Surgery, Gastroenterology and Oncology

|
|
Materials and methods:This retrospective, non-randomized study analyzed 254 patients who underwent concomitant CABG and MV surgery for moderate-to-severe IMR between January 2013 and December 2018. Patients were divided into two groups: MVRp (n=128) and MVR (n=126). Perioperative characteristics, postoperative outcomes, and long-term survival were assessed.
Results: Baseline characteristics were comparable between groups, except for a higher
incidence of preoperative atrial fibrillation in the replacement group (11.9% vs. 4.7%, P=0.037). ICU stay was shorter in the replacement group (73.48±63.8 vs. 84.6±59.59 hours, P=0.048), but mechanical ventilation duration was longer (20.5±45.46 vs. 18.55±20.1 hours, P=0.016). In-hospital mortality was similar (MVRp: 11.7% vs. MVR: 12.7%, P=0.812). Long-term mortality was 21.1% in the MVRp group and 17.5% in the MVR group. Both groups showed significant improvements in ejection fraction (MVRp: 47.67±13.00% to 57.28±13.34%, P=0.001; MVR: 47.28±12.01% to 56.50±12.27%, P=0.001) and NYHA class postoperatively.
Conclusion: Both MVRp and MVR significantly improved functional status and ejection
fraction, with no significant difference in long-term survival. MVRp remains susceptible to recurrent regurgitation, while MVR eliminates MR but prolongs ventilation time. Surgical choice should be tailored to patient-specific factors.
Introduction
Although treating options and surgical modalities for treating ischemic heart disease are present nowadays with more clear techniques, the resultant mitral disease shows controversial options for treatment. Uncorrected ischemic mitral regurge (IMR) mortality is high, with 35% of patients alive at 5y with severe MR, 44% alive with moderate MR, and 61% alive without MR (1,2).
In chronic secondary MR, the MV leaflets and chordae tendineae typically remain structurally intact or exhibit only mild thickening. However, the condition is primarily linked to significant LV dysfunction secondary to coronary artery disease, leading to ischemic chronic secondary MR. LV dilation and remodeling result in papillary muscle displacement, which in turn causes leaflet tethering and annular dilation, ultimately impairing proper leaflet coaptation (3). Furthermore, secondary MR may also arise due to left atrial enlargement and mitral annular dilation, frequently observed in patients with atrial fibrillation and various cardiomyopathies. It is important to note that both primary and secondary MR can coexist within the same individual. Given that MR is merely one facet of the broader pathophysiological process, its correction alone does not resolve the underlying ventricular pathology. Despite ongoing discussions regarding the precise criteria for defining severe secondary MR, its complex nature and multifactorial origins remain evident (4,5).
When replacing or repairing the MV, continuous ventricular overload is stopped and thus pathological remodeling, which ultimately results in better elliptical geometry (6).
The aim of this work is to compare the short- and long-term outcomes of MVRp versus MVR in patients undergoing concomitant CABG for moderate-to-severe IMR.
Materials and methods
This retrospective, non-randomized study analyzed data from 254 patients who underwent CABG and MV surgery for IMR between January 2013 and December 2018. This study was conducted after being approved by the research ethics committee, Faculty of Medicine, Cairo University.
Inclusion Criteria
Patients with moderate to severe ischemic MR, confirmed by preoperative transthoracic echocardiography and coronary angiography, were included.
Exclusion Criteria
This encompassed patients with papillary muscle rupture, cardiogenic shock, ischemic ventricular septal defect, associated left ventricular aneurysm, prior CABG or valvular surgery, and non-ischemic MR disease.
Patients Groups
Patients were divided into two groups: Group A (n=128) underwent MVRp, while Group B (n=126) underwent MVR.
Methods
Preoperative Assessment
All patients underwent comprehensive history-taking, physical examination, laboratory investigations (CBC, liver and kidney function tests, serum electrolytes, and coagulation profile), and imaging studies, including chest X-ray, 12-lead ECG, echocardiography, and coronary angiography. Carotid duplex ultrasound was performed in selected patients at risk of cerebrovascular disease.
Surgical Technique
All patients underwent standard median sterno-tomy and cardiopulmonary bypass with bicaval cannulation. Cardioplegia was administered antegrade with systemic hypothermia. CABG was performed before MV intervention. Repair involved annular ring annuloplasty, edge-to-edge repair, or chordal transfer, while valve replacement was performed when repair was deemed unfeasible. Prosthetic valves were implanted using pledgetted sutures, preserving as much of the sub-valvular apparatus as possible.
