Surgery, Gastroenterology and Oncology

|
|
Background: To maintain the less invasive approach to cholecysto-choledocholithiasis
treatment, other alternatives have been suggested, including single-step and two-step procedures. Aims and objectives: To assess the safety, accuracy, and effectiveness of Rendezvous techniques as a single-step treatment for cholecysto-choledocholithiasis and compare two different techniques (Dormia basket and Guide wire) regarding operative timing, safety, feasibility, failure, and complications.
Material and Methods: This research was done on 40 cases (20 cases in group A “Dormia Basket” and 20 cases in group B “Guidewire”) at the Theodor Bilharz Research Institute (TBRI), General Surgery Department, during the period from November 2021 to October 2023.
Results: There was no statistically significant variance among both groups concerning the existence of common bile duct stones (CBDS) in scans “Ultrasound (US), Magnetic Resonance Cholangiopancreatography (MRCP),” CBD diameter, the rendezvous “Laparo-endoscopic” technique stage I, intraoperative and postoperative sequale, postoperative
hospital stay, and follow-up till normalization of the liver functions or the presence of recurrent CBD stones by US, while there was statistically significant variance among both groups concerning the rendezvous “Laparo-endoscopic” technique stage II and stage III.
Conclusion: A one-stage laparo-endoscopic approach to cholecysto-choledocho-lithiasis is a safe and effective way to remove CBD stones with a small amount of time spent in the operating room, minimal risk of postoperative pancreatitis, and a quick recovery period. Our research indicates that the laparo-endoscopicrendezvous' approach utilizing a Dormia basket catheter is superior to a flexible guidewire for duodenal papilla cannulation with a statistically significant difference in operating time.
INTRODUCTION
Patients experiencing symptoms of cholelithiasis are typically treated with laparoscopic cholecystectomy (LC), a minimally invasive procedure. The introduction of LC has also altered therapeutic strategies for the management of choledocholithiasis. In order to maintain the minimally invasive approach to management, several alternatives have been suggested, such as two-step and single-step management (1).
Two-step preoperative endoscopic retrograde cholangio-pancreatography (ERCP), then LC while Single-step therapeutic approaches today vary depending on the experience of the surgeon and the availability of an ERCP or choledrochoscope. The single step includes laparoscopic CBD exploration (LCBDE) when a choledochoscope is available, ERCP and LC in the same setting, and Rendezvous technique “laparo-endoscopic” combinations of LC and ERCP (2).
It has been observed that the probability of CBD cannulation failing during ERCP might range anywhere from 4 to 18 percent, depending on the architecture of the periampullary area and the level of experience of the endoscopist (3).
LCBDE, administered by choledochotomy or the transcystic pathway, is a process that demands clinical experience with a high level of technical complexity and advanced laparoscopic skills with direct removal of the stone or by choledochoscope, then primary closure of CBD or over the T-tube with the risk of postoperative bile leakage and a long hospital stay (4).
The rendezvous "laparo-endoscopic" technique is a lifesaver throughout endoscopic procedures. It involves inserting a Dormia basket or guidewire into the duodenum through the cystic duct (CD) and CBD. This allows for elective CBD cannulation, which is especially important in cases with anatomical variations or difficult papilla cannulation through ERCP. By doing so, the surgeon avoids accidentally cannulating the pancreatic duct. Then, instead of injecting the dye retrogradely as in ERCP - which can lead to post-ERCP pancreatitis and pancreatic damage - the surgeon injects the intraoperative cholangiogram (IOC) through the CD (5).
The aim of this research was to assess the safety, accuracy, and efficiency of Rendezvous techniques as a single-step treatment for cholecysto-choledocholithiasis and compare two different techniques (Dormia basket and Guide wire) regarding operative timing, safety, feasibility, failure, and complications.
Material AND METHODS
This research was done on 40 cases (20 cases in group A “Dormia Basket” and 20 cases in group B “Guidewire”) at the TBRI, General Surgery Department, throughout the duration of November 2021 to October 2023.
Inclusion criteria
Cases with symptomatic gall bladder stones and confirmed concomitant CBD stone, calcular obstructive jaundice, presenting with biliary pain, ascending cholangitis, or acute biliary pancreatitis.
Exclusion criteria
People who are pregnant, a child, in prison, or have acute calcular cholecystitis that has been going on for more than 5 days, severe acute pancreatitis, ascending cholangitis with septic shock, CBD stones bigger than 1.5 cm in diameter and more than 3 stones in total, or who have had upper abdominal surgery before or have a reason not to have laparoscopic surgery are not eligible.
Ethical approval
The research procedure was authorized by the "Research Ethics Committee" of the TBRI and the School of Medicine at Cairo University, and each participant was asked to sign an informed consent document.
