone, and serum thyroglobulin.
Post-operative neck ultrasound, radioactive iodine scan if indicated.
Outcome Measures
The results of this study will be assessed as regards:
-
Operative data: operative time, blood loss, vascular & nerve injury.
-
Post-operative complications: bleeding, hematoma, transient or permanent vocal cord paralysis and transient or permanent hypoparathyroidism.
-
Recurrence.
The locoregional recurrence comparison served as the main goal.
Evaluation of the frequency of postoperative complications and the impact of PCND on PTC upstaging was the secondary goal. Depending on how long they persisted, postoperative problems were classified as temporary (less than six months) or permanent (six months). Tumor in the thyroidectomy bed or metastatic central or lateral cervical LN during the follow-up phase are considered recurrences.
Persistent hoarseness and vocal cord palsy seen with laryngoscopy more than six months following surgery are considered signs of permanent recurrent laryngeal nerve damage.
PTH values less than 10 pg/mL (range 10-65 pg/mL) are considered hypoparathyroidism. When low PTH levels recover to normal within six months, it is referred to as transient hypoparathyroidism; when PTH levels remain low for more than six months, it is referred to as permanent hypoparathyroidism.
Statistical Analysis
Version 27 of the Statistical Package for Social Science (IBM SPSS) was used to enter, code, and amend the data. The ranges, standard deviations, and mean of the quantitative data were displayed. Additionally, percentages and numbers were used to represent qualitative characteristics. To determine if a variable is normally distributed, use the one-sample Kolmogorov-Smirnov test.
The comparison between groups regarding qualitative data was done by using Chi-square test and/or Fisher exact test when the expected count in any cell found less than 5.
The confidence interval was set to 95% and the margin of error accepted was set to 5%. So, the p-value was considered significant as the following:
P-value > 0.05: Non-significant (NS);
P-value < 0.05: Significant (S);
P-value < 0.01: Highly significant (HS).
RESULTS
Our study enrolled 40 patients, 20 underwent total thyroidectomy (Group A) and 20 underwent total thyroidectomy and prophylactic ipsilateral central neck dissection (Group B). The demographic data were summarized in table 1.
Table 1 - Comparison between group A and group B regarding demographic data and characteristics of the studied patients
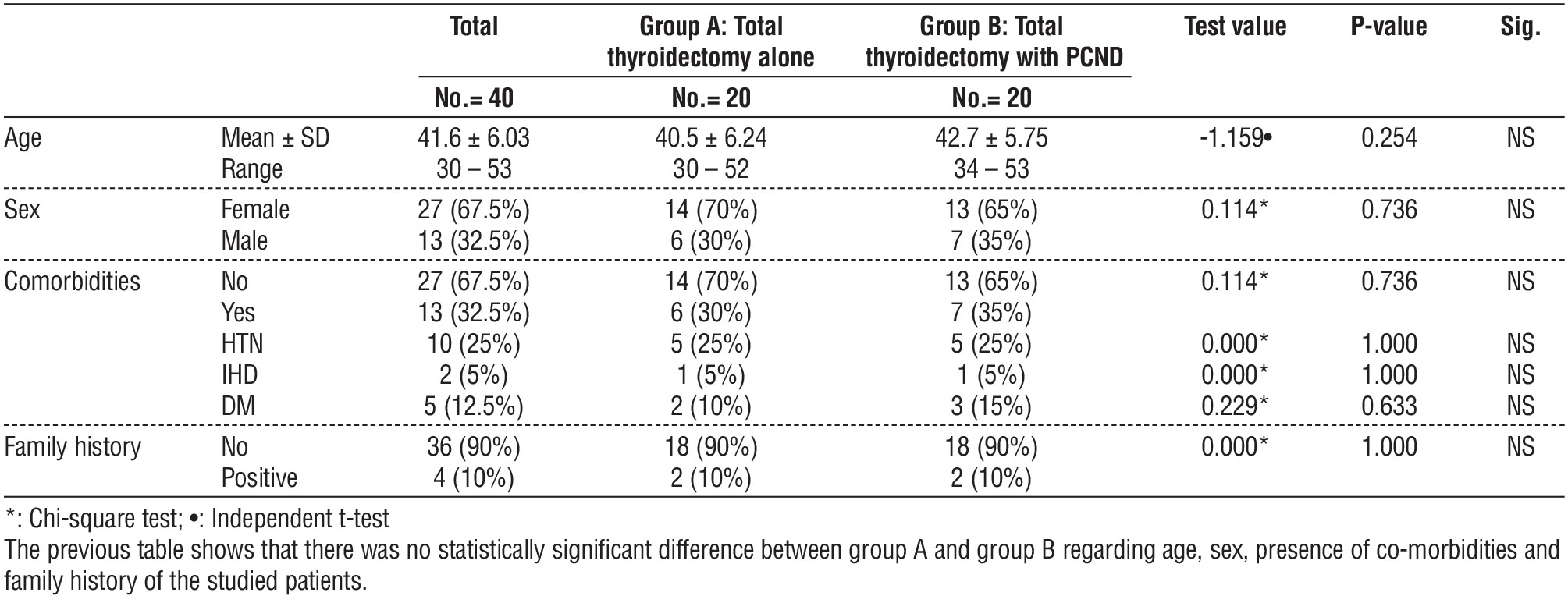
The mean age of patients in the study was 41.6 ± 6.03 years, regarding the sex the 40 patients were 27 females (67.5%) versus 13 males (32.5%).
There was no difference in age or sex between the 2 groups (p value 0.254 and 0.736 respectively) (table 1).
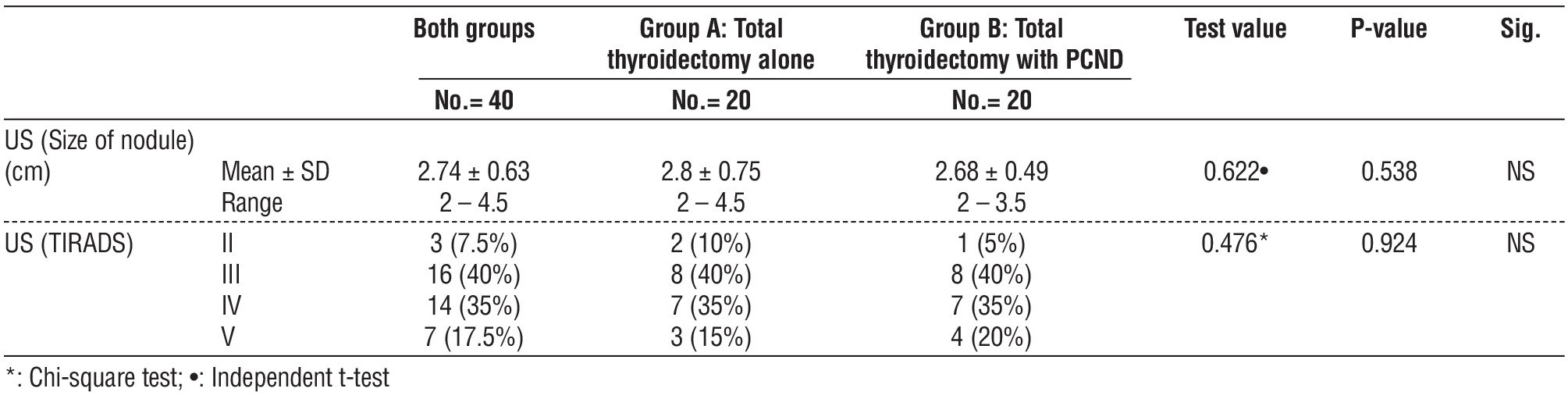
There was no significant difference between the comorbidities, family history, Ultrasound findings between the 2 groups (table 1 and 2).