Intraoperative and Postoperative Monitoring
Intraoperative parameters recorded included ischemic time, total bypass time, inotropic support requirements, and MV competence via transesophageal echocardiography (TEE). Postoperatively, patients were monitored in the ICU for hemodynamic stability, ventilatory support, blood loss, and complications such as re-exploration for bleeding, stroke, renal impairment, and infection. Total ICU and hospital stay durations were recorded.
Follow-up and Outcomes
Early postoperative assessment included echo-cardiography before discharge to evaluate MV function and cardiac contractility. Late follow-up focused on survival, NYHA functional class, echocardiographic findings, and event-free survival.
Statistical Analysis
The results were presented as mean ± standard deviation for normally distributed continuous variables, median (minimum-maximum) for non-normally distributed variables, and frequency with percentage for categorical data. Categorical variables were compared using the Chi-square test. The Kolmogorov-Smirnov test was applied to assess the normality of data distribution. For normally distributed continuous variables, comparisons between the two groups were performed using the unpaired t-test, whereas the Mann-Whitney U test was used for non-normally distributed variables. Statistical analyses were conducted using SPSS software (version 19, Windows). A P-value of <0.05 was considered statistically significant.
Results
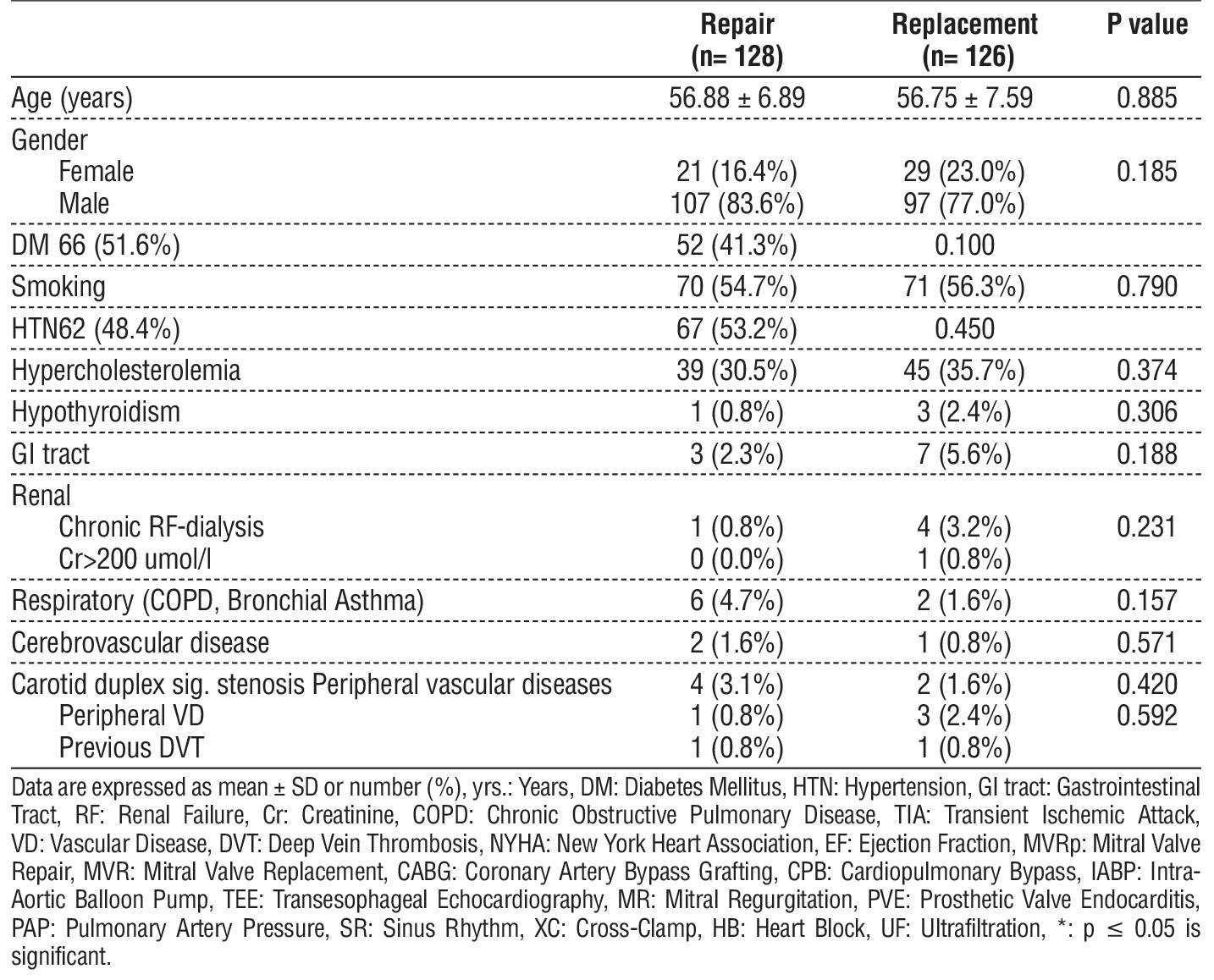
There were no statistically significant differences between the two groups regarding age and gender. Similarly, preoperative comorbidities, including diabetes mellitus, smoking, hypertension, hyper-cholesterolemia, hypothyroidism, gastrointestinal issues, renal impairment, respiratory diseases (COPD, bronchial asthma), cerebrovascular accidents (stroke, TIA), and peripheral vascular diseases, showed no significant differences between the groups (table 1).
