Surgery, Gastroenterology and Oncology

|
|
Introduction: Transanal total mesorectal excision (TaTME) has been used as a surgical technique for rectal cancer treatment for over a decade now. The bottom-up dissection
provides a better view of the pelvic sensory nerve fibers, which theoretically could lead to better nerve preservation, hence better functional outcomes. Nevertheless, concerns about worsening of the functional results due to low anastomosis and sphincter damage caused by the platform have been raised. There is no clear data showing advantage or disadvantage of TaTME compared to robotic total mesorectal excision (rTME) or laparoscopic TME in terms of functional results. This study aims to present single-center data on quality of life (QoL) after TaTME.
Material and Methods: A single-center prospective study on the quality of life after the first 16 consecutive cases of TaTME from July 2019 to June 2021 was conducted. Quality of life (QoL) was assessed with a questionnaire. A total of 13 patients were analyzed by EuroQol-5D (EQ-5D), EORTC QLQ-C30, EORTC QLQ-CR29, IPSS, LARS and Vaizey scores 1–9. Quality of Life data collection was done according to the following algorithm: (a) In patients without a stoma – preoperatively, at 3, 6, and 12 months, and annually thereafter; (b) in patients with a stoma – preoperatively, at 3 months postoperatively (if there was no stoma reversal), and after stoma reversal at 3, 6, and 12 months, and annually thereafter. All procedures were performed by the same team.
Results: A total of 13 patients completed the questionnaires preoperatively and at least once postoperatively. Statistically significant improvement was found in the following parameters postoperatively compared with preoperative levels: EuroQol-5D pain/discomfort (p=0.014); physical functioning (p=0.046), financial problems (p=0.025); global health in QLQ-C30 (p=0.001), degree of anxiety/depression in QLQ-CR29 (p=0.020), specific quality of life in the IPSS questionnaire (p=0.011). No statistical differences were found in: the visual analogue self-reported health scale in EuroQol-5D (p=0.114); social functioning in the QLQ-C30 (p=0.705); fecal incontinence for patients without a stoma in QLQ-CR29 (p=0.317); degree of LARS (p=0.763); Vaziey score (p=0.782).
Conclusion: quality of life after TaTME seems promising, large, well-structured trials in the scientific area are needed.
Introduction
Transanal total mesorectal excision (TaTME) has been used as a surgical technique for rectal cancer treatment for over a decade now. It was developed to overcome technical difficulties in pelvic dissection for low- and mid-rectal cancer, thus leading to a better quality specimens and oncologic results. The bottom-up dissection provides a better view of the pelvic sensory nerve fibers which theoretically could lead to better nerve preservation and better functional outcomes. Nevertheless, concerns about worsening of the functional results due to low anastomosis and sphincter damage caused by the platform have been raised.
TaTME shows promising results after the learning curve is passed (1,2). The learning curve of TaTME seems to be steeper than other techniques with around 60 cases for major complications reduction, 70 cases for operative time reduction, and 25-30 cases for anastomotic leak reduction (3,4). Data show no major difference between TaTME and robotic total mesorectal excision (rTME) (5).
A wide range of data is available on the quality of life (QoL) after TaTME. Initial studies showed worse short- and mid-term functional results, but most of the sub-sequent studies showed comparable results between the different minimally invasive TME procedures (6-9). There is no clear data that prove advantage or disadvantage of TaTME over rTME or laparoscopic TME in terms of functional results (6,10-12). This study aims to present single-center data on QoL after TaTME.
Material and method
A single-center prospective study on the quality of life after the first 16 consecutive cases of TaTME from July 2019 to June 2021 was conducted. QoL was assessed with a questionnaire. A total of 13 patients were analysed by EuroQol-5D (EQ-5D), EORTC QLQ-C30, EORTC QLQ-CR29, IPSS, LARS and Vaizey scores (13-21). Quality of Life data collection was done according to the following algorithm: (a) In patients without a stoma – preoperatively, at 3, 6, and 12 months and annually thereafter; (b) in patients with a stoma – preoperatively, at 3 months postoperatively (if there was no stoma reversal), and after stoma reversal at 3, 6, and 12 months, and annually thereafter.