Table 2 - Comparison between group A and group B regarding Ultrasound findings of the studied patients
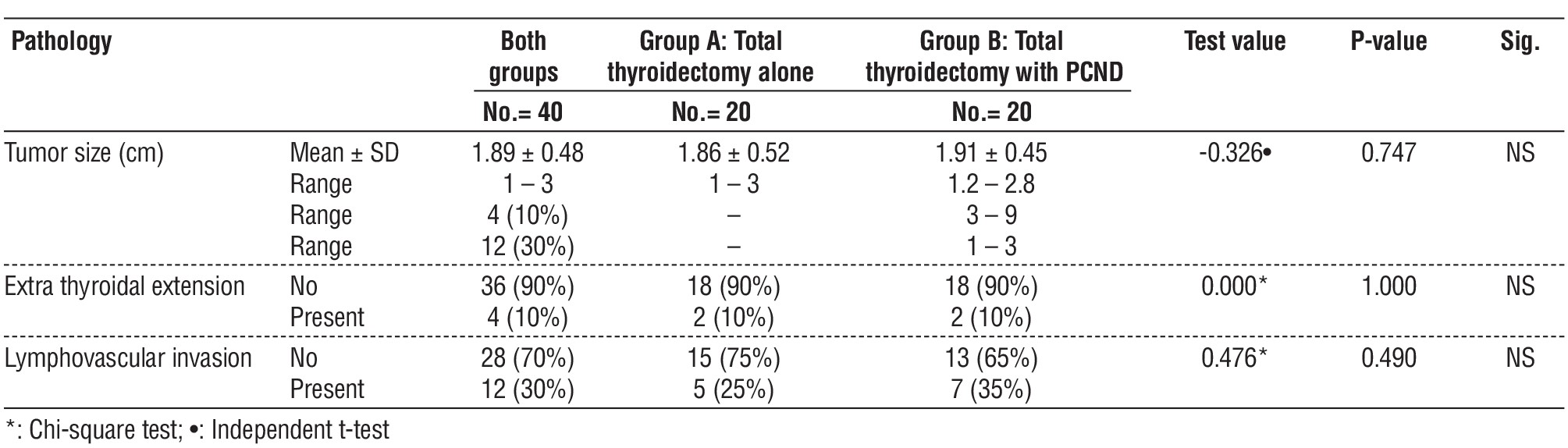
The mean tumor size in Group A 1.86 ± 0.52 versus 1.91 ± 0.45 in Group B with no significant difference (table 4).
There was no significant difference in Extrathyroidal extension and lymphovascular invasion between the 2 groups (P value 1.000 and 0.490 respectively) (table 3).
Table 3 - Comparison between group A and group B regarding the operative time of the studied patients

Table 4 - Comparison between group A and group B regarding pathological findings of the studied patients
In Group B the mean number of central lymph nodes excised is 5.6 ± 1.47 with the mean number of involved lymph nodes 2.09 ± 0.7.
The total number of patients that received post-operative radioactive iodine was 17 patients, 6 patients (30%) in group A versus 11 patients (55%) in Group B (table 5).
Table 5 - Comparison between group A and group B regarding postoperative data of the studied patients

The follow up period ranged from 18 to 22 months with mean 20.05 months in Group A and 19.8 in Group B (table 5).
The operative time was significantly longer in the second group with mean time: 136.5 ± 9.75 min. in group A and 177.75 ± 12.51 min. in group B (table 3).
The incidence of postoperative complications was more in Group B but without statistically significant difference (table 6).