Table 1 - General characteristics of the two studied groups
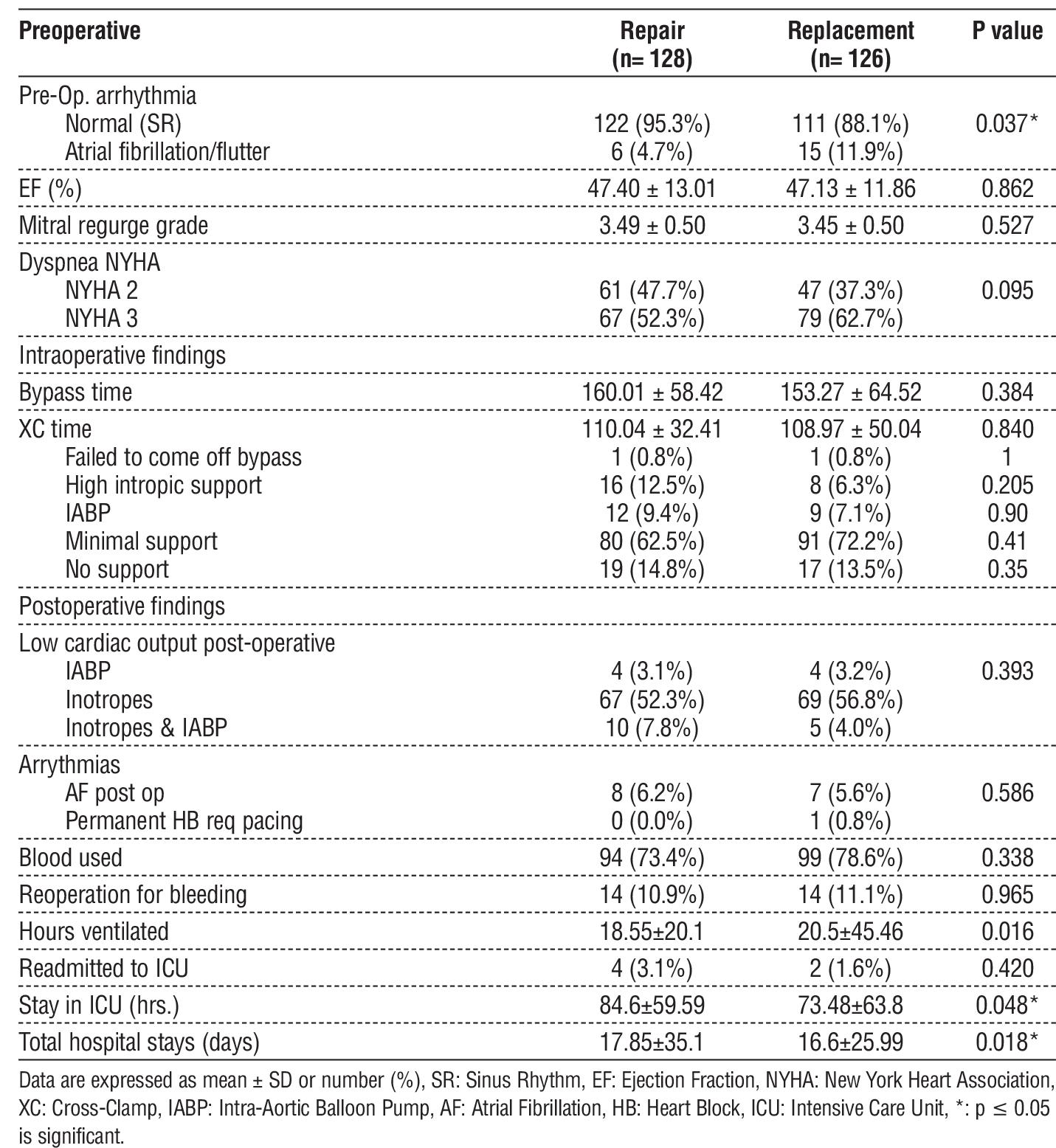
As regard the pre-operative arrhythmia the AF was significantly higher in the replacement group (p=0.037). Both groups showed no significant differences in ejection fraction, mitral regurgitation grade, NYHA classification, ischemic time, CPB time, or coming off bypass. All repair patients underwent annuloplasty (ring size 26–32, most commonly 28), while all replacement patients received mechanical valves (size 27-33) with efforts to preserve at least one leaflet. Intraoperative TEE led to 21 patients converting from repair to replacement. Mechanical ventilation duration was significantly longer in the replacement group (p=0.016), while ICU stay was significantly shorter (p=0.048). Other postoperative parameters, including low cardiac output, arrhythmias, reoperations, blood