Method
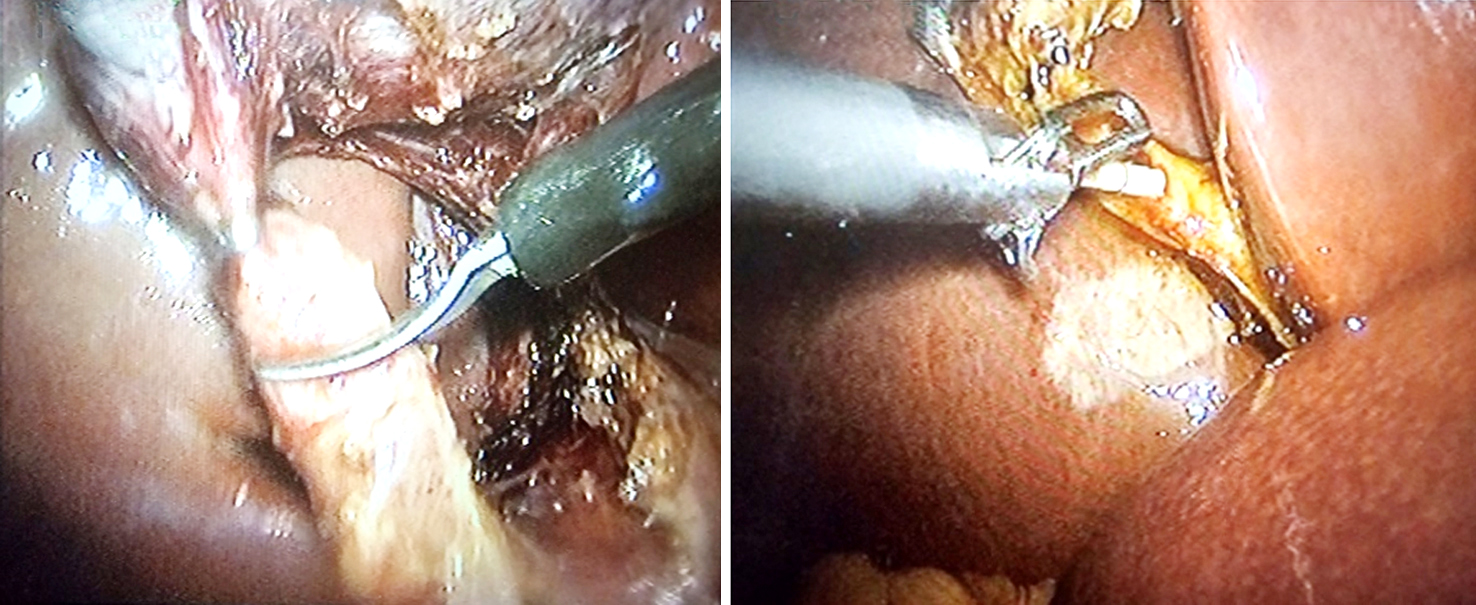
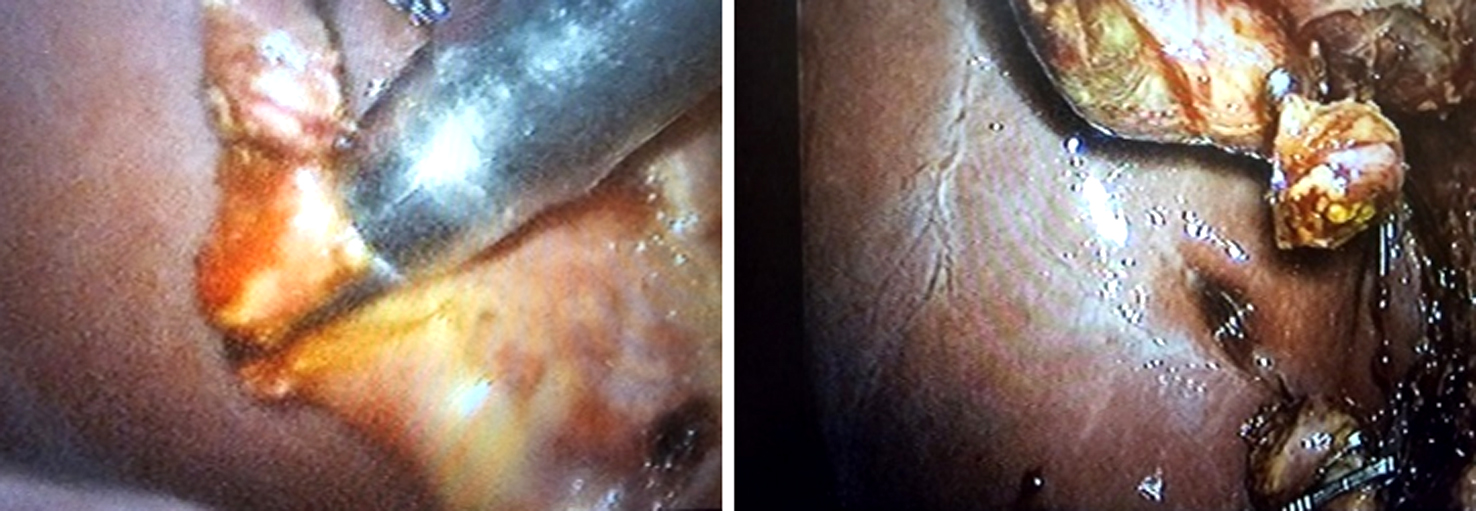
The patient was placed in a somewhat anti-Trendelenburg and supine posture with their left leg tilted to the side using four port trocars in the American way. After the cystic artery was clipped, it was first dissected and split. A tiny incision was made in the CD distal to the clip, and the gallbladder was partly removed from the liver, leaving a rim of attachment at the fundus of the gall bladder and the CD intact. The CD was clipped as high as possible. To achieve an IOC, the CD was catheterized and diluted urographin was injected. Intraoperative ERCP and endoscopic sphincterotomy (ES) were carried out when the IOC showed or verified the presence of CBDS. On the left side of the patient's head, the ERCP apparatus was positioned (fig. 1).