Table 6 - Comparison between group A and group B regarding postoperative complications of the studied patients
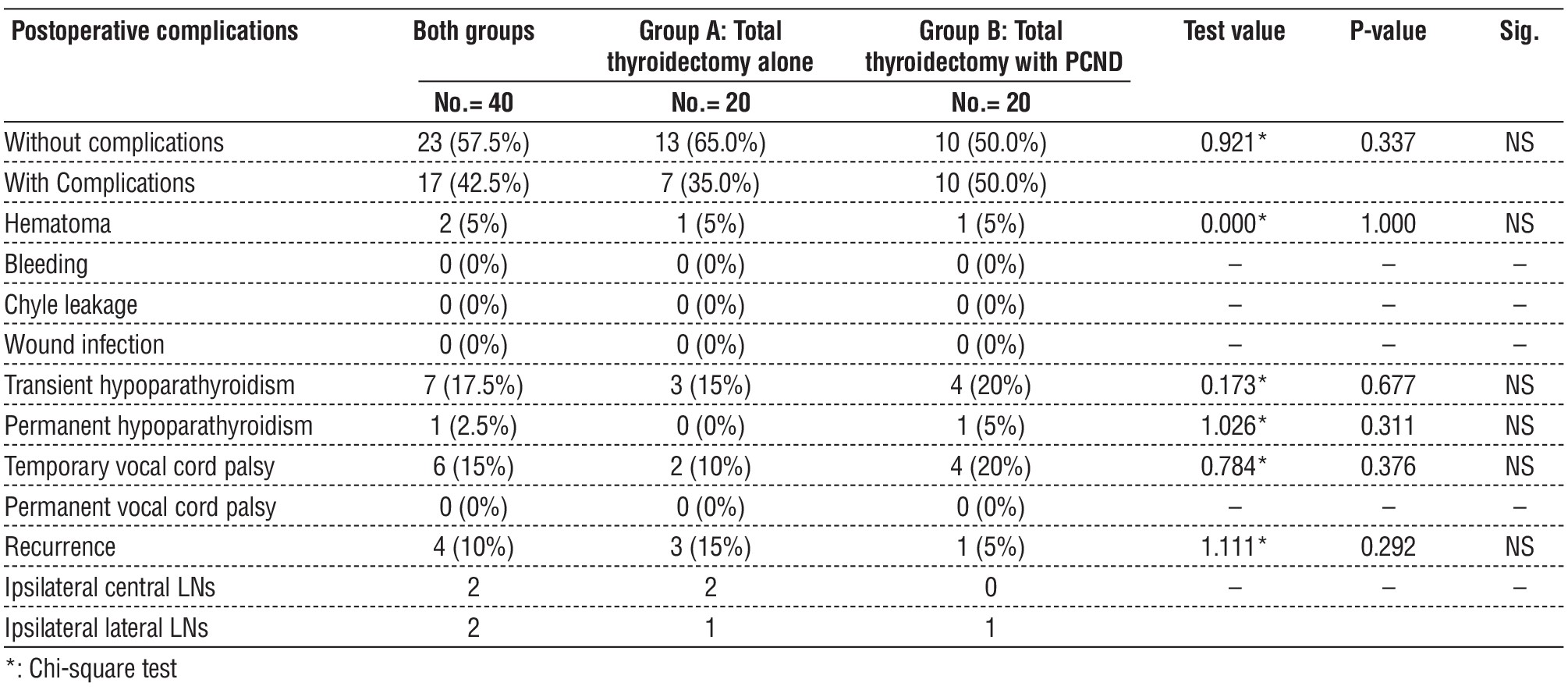
There was incidence of hematoma in 1 patient in each Group.
No incidence of bleeding or wound infection or chyle leakage. The number of patients with transient hypoparathyroidism was 3 (15%) in Group A versus 4 (20%) in Group B.
1 patient in Group B had permanent hypopara-thyroidism. Temporary vocal cord palsy occurred in 2 patients (10%) in Group A versus 4 patients (20%) in Group B. There was no incidence of permanent vocal cord palsy.
Recurrence occurred in 3 patients (15%) in Group A versus 1 patient (5%) in Group B.
Regarding the site of recurrence, in Group A the recurrence occurred in the central compartment in 2 patients and the lateral compartment in 1 patient, while in group B it occurred in the lateral compartment.
The mean tumor size in these patients with recurrence was 2.75 cm (>2 cm).
DISCUSSION
Papillary thyroid carcinoma is the most common type of thyroid cancer (5).
In papillary thyroid cancer, the occurrence of lymph node metastases is common (8). The prognosis for papillary thyroid carcinoma is good, but studies reveal that 30 to 65% of cN0 PTCs have subclinical central lymph node metastases. The ATA guidelines permit preventive CLND in high-risk cN0 patients (T3 and T4), although this procedure is still debatable because there is insufficient information available regarding the evidence of central lymph node metastases (1). Therapeutic lymph node dissection should be performed along with the procedure in patients with affected lymph nodes (N1) (5).
The best surgical approach for managing the central neck compartment in patients with papillary thyroid cancer who are clinically node negative is still controversial (12).
The oncologic advantages of prophylactic central neck dissection in cases of cN0 papillary thyroid cancer remain debatable (13).