transfusions, and total hospital stay, showed no significant differences. Six patients required ICU readmission: two in the repair group (for atrial fibrillation and heart failure) and four in the replacement group (for myocardial infarction and arrhythmias) (table 2).
Table 2 - Operative findings in the two studied groups
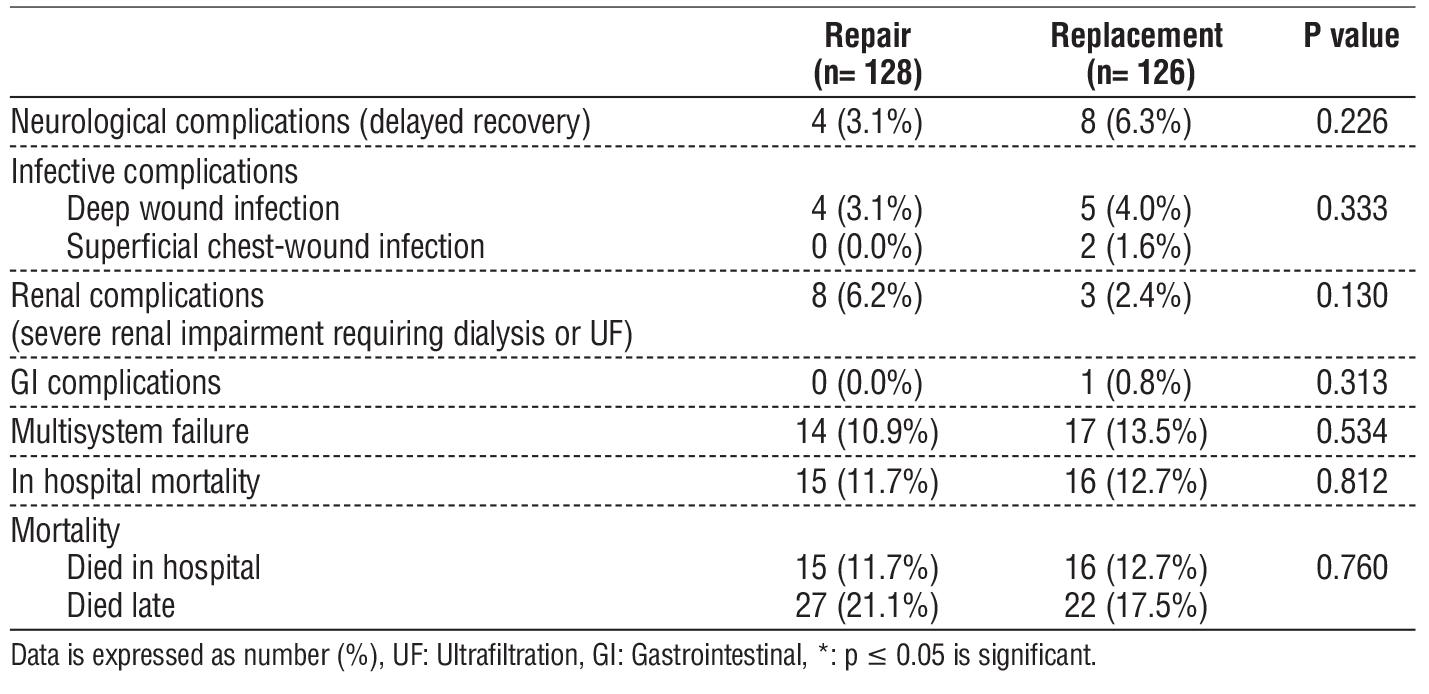
Postoperative complications and in-hospital mortality showed no significant differences between groups. Multisystem failure occurred in 31 patients, with 12 deaths in the repair group and 13 in the replacement group. In-hospital mortality was 11.7% for repair and 12.7% for replacement, with causes including heart failure, arrhythmia, and infective endocarditis. Event-free survival analysis showed 49 deaths during follow-up (21.1% in repair vs. 17.5% in replacement) (table 3).