Figure 1 - (a) Incision in cystic duct; (b): Catheterization of CD for IOC
Group A: using a dormia basket catheter
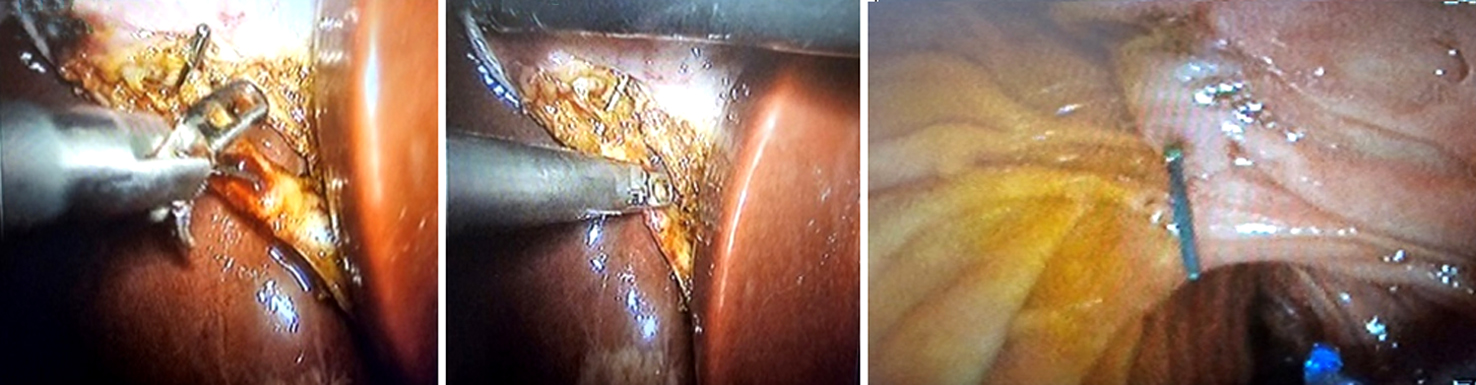
The Dormia basket catheter was inserted into the duodenum via the papilla after passing through the CD opening and into the CBD (fig. 2). While the endoscopist monitored the Dormia basket catheter's passage through the papilla, they continued to feed the endoscope to the duodenum in the same way as traditional ERCP. A sphincterotome with a guide wire attached to it was advanced under endoscopic supervision until its hydrophilic tip became lodged in the Dormia basket, which had been opened. In order to do elective CBD cannulation, the endoscopist advances the sphincterotome over the guide wire during the laparoscopic procedure. The surgeon closes the basket to capture the guide wire and pulls back the basket catheter. Now that the endoscopist had the guide wire retracted through the opened basket, the surgeon extracted the catheter from the basket and double-clipped the cyst duct at the entrance to prevent bile leakage. As with standard ERCP, the procedure began with a sphincterotomy and balloon dilatation as directed. The next step was to remove the CBD stone using a basket or balloon catheter while under fluoroscopic monitoring. To make sure the CBD is out of the system, another cholangiography per ERCP was done. After aspirating the air and fluid from the duodenum and stomach, the endoscopist removes the duodenoscope. In order to finish the cholecystectomy, the surgeon utilized clips to separate the CD.