The benefits of PCND include decreased post-operative serum thyroglobulin levels, improved staging due to its ability to identify occult lymph node metastases, and a reduction in the risk of recurrence and reoperation.
However, others are against PCND because there is insufficient data to support its effects on survival or recurrence benefit, and because it is linked to a greater rate of postoperative problems and additional expenses (4).
According to meta-analyses assessing PCND's effectiveness, it has a greater rate of postoperative complications but a reduced chance of locoregional recurrence.
However, some research has demonstrated that PCND did not lead to better long-term outcomes; rather, it exacerbated problems, indicating that PCND was not clinically significant in PTC cN0 patients (5).
Zhao et al.'s 2017 metanalysis results indicated that PCND caused a 12.1% rise in the incidence of temporary hypoparathyroidism, a 1.7% increase in the rate of permanent hypoparathyroidism, and a 1.3% increase in the rate of transient laryngeal nerve damage. Additionally, the recurrence rate decreased by almost 1%. The study found that the probability of locoregional recurrence has been considerably decreased in individuals with cN0 PTC when PCND and complete thyroidectomy were combined for therapy. However, the incidence rate of both temporary and permanent hypoparathyroidism as well as temporary recurrent laryngeal nerve injury has increased after PCND was added. However, even taking the complications following reoperation into account, assessing the risk and efficacy of PCND remains contentious.
On the other hand, the results from the 2017 study by Giordano et al. studied three groups: Group A had a total thyroidectomy alone, Group B had a total thyroidectomy plus ipsilateral CND, and Group C had a total thyroidectomy plus bilateral CND.
The rates of distant metastasis (p = 0.538) and locoregional recurrence (p = 0.890) did not differ significantly across the groups, according to statistical analysis.
The analysis of postoperative complications revealed that, without significant variations between study groups, the rate of persistent RLN damage in the study population was 0.66%, In Groups A, B, and C, it was 0.49%, 0.71%, and 0.81%, respectively. Bilateral RLN damage was not seen in any case. In the study population, the rate of persistent hypoparathyroidism was 7.38%. The rate of this complication was found in Groups A, B, and C to be 4.59%, 4.98%, and 17.74%, respectively. Group C had a substantially higher risk than Groups A and B.
According to the research Groups' results, there is no obvious benefit to elective CND in terms of loco-regional recurrence or long-term survival, notwithstanding the variations in prognostic factors. Furthermore, it raises the possibility of long-term hypoparathyroidism. Nonetheless, it provides precise lymph node staging in the center.
Ahn et al.'s prospective controlled research found that preventive central neck dissection increased the frequency of patients with lymph node metastases without increasing the risk of postoperative problems. The locoregional recurrence findings did not differ between the two groups, though (P = 0.95). Consequently, there was no therapeutic advantage from PCND for cN0 patients receiving non-invasive PTC; if a thyroidectomy is anticipated, PCND may not be necessary.
According to the results of another randomized controlled studies, surgery-related morbidity did not differ statistically between the two groups, however the use of PCND in cN0 PTC did not have any favorable influence on recurrence rate or recurrence free survival rate when compared to no PCND (13).
However, preventive central node dissection is linked to a reduction in recurrence without appreciably raising the risk of the initial operation and avoiding morbidity brought on by a second surgery, according to a prospective analysis conducted in 2020 by Mukherjee et al. However, given the increased risk of recurrent laryngeal nerve damage and hypoparathyroidism, many surgeons continue to dispute on the significance of these occult metastases and their influence on survival and risk of recurrence. As a result, not everyone agrees that prophylactic central node dissection is a beneficial approach (3).
Prophylactic central node dissection, particularly in high-risk patients with advanced primary tumors (T3 or T4), should be performed by surgeons in a tertiary care facility to reduce complications, according to 2015 ATA and Endocrine Surgery Unit guidelines. Nonetheless, there is ongoing debate over the need of doing a PCND in every case of clinically node negative PTC (cN0) (8).
Yoo et al.'s results regarding the ideal extent of PCND indicate that unilateral PCND, while less likely to cause postoperative transient hypoparathyroidism than bilateral CND, may be a suitable procedure for clinically node-negative unilateral PTC due to the relatively low rate of contralateral paratracheal node metastasis, as well as comparable serum Tg levels, recurrence rates, and disease-free survival (3).