Table 3 - Post-operative complications and mortality in the two studied groups
The repair group showed significant postoperative improvement in cardiac function, with increased ejection fraction and reduced mitral regurgitation (p=0.001, for both). Dyspnea status also improved, shifting from higher preoperative grades (2 and 3) to lower postoperative grades (1 and 2) (table 4).
Table 4 - Comparison between pre- and post-operative findings in repair group
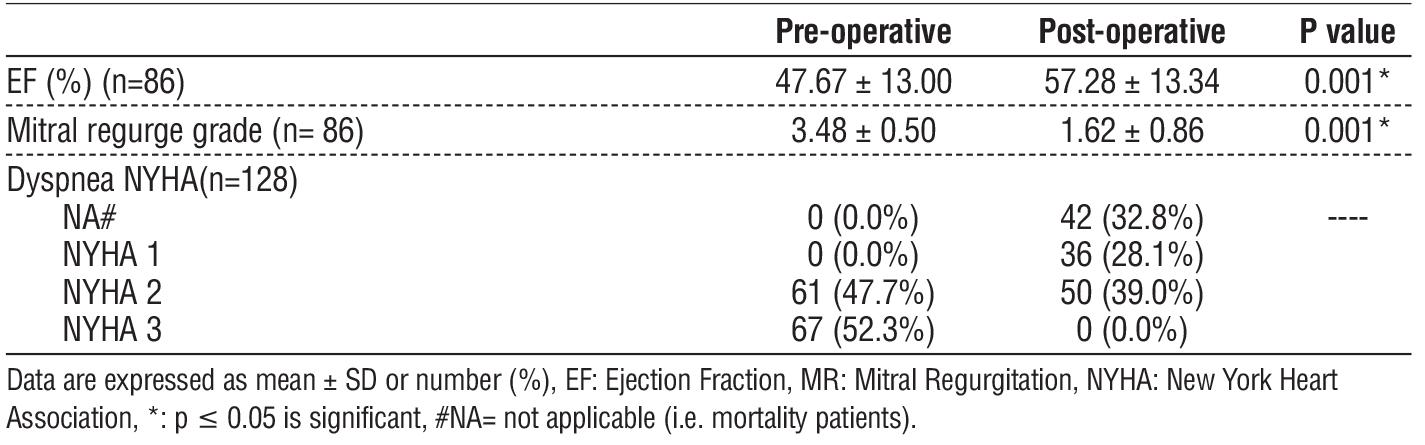
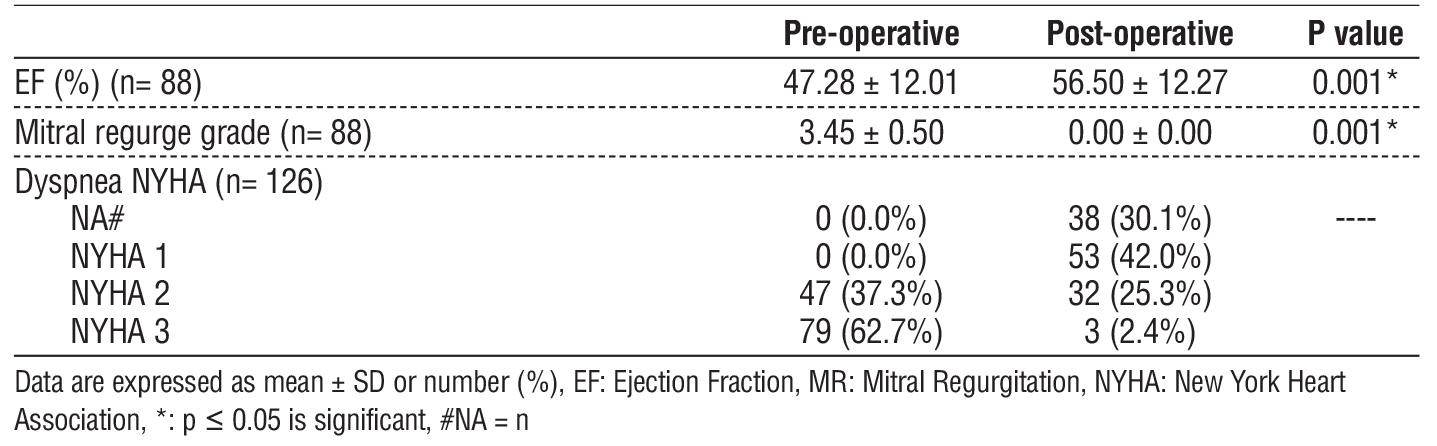
The replacement group showed significant improvement in cardiac function, with increased ejection fraction and no residual mitral regurgitation. Dyspnea status improved, shifting mostly to grades 1 and 2 postoperatively, with only three patients remaining at grade 3 (table 5).