All procedures were performed by the same team. The inclusion criteria were: signed informed consent for inclusion in the study, histologically proven invasive carcinoma of the middle or lower rectum, staging with endorectal ultrasound or MRI and whole-body contrast-enhanced CT, and ASA Class I – III. The exclusion criteria were: contraindications for general anesthesia, recurrent rectal cancer and emergency surgery. The ERAS protocols were followed for all patients. Mechanical bowel preparation was done on the day before surgery and preoperative antibiotic prophylaxis with II-generation Cephalosporin and Metronidazole was done i.v. 60 minutes prior to skin incision. The preoperative work-up included a complete blood count, biochemical assessment, carcino-embryonic antigen (CEA), colonoscopy, pelvic MRI and whole-body contrast-enhanced CT. TaTME was done by a two-team (Cecil) approach and single-stapled colo-rectal anastomosis with a 32 mm EEA circular stapler was performed. Patients in stage IIB or higher, received neoadjuvant treatment. The assessement for stoma formation was based on age, sex, neoadjuvant therapy, smoking habits, total serum protein and albumin levels, the distance of the anastomosis from the anal verge. Risk assessment was also performed using an anastomotic leak calculator (22). Data analysis was performed with IBM SPSS statistics 26.0 statistical software. p<0.05 (95% confidence interval) was accepted as a level of significance at which the null hypothesis is rejected. For the analysis of the change of QoL in every patient, data were compared preoperatively with the last completed questionnaire postoperatively.
Results
A total of 16 patients underwent surgery in the study period, with a mean age of 69,9 years and a mean BMI of 26.98. Most of the patients (81.25%) had undergone neoadjuvant treatment (table 1). A total of 13 patients completed the questionnaires preoperatively and at least once postoperatively (two patients filled the preoperative questionnaire and were lost to follow-up after). The median follow-up was 14 months (range 3 to 36 months). It should be noted that these patients had their surgery at the beginning of the learning curve of the team, which could also affect the functional results.
Table 1 - Patients’ characteristics and outcomes

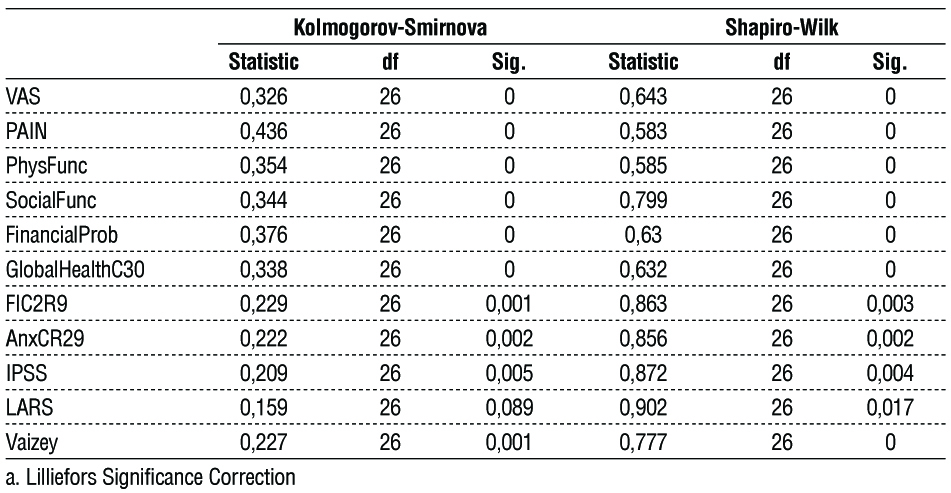
Data from the VAS on patient self-reported health and pain levels in the EuroQol-5D, physical and social functioning, financial problems and global health in the QLQ-C30, fecal incontinence and depression levels in the QLQ-CR29, IPSS score, LARS levels and Vaizey score were tested for normal distribution of the data with the Kolmogorov-Smirnov and Shapiro-Wilk tests. All data were not normally distributed (table 2). Thus, non-parametric tests for comparing the scores before and after the procedure were used - Friedman test and Kendall's W test.
When analyzing VAS data from the EuroQol-5D questionnaire the preoperative score was 64.85±10.86 (mean±SD) and the postoperative was 86.23±5.49 (mean±SD).
In the pain/discomfort section of the EuroQol-5D questionnaire, three items are possible: 1-No pain/discomfort, 2-Moderate pain/discomfort, and 3-High pain/discomfort. For the analysis, data were compared between the preoperatively completed questionnaire and the last postoperatively completed one. The mean preoperative score was 1.73 and the postoperative was 1.27.
The Physical functioning scores range from 0 (worst possible) to 100 (best possible). There are five items (questions) with three degrees of freedom. The mean preoperatively was 89.77±15.82 (mean±SD) and postoperatively 97.46±5.03 (mean±SD).