Figure 2 - Using a dormia basket catheter in group A
(a): Dormia basket catheter passed into CBD through the opening in cystic duct;
(b): The dormia basket passes through the papilla into the duodenum;
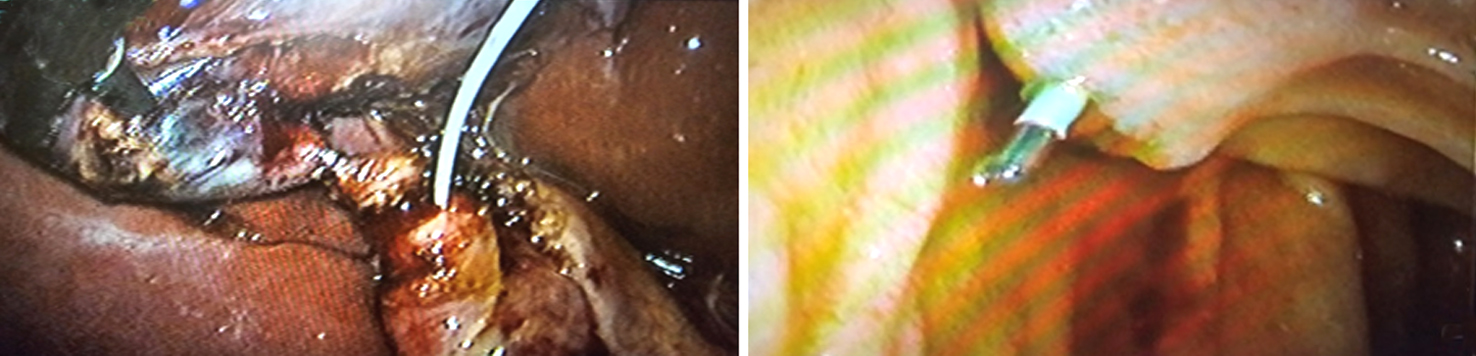
(c): A sphincterotome loaded with guide wire introduced through endoscope to approach the opened Dormia basket;
(d): Laparoscopic surgeon close the basket to grasp the guide wire into CBD;
(e): Sphincterotome is then advanced over the guide wire by the endoscopist to achieve elective CBD cannulation;
(f): surgeon open the basket and let the endoscopist retreating guide wire;
(g): double clip the cyst duct distal to the opening to avoid bile leakage during completing the process;
(h): Sphincterotomy & balloon dilatation followed by CBD stone clearance

Group B: using a guide wire (Jag-wire)
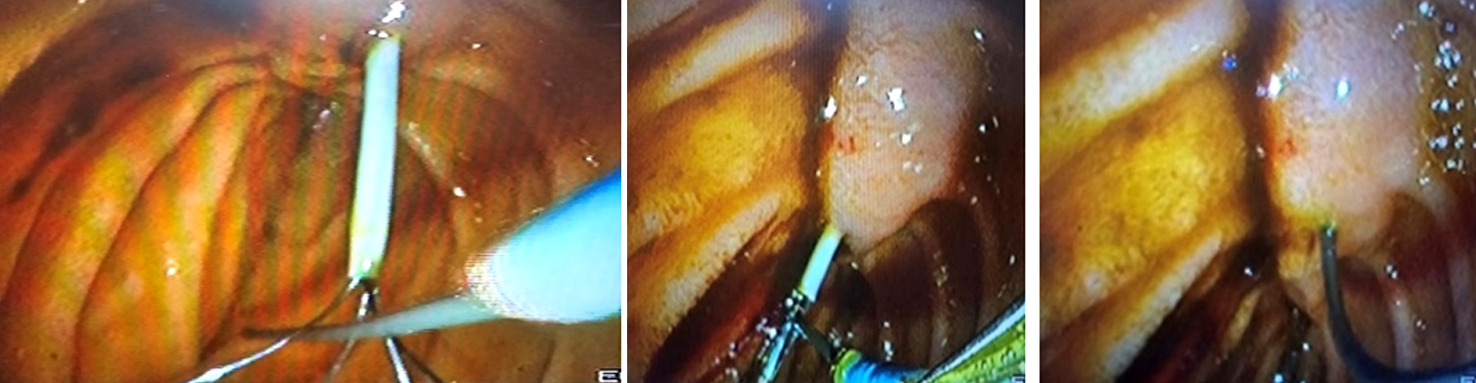
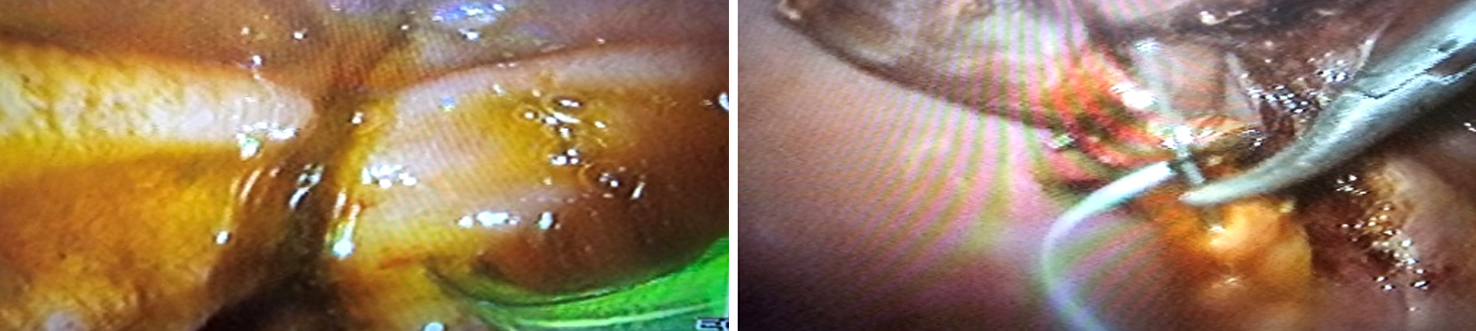
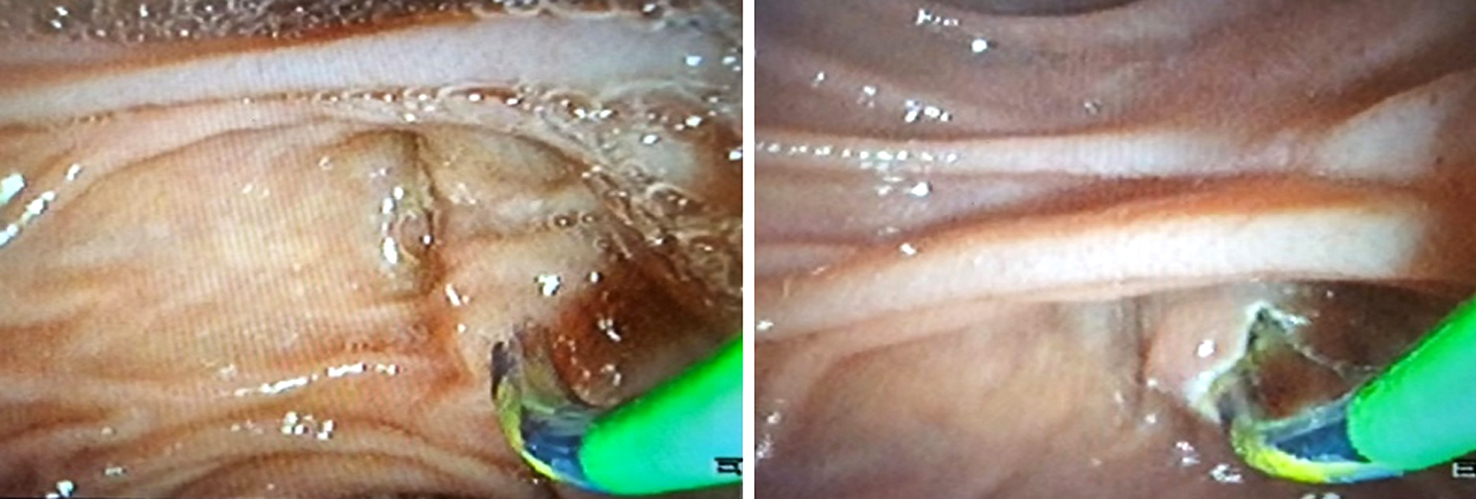