Table 5 - Comparison between pre- and post-operative findings in replacement group
Discussion
Mitral regurgitation in ischemic heart disease is not just a valve disorder—it is a manifestation of complex ventricular pathology. The decision to repair or replace remains a surgical dilemma, where balancing long-term durability with functional recovery defines success (7). This study provides insights into the intricate trade-offs between preserving native structures and ensuring complete valve competence.
In the current study, both groups had a majority of patients in the NYHA class II-III (NYHA class III is 52.3 % in group I and 79 % in group II). This is consistent with the findings of other authors; Lam et al. reported that nearly 60% of their patients were in NYHA class III. However, it was slightly higher in other studies, such as Lam and colleagues', who classified approximately 73% of patients as NYHA class II-III (8), and Tolis et al. (9) who classified approximately 75% of patients as NYHA class II-III. In the present study, the mean EF was 47.4 % in group I and 47.13 % in group II. This was nearly identical to Chan et al. but slightly higher (40.5 % for repair and 42.4 % for replacement group) (6). However, higher than Lorusso et al (35.8% for repair and 36.6% for replacement) (10).
In the current study, there were statistical differences in preoperative heart rhythms, with 4.7 % of group I patients having AF compared to 11.9 % of group II patients. In contrast, Lorusso et al. (10) found no statistical difference between the repair and replacement groups, with 10.8 % in the repair group and 13.3 % in the replacement group) and Magne et al., who found no statistical difference between the two groups (11).
In our study, the mean cross clamp and total CPB times were 110.04 ± 32.41 min & 160.01 ± 58.42 min for the repair group, compared to 108.97 ± 50.04 & 153.27 ± 64.52 for the replacement group. With no significant changes between both. In accordance, Magne et al. (12) reported ischemic and CPB times of 100 ± 29 and 134 ± 42 minutes for MVRp, compared to 99 ± 32 and 137 ± 42 minutes for replacement, with no significant difference in cross-clamp time (105 ± 42 vs. 98 ± 39 minutes, p = 0.158). Maltais et al. (13) reported a mean CPB time of 124.4 ± 47.5 minutes (range, 30-340) and a mean cross-clamp time of 82.2 ± 31.6 minutes (range, 16.5-46.4).
Our post-operative complications as regard IABP need, Acute renal failure, Arrhythmias, Neurological complications, Reoperations and Multisystem failure; shows no significant differences, although ICU stay was significantly lower in the replacement group. This compares favorably with results obtained by Calafiore and his colleagues (14).
Hospital mortality occurred in 31 cases (15 in the repair group (11.7%) and 16 in the replacement group (12.7%)), with an overall perioperative mortality rate of 12.2%. Given the study's sample size, these figures may not be fully representative. Our findings align with previous reports, such as Magne et al. (12) (13.5% overall mortality; 9.7% for repair vs. 17.4% for replacement) and Gillinov et al. (15) (11% in-hospital mortality; 13% operative mortality).