The Scores for social functioning range from 0 (worst possible) to 100 (best possible). There are two items (questions) with three degrees of freedom. The mean preoperatively was 69.38±9.05 (mean±SD) and postoperatively was 73.15±12.62 (mean±SD).
The scores for financial problems related to the treatment and the disease range from 0 (worst possible) to 100 (best possible). The item (question) is one and has three degrees of freedom. The mean preoperatively was 25.38±14.47 (mean±SD) and post-operatively was 12.69±16.71 (mean±SD).
The Global health status scores range from 0 (worst possible) to 100 (best possible). There are two items (questions) with six degrees of freedom. The mean preoperatively was 64.15±8.7 (mean±SD) and postoperatively was 82.08±8.29 (mean±SD).
The Fecal incontinence scores for patients without a stoma range from 0 (complete incontinence) to 100 (best possible continence). There are six items (questions) with four degrees of freedom. The mean preoperatively was 15.38±13.87 (mean±SD) and postoperatively was 14.08±15.73 (mean±SD).
The anxiety/depression scores range from 0 (worst possible state) to 100 (best possible state). There are two items (questions) with four degrees of freedom. The mean preoperatively was 35.85±24.33 (mean±SD) and postoperatively was 19.15±24.24 (mean±SD).
The LARS questionnaire consists of five questions with three or four degrees of freedom and gives a total score between 0 (no LARS) and 42 (major/high LARS). The division into subgroups is: 0-20 points - no LARS, 21-29 points - low LARS, 30-42 points - high LARS. The mean preoperatively was 15.46±14.08 (mean±SD) and post-operatively was 16.31±16.04 (mean±SD). Preoperatively, 7 patients were no LARS, 4 patients with minor LARS, and 2 patients with major LARS. Postoperatively, 8 patients were no LARS, 2 patients with minor LARS, and 3 patients with major LARS.
The Vaizey questionnaire contains seven questions (4 questions with five degrees of freedom and 3 questions with two degrees of freedom) and gives a total of between 0 (perfect continence) and 24 points (complete incontinence). The mean preoperatively was 2.62±3.33 (mean±SD) and postoperatively was 1.85±1.82 (mean±SD).
Table 2 - Tests of Normality
The IPSS questionnaire contains seven questions with six degrees of freedom to answer about specific symptoms and overall quality of life related to urination. The IPSS score ranges from 0 (asymptomatic) to 35 (severely symptomatic). 1-7: mild grade, 8-19: moderate grade and 20-35: severe grade. The mean preoperatively was 2.00±1.22 (mean±SD) and post-operatively 0.69±0.85 (mean±SD).
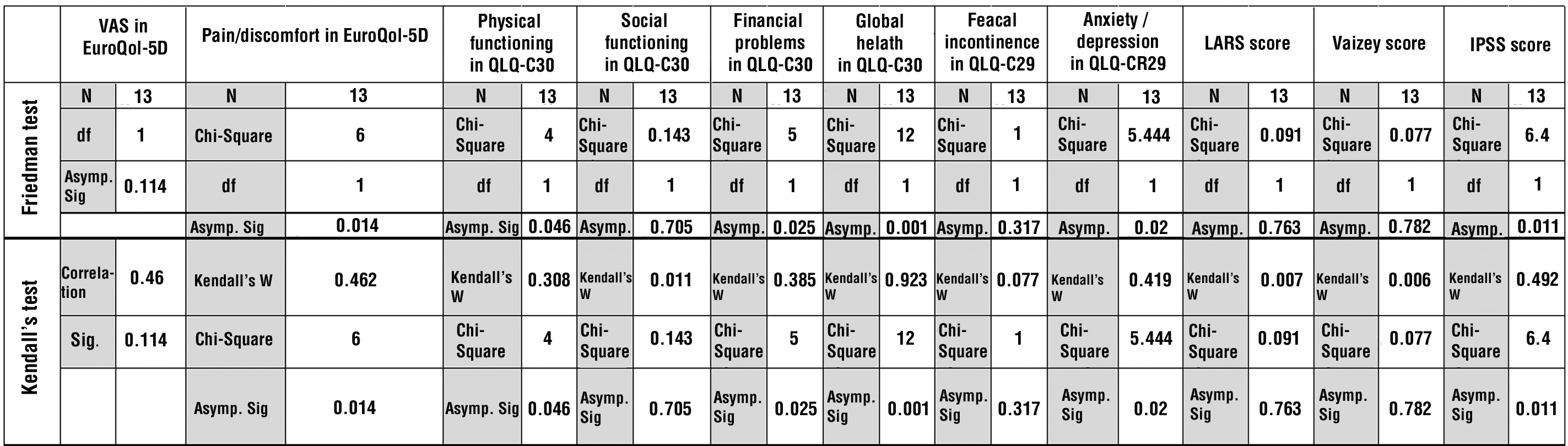
Statistically significant improvement in the following parameters postoperatively compared with preoperative levels was found: EuroQol-5D pain/discomfort (p=0.014); physical functioning (p=0.046), financial problems (p=0.025); global health in QLQ-C30 (p=0.001), degree of anxiety/depression in QLQ-CR29 (p=0.020), specific quality of life in the IPSS questionnaire (p=0.011).