In this randomized trial, we compared the efficacy of prophylactic ipsilateral central neck dissection—whether performed or not—with complete thyroidectomy in to demonstrate its need in patients with papillary thyroid cancer who are clinically node negative.
The demographics of the two groups in our research (age, sex, comorbidities, and family history) did not significantly differ from one another.
The preoperative ultrasound findings (nodule size and TIRADS score) did not show any statistically significant differences between the two groups.
When comparing postoperative pathology findings:
-
The mean tumour size was 1.89 ± 0.48 cm, with no significant difference between both groups.
-
The average number of lymph nodes removed from the central compartment in Group B was 5.6 ± 1.47, with a range of 3 to 9 lymph nodes. Of the 20 patients in this group, 11 individuals (or 55%) had metastatic central lymph nodes, which is in line with the proportion of occult metastasis reported in other studies. The average number of metastatic lymph nodes that were positive was 2.09 ± 0.7, with a range of 1 to 3.
There were four patients—two in each group—who had extra thyroidal extension. Five patients in group A and seven patients in group B had lymphovascular invasion, however.
Serum TG levels following thyroidectomy are well acknowledged to be an extremely sensitive and precise indicator of residual thyroid cancer or recurrence. Nonetheless, it is still debatable how pCND affects the postoperative serum TG level (13).
A total of 17 patients—11 from the second group and 6 from the first group—received post-operative radioactive iodine ablation.
When prophylactic central neck dissection was performed as opposed to a complete thyroidectomy alone, the operating time was noticeably longer.
19.9 months was the average follow-up period (with a range of 18 to 22 months).
Group B saw a higher incidence of problems in terms of postoperative morbidity and complications, although there was no statistically significant difference between the two groups.
Regarding the effect on parathyroid gland, there were 7 individuals who experienced transient hypoparathyroidism (3 in Group A, 15%) compared to 4 in Group B, 20%). One patient in Group B had permanent hypoparathyroidism.
Six individuals experienced temporary vocal cord palsy; two (10%) in Group A and four (20%) in Group B. Permanent vocal cord palsy did not occur.
Recent research has shown that tumor-induced lymphovascular invasion is a high-risk factor for both local and distant recurrence as well as central lymph node metastasis. It has been shown that individuals with lesions exhibiting capsular invasion, multifocality, and an elevated risk of lymph node metastasis, distant metastasis, and local recurrence (8).
In our analysis, there was a higher number of patients with locoregional recurrence in the first group; however, this difference was not statistically significant. Recurrence was found in 4 patients in total, 3 (15%) in Group A and 1 (5%) in Group B. One patient in Group A experienced a recurrence in the lateral compartment and two patients in the central compartment. The only recurrent occurrence in Group B occurred in the lateral compartment.
After analyzing the pathological data of these four patients, it was found that three of them had extra-thyroidal extension and that all of them had lympho-vascular invasion. These findings clearly support the concept that lymphovascular invasion and extra-thyroidal extension are significant risk factors for recurrence.
Regarding these 4 patients with recurrence there wasn’t any significant difference in age, sex, mean tumor size between both groups.
Advantages of our study include being a prospective study, done by experienced endocrine surgeons in a specialized tertiary center.
Limitations
The two main limitations of our study were the small sample size of patients and the duration of follow up ranging from 18 to 22 months. As longer follow up of patients is needed to provide a more accurate assessment of the effect of adding central lymph node dissection in papillary thyroid carcinoma on recurrence free and overall survival.
The possibility of recurrence being lower than in previous studies, because the study included mainly small, noninvasive papillary thyroid cancer patients and the short follow up period.
At last, the incidence of postoperative complications after PCND may have been underestimated in this study. As the surgeons involved were skilled experienced endocrine surgeons in a large-volume center. Further studies with larger number of patients and longer follow up period is needed.
Lacking the comparison between tumor histological differentiation and its relation to locoregional recurrence was another limitation.