However, our rates were higher than those reported by Chan et al. (16) (4% at 30 days) and Mantovani et al. (17) (8.2% for repair, 7.3% for replacement). Maltais et al. observed a 5% in-hospital or 30-day mortality rate. Patients with ischemic MR generally have worse prognoses than those with other mitral pathologies. Reported survival rates vary, with Gillinov et al. (15) noting 77% at one year and 55% at five years. Magne et al. (12) found comparable long-term survival between groups (6-year: 73±4% vs. 67±4%; 12-year: 48±13% vs. 47±7%). Chan et al. (16) reported five-year survival of 79.3±6.1% for repair and 60.6±8.8% for replacement. Prosthetic valves carry a higher risk of thromboembolic events, particularly mechanical valves, as highlighted by Magne et al. (12). Grossi et al. reported higher complication-free survival at five years for repair (64%) compared to replacement (47%) (18).
In our study, 100% of the patients in the replacement group in our study received mechanical valves. Some would argue that biological valves would offer an intermediate solution between repair and mechanical valves, with lower incidence of valve related events (thrombo-embolism, PVE, etc.), and better freedom from recurrent/ residual MR, particularly in a category of patients where long-term survival rates is not so high. Yet with patients presenting at younger ages, better follow-up and adjustment of postoperative medical treatment, we expect survival rates would improve and feel that the use of mechanical valves in some cases would be completely justified.
Mantovani et al. (17) recommended bioprosthetic valves for chronic IMR due to patients' limited life expectancy. However, the present study supports mechanical prostheses in younger patients, given the observed five-year survival of 73.4%. Magne et al. (12) highlighted the increasing risk of structural valve deterioration in bioprostheses over time, with age and MV position as key risk factors. Additionally, severe prosthesis-patient mismatch after MVR has been linked to reduced postoperative survival.
In this study, the replacement group remained entirely free of MR throughout the follow-up period. While MVRp may circumvent the complications associated with prosthetic valve implantation, its higher incidence of persistent or recurrent MR in patients with ischemic MR could potentially outweigh this advantage. Recurrent MR remains a notable concern following repair, with McGee et al. (19) reporting a recurrence rate of 30% within six months. Chan et al. (17) found freedom from recurrent MR (grade 2+ or higher) at six months was 95.0±3.5% for repair and 100% for replacement, decreasing at five years to 41.4±14.8% for repair and 85.7±13.2% for replacement. They suggested recurrence may result from insufficient LV reverse remodeling. While Gillinov et al. (15) indicated mixed findings on repair versus replacement outcomes, they emphasized the importance of chordal preservation in replacement. Cohn et al. and Dion et al. (20,21) concluded that MR pathophysiology and patient presentation are more critical to outcomes than the surgical approach.
Long-term survival after mitral surgery is primarily influenced by non-cardiac comorbidities such as diabetes, renal insufficiency, and age rather than the surgical approach. Maltais et al. (13) found no impact of mitral repair versus replacement on early or late survival, with severe preoperative cardiac dysfunction (LVEF 45% with significant MR) being a dominant factor. Additionally, the type of repair had no effect on outcomes.
This study is limited by its retrospective, non-randomized design and single-center setting. Longer follow-up is needed to assess durability and late complications.
Conclusion
Both MVRp and MVR significantly improved functional status and ejection fraction, with no significant difference in long-term survival. MVRp remains susceptible to recurrent regurgitation, while MVR eliminates MR but prolongs ventilation time. Surgical choice should be tailored to patient-specific factors.
Conflict of Interest
None to be declared.
Funding
None to be declared.
References
1. Grigioni F, Enriquez-Sarano M, Zehr KJ, Bailey KR, Tajik AJ. Ischemic mitral regurgitation: long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation. 2001;103(13): 1759-64.
2. Nappi F, Avtaar Singh SS, Padala M, Attias D, Nejjari M, Mihos CG, et al. The Choice of Treatment in Ischemic Mitral Regurgitation With Reduced Left Ventricular Function. Ann Thorac Surg. 2019;108(6): 1901-12.
3. Huang AL, Dal-Bianco JP, Levine RA, Hung JW. Secondary Mitral Regurgitation: Cardiac Remodeling, Diagnosis, and Management. Struct Heart. 2023;7(3):100129.
4. Asgar AW, Mack MJ, Stone GW. Secondary mitral regurgitation in heart failure: pathophysiology, prognosis, and therapeutic considerations. J Am Coll Cardiol. 2015;65(12):1231-48.
5. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021; 143(5):e35-e71.
6. Chan V, Levac-Martinho O, Sohmer B, Elmistekawy E, Ruel M, Mesana TG. When Should the Mitral Valve Be Repaired or Replaced in Patients With Ischemic Mitral Regurgitation? Ann Thorac Surg. 2017;103(3):742-7.