No statistical differences were found in: visual analogue self-reported health scale in EuroQol-5D (p=0.114); social functioning in the QLQ-C30 (p=0.705); fecal incontinence for patients without a stoma in QLQ-CR29 (p=0.317); degree of LARS (p=0.763); Vaziey score (p=0.782)(table 3).
Table 3 - Friedman and Kendall's tests
Discussion
Quality of life after TaTME is a widely discussed and important topic as the procedure is a tool to help with difficult and low rectal tumors. These patients usually have worse QoL and higher fecal and urinary incontinence rates. Low anastomosis and sphincter trauma from the platform could lead to worse QoL. However, better nerve endings visualization and preservation could lead to better QoL and incontinence rates.
Assessment using the visual analogue scale for self-rated health within the EuroQol-5D questionnaire, showed no statistically significant differences between pre- and postoperative scores, although there was a trend towards improvement. These results are encouraging in view of the fact that no deterioration in health was observed after the surgical intervention. When analyzing the data in the pain/discomfort section of the EuroQol-5D questionnaire, a statistically significant lower level of pain/discomfort was observed in patients postoperatively (p=0.014). Pain and discomfort were associated with the quality of surgical intervention, the presence of complications in the perioperative period and recurrence-free survival. In K-related sample analysis (Friedman test and Kendall's W test) of non-parametric data of physical functioning data in QLQ-C30, there was a statistically significant improvement in patients' physical functioning post-operatively (p=0.046). In view of improving the global quality of life after surgical interventions, physical functioning is an important indicator providing clarity on patients' return to their normal lifestyle. In the same questionnaire analysis of social functioning data, they did not show statistical significance, which also means that there was no deterioration in patients' social functioning after the surgical intervention (p=0.705). In the analysis of financial problems in the QLQ-C30, the data showed a statistically significant improvement in patients' financial problems during the follow-up period. Despite a good and functioning healthcare system and free treatment for cancer patients, financial difficulties appear in a large proportion of patients during the period of active treatment. These are probably related to transportation costs, outpatient care, consumables for surgical treatment not covered by the health system, etc. Postoperative improvement in global health within the QLQ-C30 questionnaire was observed with very strong statistical significance (p=0.001). This is very promising and indicates good compliance, good awareness, patient expectations achieved, good surgical and therapeutic outcomes with low complication rates, etc. Fecal incontinence is one of the most commonly studied and important indicators related to the quality of surgery and the quality of life of patients. The analysis of fecal incontinence data for patients without a stoma within the QLQ-CR29 questionnaire showed a lack of statistical significance of pre- and postoperative outcomes. This is a positive result in this case due to the clear association between the surgical intervention and the worsening of fecal continence in patients. In TaTME, there is the advantage of visualizing and preserving the terminal nerve endings of the plexus hypogastricus inferior and plexus prostaticus. Anxiety/depression within the QLQ-CR29 questionnaire after analysis of non-parametric data (Friedman test and Kendall's W tests) showed statistically significant improvement postoperatively (p=0.020). LARS as a specific, internationally validated and widely used questionnaire for the level of fecal incontinence plays an important role in the follow-up and assessment of the quality of the surgical intervention. Pre- and postoperative data analysis showed no statistically significant difference in scoring (p=0.763), which is a positive result as no worsening of incontinence rates was observed. Vaizey questionnaire is also common for the assessment of fecal incontinence and the results also showed no statistical significance with a close p-value (p=0.782), which also indicates the stability and reliability of the data.