CONCLUSION
The application of prophylactic central neck dissection with total thyroidectomy in papillary thyroid carcinoma without clinical evidence of lymph node metastases did not show any beneficial impact on the recurrence rate when compared to cases without dissection and the two groups did not differ significantly in terms of surgery-related morbidity and complications. Nevertheless, adding prophylactic central neck dissection led to identifying occult lymph node metastases, enabling the evaluation of the central lymph node compartment, and upstaging of the PTC patients.
Conflicts of Interest
The authors have no conflicts of interest.
Ethical Statement
This study was approved by the Ethical Committee in Ain Shams University.
REFERENCES
-
Liu J, Fan XF, Yang M, Huang LP. Analysis of the risk factors for central lymph-node metastasis of cN0 papillary thyroid micro-carcinoma: A retrospective study. Asian J Surg. 2022;45(8):1525–9.
-
Dobrinja C, Troian M, Cipolat Mis T, Rebez G, Bernardi S, Fabris B, et al. Rationality in prophylactic central neck dissection in clinically node-negative (cN0) papillary thyroid carcinoma: Is there anything more to say? A decade experience in a single-center. Int J Surg. 2017;41 Suppl 1:S40-S47.
-
Yoo HS, Shin MC, Ji YB, Song CM, Lee SH, Tae K. Optimal extent of prophylactic central neck dissection for papillary thyroid carcinoma: Comparison of unilateral versus bilateral central neck dissection. Asian J Surg. 2018;41(4):363–9.
-
Jin SH, Kim IS, Ji YB, Song CM, Chung MS, Tae K. Efficacy of prophylactic central neck dissection in hemithyroidectomy for papillary thyroid carcinoma. European Archives of Oto-Rhino-Laryngology. 2020;277(3):873–9.
-
Ahn J hyuk, Kwak JH, Yoon SG, Yi JW, Yu HW, Kwon H, et al. A prospective randomized controlled trial to assess the efficacy and safety of prophylactic central compartment lymph node dissection in papillary thyroid carcinoma. In: Surgery (United States). Elsevier Inc.; 2022. p. 182–9.
-
Gonçalves Filho J, Zafereo ME, Ahmad FI, Nixon IJ, Shaha AR, Vander Poorten V, et al. Decision making for the central compartment in differentiated thyroid cancer. Eur J Surg Oncol. 2018; 44(11):1671-1678.
-
Yoo HS, Shin MC, Ji YB, Song CM, Lee SH, Tae K. Optimal extent of prophylactic central neck dissection for papillary thyroid carcinoma: Comparison of unilateral versus bilateral central neck dissection. Asian J Surg. 2018;41(4):363–9.
-
Mukherjee D, Arnav A, Agarwal VK, Sharma R, Saidha N. Prophylactic central node dissection in differentiated thyroid cancer: a prospective tertiary care center experience. Cancer Treat Res Commun. 2020:25:100228.
-
Elaraj DM, Sturgeon C. Adequate surgery for papillary thyroid cancer. Surgeon. 2009;7(5):286–9.
-
Sun F, Zou Y, Huang L, Shi Y, Liu J, Cui G, et al. Nomogram to Assess the Risk of Central Cervical Lymph Node Metastasis in Patients With Clinical N0 Papillary Thyroid Carcinoma. Endocrine Practice. 2021; 27(12):1175–82.
-
Zhao WJ, Luo H, Zhou YM, Dai WY, Zhu JQ. Evaluating the effectiveness of prophylactic central neck dissection with total thyroidectomy for cN0 papillary thyroid carcinoma: an updated meta-analysis. Eur J Surg Oncol. 2017;43(11):1989-2000.
-
Giordano D, Frasoldati A, Gabrielli E, Pernice C, Zini M, Castellucci A, et al. Long-term outcomes of central neck dissection for cN0 papillary thyroid carcinoma. Am J Otolaryngol. 2017;38(5):576-581.
-
Kim BY, Choi N, Kim SW, Jeong HS, Chung MK, Son YI. Randomized trial of prophylactic ipsilateral central lymph node dissection in patients with clinically node negative papillary thyroid micro-carcinoma. Eur Arch Otorhinolaryngol. 2020;277(2):569-576.
Full Text Sources:
Abstract:
Views: 4430

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.