With the use of fluoroscopy, a guide wire was threaded into the duodenum via the catheter (fig. 3). After the endoscopist located the wire and secured it in a polypectomy loop, the procedure was reversed: the wire was extracted through the mouth while the scope remained in place. Afterwards, a sphincterotome was advanced through the wire to perform elective CBD cannulation. Now that the sphincterotomy is still in the distal CBD, the wire was extracted through the mouth. The CD was cut, and the cholecystectomy was finished by dividing the duct among the clips.
Figure 3 - Using a guide wire (Jag-wire) in group B
(a): A Guide Wire is advanced through the catheter into the duodenum under fluoroscopic guidance;
(b): Endoscopist inserts the endoscope in order to find the wire;
(c): The wire trapped into a polypectomy loop;
(d): The wire is pulled out through the mouth with the scope remaining in situ;
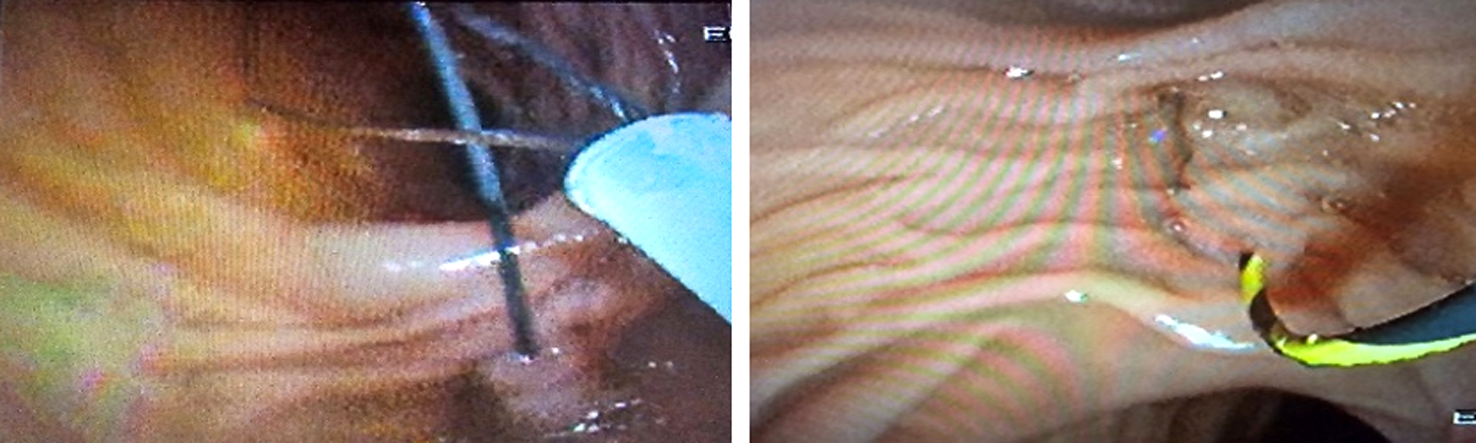
(e): A sphincterotome is advanced through the wire for elective CBD cannulation, wire is removed through the mouth while the sphincterotome remains in the distal CBD.