A lot of research has been dedicated to comparing the functional outcomes after laparoscopic TME and TaTME, with several meta-analyses showing that both procedures result in similar functional outcomes and QoL (23,24). Although TaTME was introduced to get a better view in the pelvis, initial concerns about worsening of the functional outcomes were raised (6,25). TaTME allows sphincter preservation in some patients who otherwise will undergo an abdomino-perineal excision, leading to a lower anastomosis and potential worsening of anal continence. The most commonly used tools to compare QoL were questionnaires (EORTC QoL questionnaires, International Index of Erectile Function, Female Sexual Function Index, LARS, Wexner, IPSS, and Vaizey scores), endoscopic transanal ultrasound and anorectal manometry (14,16,17,19,26,27).
An important conclusion about TaTME and any other TME techniques is that TaTME may lead to significant functional impairments so patients should receive preoperative counseling on this topic and be fully aware of the potential consequences of their treatment (28). The reported major LARS scores in these patients are 25%-33% and higher. Nevertheless, the majority of these patients had major LARS even before the procedure (26,27). Major LARS is considered one of the most important functional outcome measurements due to its great impact on the quality of life. However, stoma formation and anastomotic leak affect the QoL negatively and are connected with higher rates of major LARS. The currently available data on QoL after TaTME come mostly from small studies, with some bias, different variables, missing information and other limitations (6,11,19,25,26,29,30). More well-structured research is needed.
Conclusion
Quality of life after TaTME seems promising. Large, well-structured trials in the scientific area are needed.
Conflicts of interest and source of funding
This work was supported by the European Regional Development Fund through the Operational Programme "Science and Education for Smart Growth" under contract ?BG05M2OP001-1.002-0010-C01(2018-2023).
References
1. Keller DS, Hompes R. The learning curve in TaTME - considerations to guide safe implementation. Ann Laparosc Endosc Surg 2019;4:7.
2. Van Oostendorp SE, Eric Belgers HJ, Hol JC, Doornebosch PG, Th Belt EJ, Oosterling SJ, et al. The learning curve of transanal total mesorectal excision for rectal cancer is associated with local recurrence: results from a multicentre external audit. Color. Dis. Off. J. Assoc. Colorectal Dis. 2021;23(8):2020-2029.
3. Persiani R, Agnes A, Belia F, D’Ugo D, Biondi A, Persiani R, et al. The learning curve of TaTME for mid-low rectal cancer: a comprehensive analysis from a five-year institutional experience. Surg Endosc. 2021;35(11):6190-6200.
4. Caycedo-Marulanda A, Verschoor CP. Experience beyond the learning curve of transanal total mesorectal excision (taTME) and its effect on the incidence of anastomotic leak. Tech Coloproctol. 2020; 24(4):309-316.
5. Planellas P, Cornejo L, Pigem A, Gómez-Romeu N, Julià-Bergkvist D, Ortega N, et al. Challenges and Learning Curves in Adopting TaTME and Robotic Surgery for Rectal Cancer: A Cusum Analysis. Cancers (Basel). 2022;14(20):5089.
6. van der Heijden JAG, Koëter T, Smits LJH, Sietses C, Tuynman JB, Maaskant-Braat AJG, et al. Functional complaints and quality of life after transanal total mesorectal excision: a meta-analysis. Br J Surg. 2020;107(5):489-498.
7. Svoboda M, Procházka V, Grolich T, Kala Z. Quality of life after transanal total mesorectal excision - our experience. Rozhl Chir. 2021;100(11):534-542.
8. De Nardi P. Functional results and quality of life after transanal total mesorectal excision. Mini-invasive Surg. 2018;2:20.
9. Bjoern MX, Clausen FB, Seiersen M, Bulut O, Bech-Knudsen F, Jansen JE, et al. Quality of life and functional outcomes after transanal total mesorectal excision for rectal cancer-results from the implementation period in Denmark. Int J Colorectal Dis. 2022;37(9): 1997-2011.
10. Bloemen JG, Visschers RGJ, Truin W, Beets GL, Konsten JLM. Long-term quality of life in patients with rectal cancer: association with severe postoperative complications and presence of a stoma. Dis Colon Rectum. 2009;52(7):1251-8.
11. Koedam TWA, van Ramshorst GH, Deijen CL, Elfrink AKE, Meijerink WJHJ, Bonjer HJ, et al. Transanal total mesorectal excision (TaTME) for rectal cancer: effects on patient-reported quality of life and functional outcome. Tech Coloproctol. 2017;21(1):25-33.
12. Pucciani F. A review on functional results of sphincter-saving surgery for rectal cancer: the anterior resection syndrome. Updates Surg. 2013;65(4):257-63.