7. Varma PK, Krishna N, Jose RL, Madkaiker AN. Ischemic mitral regurgitation. Ann Card Anaesth. 2017;20(4):432-9.
8. Lam BK, Gillinov AM, Blackstone EH, Rajeswaran J, Yuh B, Bhudia SK, et al. Importance of moderate ischemic mitral regurgitation. Ann Thorac Surg. 2005;79(2):462-70; discussion -70.
9. Tolis GA, Jr., Korkolis DP, Kopf GS, Elefteriades JA. Revascularization alone (without mitral valve repair) suffices in patients with advanced ischemic cardiomyopathy and mild-to-moderate mitral regurgitation. Ann Thorac Surg. 2002;74(5):1476-80; discussion 80-1.
10. Lorusso R, Gelsomino S, Vizzardi E, D'Aloia A, De Cicco G, Lucà F, et al. Mitral valve repair or replacement for ischemic mitral regurgitation? The Italian Study on the Treatment of Ischemic Mitral Regurgitation (ISTIMIR). The Journal of thoracic and cardiovascular surgery. 2013;145(1):128-39.
11. Magne J, Pibarot P, Dagenais F, Hachicha Z, Dumesnil JG, Sénéchal M. Preoperative posterior leaflet angle accurately predicts outcome after restrictive mitral valve annuloplasty for ischemic mitral regurgitation. Circulation. 2007;115(6):782-91.
12. Magne J, Pibarot P, Dumesnil JG, Sénéchal M. Continued global left ventricular remodeling is not the sole mechanism responsible for the late recurrence of ischemic mitral regurgitation after restrictive annuloplasty. J Am Soc Echocardiogr. 2009; 22(11):1256-64.
13. Maltais S, Tchantchaleishvili V, Schaff HV, Daly RC, Suri RM, Dearani JA, et al. Management of severe ischemic cardiomyopathy: left ventricular assist device as destination therapy versus conventional bypass and mitral valve surgery. J Thorac Cardiovasc Surg. 2014; 147(4):1246-50.
14. Calafiore AM, Di Mauro M, Gallina S, Di Giammarco G, Iacò AL, Teodori G, et al. Mitral valve surgery for chronic ischemic mitral regurgitation. Ann Thorac Surg. 2004; 77(6):1989-97.
15. Gillinov AM, Blackstone EH, Rajeswaran J, Mawad M, McCarthy PM, Sabik JF, 3rd, et al. Ischemic versus degenerative mitral regurgitation: does etiology affect survival? Ann Thorac Surg. 2005;80(3): 811-9; discussion 09.
16. Chan KJ, Wage R, Symmonds K, Roussin I, Flather M, Pennell DJ, et al. Mitral Valve Annular, Leaflet and Papillary Muscle Geometry and Function in Functional Ischemic Mitral Regurgitation: New Insights from Cardiovascular Magnetic Resonance. Lippincott Williams & Wilkins; 2011.
17. Mantovani V, Mariscalco G, Leva C, Blanzola C, Cattaneo P, Sala A. Long-term results of the surgical treatment of chronic ischemic mitral regurgitation: comparison of repair and prosthetic replacement. J Heart Valve Dis. 2004;13(3):421-8; discussion 8-9.
18. Grossi EA, Goldberg JD, LaPietra A, Ye X, Zakow P, Sussman M, et al. Ischemic mitral valve reconstruction and replacement: comparison of long-term survival and complications. J Thorac Cardiovasc Surg. 2001;122(6):1107-24.
19. McGee EC, Gillinov AM, Blackstone EH, Rajeswaran J, Cohen G, Najam F, et al. Recurrent mitral regurgitation after annuloplasty for functional ischemic mitral regurgitation. J Thorac Cardiovasc Surg. 2004;128(6):916-24.
20. Cohn LH, Rizzo RJ, Adams DH, Couper GS, Sullivan TE, Collins JJ, Jr., et al. The effect of pathophysiology on the surgical treatment of ischemic mitral regurgitation: operative and late risks of repair versus replacement. Eur J Cardiothorac Surg. 1995;9(10):568-74.
21. Dion R, Benetis R, Elias B, Guennaoui T, Raphael D, Van Dyck M, et al. Mitral valve procedures in ischemic regurgitation. J Heart Valve Dis. 1995;4 Suppl 2S124-9; discussion S9-31.
Full Text Sources:
Abstract:
Views: 725

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.