Follow-up
All patients underwent postoperative follow-up for liver functions (AST, ALT, total bilirubin, GGT, amylase, and lipase) until normalization and ultrasonography for the presence of recurrent CBD stones after one week, two weeks, and one month from the operation.
Statistical analysis
The data were entered into the computer, and the IBM SPSS software program version 20.0 was utilized to do the analysis. (Armonk, NY: IBM Corp.) In the description of qualitative data, both numbers and percentages were utilized. To determine whether or not the distribution was normal, the Shapiro-Wilk test was carried out. The range (minimum and maximum), mean, standard deviation, median, and interquartile range (IQR) were the statistical measures that were utilized to characterize the quantitative data. An evaluation of the significance of the data acquired was carried out at a level of 5%. The Chi-square test, Fisher's exact or Monte Carlo correction, the student t-test, and the Mann-Whitney test were the statistical operations that were carried out.
RESULTS
Table 1 showed that there was no statistical significance among both groups concerning the presence of CBD stones in Scans “US, MRCP” and CBD diameter.
Table 1 - Comparison between the two studied groups according to the presence of CBD stone in scans “US, MRCP” and CBD diameter.
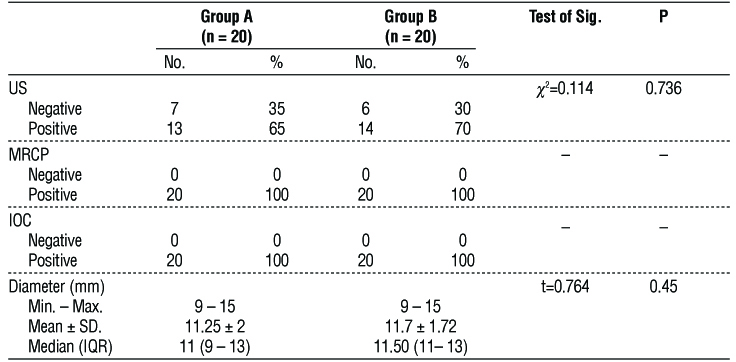
Table 2 displayed that there was no statistically significant variance among two groups concerning the rendezvous “Laparo-endoscopic” technique stage I (p=0.879), while there was statistically significant variance among both groups concerning stage II (p<0.001) and stage III (p=0.028).
Table 2 - Comparison between the two studied groups according to operative time stages.
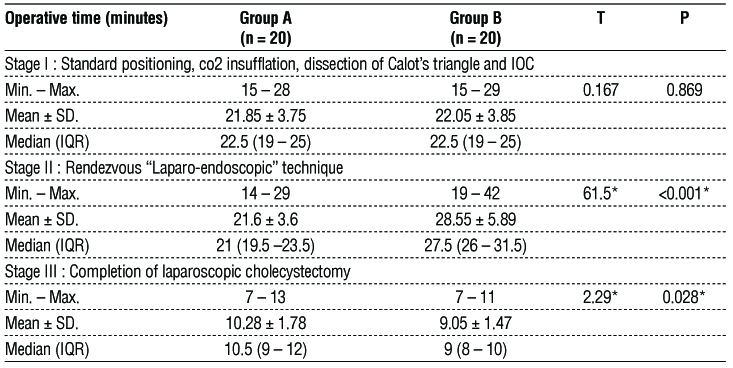
Table 3 displayed that there was no statistical significance amongst both groups concerning intra-operative and postoperative segregation.
Table 3 - Comparison between the two studied groups according to different parameters of intraoperative and postoperative segregation
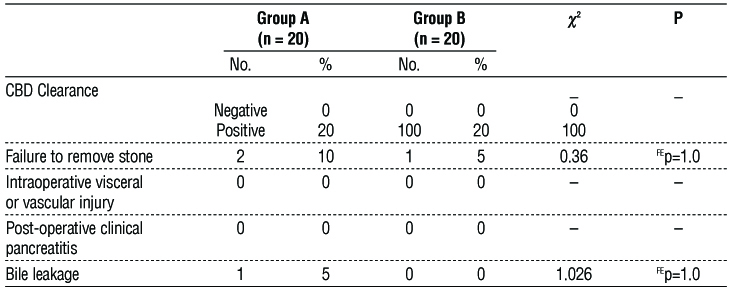
Table 4 displayed that there was no statistical signifi-cance amongst both groups concerning postoperative hospital stays.