13. Balestroni G, Bertolotti G. EuroQol-5D (EQ-5D): an instrument for measuring quality of life. Monaldi Arch Chest Dis. 2012;78(3):155-9. Italian
14. Fayers P, Bottomley A. Quality of life research within the EORTC - the EORTC QLQ-C30. Eur J Cancer. 2002 Mar:38 Suppl 4:S125-33.
15. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993; 85(5):365-76.
16. van der Hout A, Neijenhuijs KI, Jansen F, van Uden-Kraan CF, Aaronson NK, Groenvold M, et al. Measuring health-related quality of life in colorectal cancer patients: systematic review of measurement properties of the EORTC QLQ-CR29. Support Care Cancer. 2019;27(7):2395-2412.
17. Stiggelbout AM, Kunneman M, Baas-Thijssen MCM, Neijenhuis PA, Loor AK, Jägers S, et al. The EORTC QLQ-CR29 quality of life questionnaire for colorectal cancer: validation of the Dutch version. Qual Life Res. 2016;25(7):1853-8.
18. Johnson TV, Abbasi A, Ehrlich SS, Kleris RS, Owen-Smith A, Raison CL, et al. IPSS quality of life question: a possible indicator of depression among patients with lower urinary tract symptoms. Can J Urol. 2012;19(1):6100-4.
19. Pape E, Pattyn P, Van Hecke A, Somers N, Van de Putte D, Ceelen W, et al. Impact of low anterior resection syndrome (LARS) on thequality of life and treatment options of LARS - A cross sectional study. Eur J Oncol Nurs. 2021;50:101878.
20. Juul T, Battersby NJ, Christensen P, Janjua AZ, Branagan G, Laurberg S, et al. Validation of the English translation of the low anterior resection syndrome score. Colorectal Dis. 2015;17(10): 908-16.
21. Vaizey CJ, Carapeti E, Cahill JA, Kamm MA. Prospective comparison of faecal incontinence grading systems. Gut. 1999;44(1):77-80.
22. Anastomotic leak calculator. http://www.anastomoticleak.com/.
23. Choy KT, Wilson Yang TW, Prabhakaran S, Heriot A, Kong JC, Warrier SK. Comparing functional outcomes between transanal total mesorectal excision (TaTME) and laparoscopic total mesorectal excision (LaTME) for rectal cancer: a systematic review and meta-analysis. Int J Colorectal Dis. 2021;36(6):1163-1174.
24. Alimova I, Chernyshov S, Nagudov M, Rybakov E. Comparison of oncological and functional outcomes and quality of life after transanal or laparoscopic total mesorectal excision for rectal cancer: a systematic review and meta-analysis. Tech Coloproctol. 2021; 25(8):901-913.
25. Veltcamp Helbach M, Koedam TWA, Knol JJ, Velthuis S, Jaap Bonjer H, Tuynman JB, et al. Quality of life after rectal cancer surgery: differences between laparoscopic and transanal total mesorectal excision. Surg Endosc. 2019;33(1):79-87.
26. Leão P, Santos C, Goulart A, Caetano AC, Sousa M, Hogemann G, et al. TaTME: analysis of the evacuatory outcomes and EUS anal sphincter. Minim Invasive Ther Allied Technol. 2019;28(6):332-337.
27. de Lacy FB, Turrado-Rodriguez V, Torroella A, van Laarhoven J, Otero-Piñeiro A, Almenara R, et al. Functional Outcomes and Quality of Life After Transanal Total Mesorectal Excision for Rectal Cancer: A Prospective Observational Study. Dis Colon Rectum. 2022;65(1):46-54.
28. van der Heijden JAG, van de Pas KGH, van den Broek FJC, van Dielen FMH, Slooter GD, Maaskant-Braat AJG. Oncological and functional outcomes of transanal total mesorectal excision in a teaching hospital in the Netherlands. Ann Coloproctol. 2022;38(1):28-35.
29. Li Y, Bai X, Niu B, Zhou J, Qiu H, Xiao Y, et al. A prospective study of health related quality of life, bowel and sexual function after TaTME and conventional laparoscopic TME for mid and low rectal cancer. Tech Coloproctol. 2021;25(4):449-459.
30. Ha RK, Park SC, Park B, Park SS, Sohn DK, Chang HJ, et al. Comparison of patient-reported quality of life and functional outcomes following laparoscopic and transanal total mesorectal excision of rectal cancer. Ann Surg Treat Res. 2021;101(1):1-12.
Full Text Sources:
Abstract:
Views: 3181

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.