Table 4 - Comparison between the two studied groups according to hospital stay

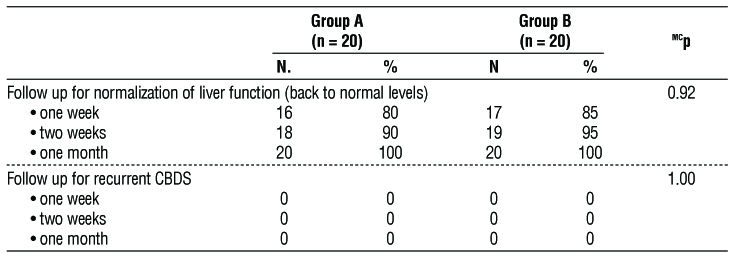
Table 5 displayed that there was no statistical significance amongst both groups concerning follow-up till normalization of the liver functions or presence of recurrent CBD stones by US.
Table 5 - Comparison between the two studied groups according to follow-up until normalization of liver functions and presence of recurrent CBD stones by US.
DISCUSSION
With advances in laparoscopy, endoscopy along with preoperative confirmation of CBD stone through MRCP, one-stage “Rendezvous” management of cholecysto-choledocholithiasis and co-ordination between laparoscopic surgeons and endoscopist has become more easier.
In our study, pre-operative US results revealed CBD stones in 65-75% of the studied cases, while intraoperative cholangiogram (IOC) and MRCP revealed CBD stones in all studied patients with a CBD diameter range of 9–15 mm, and the range size of stones was 5–14 mm. According to a recent study by Mohseni et al. among UK surgeons, the majority preferred MRCP as the primary method for likely choledocholithiasis, while the remaining percentage chose intraoperative imaging (6).
In our research, the median operative duration was 54 minutes (range of 47.5–60.5 minutes) in group A and 59 minutes (range of 53-66.5 minutes) in group B, with statistically significant variance among both groups as regard the rendezvous “Laparo-endoscopic” technique stage II: “21 minutes (range of 19.5-23.5 minutes) for Dormia basket, 27.5 minutes (range of 26-31.5 minutes) for guide wire” (p-value < 0.001). While the flexible guidewire was easier for general doctors to use and could get clogged by CBD stones, the Dormia basket catheter was better at what it was supposed to do. In a study conducted by Sherif et al., who assessed the efficacy of one-stage laparo-endoscopic “rendezvous” treatment of cholecysto-choledocholithiasis, the median operative time was 65 minutes (range of 35–120 minutes), with a stage II range of 25–55 minutes (7).
In current retrospective research from Italy done by Lagouvardou et al., the median stage II time was 15 minutes (range of 12–22 minutes) (8).
Furthermore, research conducted by Tsiopoulos et al. discovered that the median stage II time was 32 minutes (range of 15–70 minutes). These results indicated that laparoscopic rendezvous could be a viable substitute for intraoperative ERCP and reduced the endoscopic duration (9).
In our study, conversion to LCBDE was performed in 2 cases in group A and 1 case in group B due to the inability to remove stones by ERCP, with no significant variance among both groups. Unfortunately, bile leakage was noticed in one patient on postoperative day one, but the patient was managed conservatively for 14 days without further intervention.
In a study conducted by Lin et al., the intraoperative rendezvous group had lower rates of postoperative pancreatitis, morbidity, and hospitalization, according to a current meta-analysis and systematic review involving 1061 cases (519 with two-stage preoperative ERCP and subsequent LC and 542 with intraoperative rendezvous). No distinctions were observed in stone clearance, bile leakage, or conversion rate (10).
Additionally, in research conducted by Sherif et al., conversion to CBD exploration following failure of rendezvous was performed in 2.5% of cases (7).
In our research, the mean duration of postoperative hospitalization was 2.1 days (range of 1–14 days) in group A and 1.7 days (range of 1-3 days) in group B.
There was a significant improvement in success rate, reduction in hospitalization, postoperative acute
pancreatitis, and financial expense when ERCP-ES was used intraoperatively rather than postoperatively, in accordance with recent comparative research by Tan et al. and Di Lascia et al. (11,12).
In addition, a study conducted by González et al., which contrasted three various methods for CBD stone management: LC + ERCP, ERCP followed by LC throughout the same hospital admission, and LC + LCBDE, found that there were no significant variances in success rates of ductal stone clearance; nevertheless, length of hospital stays and postoperative complications were better in the first group (13).
In our study, follow-up of liver functions (AST, ALT, total bilirubin, GGT, amylase, and lipase) returned to normal levels in 80–85% of patients in both groups within one week from the operation, and all patients returned to normal levels within a month. In addition, none of the patients developed recurrent CBD stones on follow-up US up to one month from the operation.
In a study conducted by Sherif et al., they were able to reevaluate every patient at one month and 86.5% at six months; every patient had no symptoms or signs of recurring CBD stones on radiologic or laboratory evaluation, and the median time for liver function to return to normal was 2 weeks (range: 1-3 weeks) (7).
CONCLUSION
A one-stage laparo-endoscopic approach to cholecysto-choledocholithiasis is safe and effective at removing CBD stones. It avoids postoperative pancreatitis and shortens the procedure and hospital stay. Our study recommends that the laparo-endoscopic'rendezvous' technique using the Dormia basket catheter is better than flexible guidewire in duodenal papilla cannulation with a statistically significant variance in the operative time.
Acknowledgements
The authors thank the Faculty of medicine, Cairo University for providing facilities and software support for this research. Rami hassan is grateful for the infinite and selfless support from Mohammed khattab, Sami M. Said, Sobhy A. kishta, Ayman Nafeh, Ahmed M. Abdelaziz Hassan, Mohamed A. Elrefaiy and Hesham A. Elmeligy.
Conflict of interest: None.
Funding: None.
REFERENCES
1. Cianci P, Restini E. Management of cholelithiasis with choledocholithiasis: Endoscopic and surgical approaches. World J Gastroenterol. 2021;27(28):4536-4554.
2. La Barba G, Gardini A, Cavargini E, Casadei A, Morgagni P, Bazzocchi F, et al. Laparoendoscopic rendezvous in the treatment of cholecysto-choledocholitiasis: a single series of 200 patients. Surg Endosc. 2018;32(9):3868-3873.
3. Berry R, Han JY, Tabibian JH. Difficult biliary cannulation: Historical perspective, practical updates, and guide for the endoscopist. World J Gastrointest Endosc. 2019;11(1):5-21.
4. Lyu Y, Cheng Y, Li T, Cheng B, Jin X. Laparoscopic common bile duct exploration plus cholecystectomy versus endoscopic retrograde cholangiopancreatography plus laparoscopic cholecystectomy for cholecystocholedocholithiasis: a meta-analysis. Surg Endosc. 2019; 33(10):3275-3286.
5. Qian Y, Xie J, Jiang P, Yin Y, Sun Q. Laparoendoscopic rendezvous versus ERCP followed by laparoscopic cholecystectomy for the management of cholecysto-choledocholithiasis: a retrospectively cohort study. Surg Endosc. 2020;34(6):2483-2489.
6. Mohseni S, Bass GA, Forssten MP, Casas IM, Martin M, Davis KA, et al. Common bile duct stones management: A network meta-analysis. J Trauma Acute Care Surg. 2022;93(5):e155-e165.
7. Sherif AS, Hamdy SA, Al-Shareef M. One-Stage Laparo-Endoscopic Treatment of Cholecysto-Choledocholithiasis. The Medical Journal of Cairo University. 2020;88(March):833-9.
8. Lagouvardou E, Martines G, Tomasicchio G, Laforgia R, Pezzolla A, Caputi Iambrenghi O. Laparo-endoscopic management of chole-choledocholithiasis: Rendezvous or intraoperative ERCP? A single tertiary care center experience. Front Surg. 2022;9:938962.
9. Tsiopoulos F, Kapsoritakis A, Psychos A, Manolakis A, Oikonomou K, Tzovaras G, et al. Laparoendoscopic rendezvous may be an effective alternative to a failed preoperative endoscopic retrograde cholangiopancreatography in patients with cholecystocholedocholithiasis. Ann Gastroenterol. 2018;31(1):102-108.
10. Lin Y, Su Y, Yan J, Li X. Laparoendoscopic rendezvous versus ERCP followed by laparoscopic cholecystectomy in the management of cholecystocholedocholithiasis: a systemic review and meta-analysis. Surg Endosc. 2020;34(9):4214-4224.
11. Di Lascia A, Tartaglia N, Pavone G, Pacilli M, Ambrosi A, Buccino RV, et al. One-step versus two-step procedure for management procedures for management of concurrent gallbladder and common bile duct stones. Outcomes and cost analysis. Ann Ital Chir. 2021:92:260-267.
12. Tan C, Ocampo O, Ong R, Tan KS. Comparison of one stage laparoscopic cholecystectomy combined with intra-operative endoscopic sphincterotomy versus two-stage pre-operative endoscopic sphincterotomy followed by laparoscopic cholecystectomy for the management of pre-operatively diagnosed patients with common bile duct stones: a meta-analysis. Surg Endosc. 2018; 32(2):770-778.
13. González JE, Peña RT, Torres JR, Alfonso MÁ, Quintanilla RB, Pérez MM. Endoscopic versus laparoscopic treatment for choledocho-lithiasis: a prospective randomized controlled trial. Endosc Int Open. 2016;4(11):E1188-E1193.
Full Text Sources:
Abstract:
Views: 6181

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.