Surgery, Gastroenterology and Oncology
|
Introduction: Lower abdominal pain is caused by various gastrointestinal tract (GIT) emergencies, including acute appendicitis, intestinal obstruction, acute perforated diverticulitis, obstructed hernia, and iatrogenic colon perforation. Therefore, laparoscopy may be of diagnostic and therapeutic value.
Methods: Between April 2017 and April 2020, 793 patients with lower GIT emergencies, including acute appendicitis, acute intestinal obstruction, complicated colonic diverticulum, complicated hernias, and iatrogenic colonic perforations, were included.
Results: The most common age was under 40 (63%), with a male predominance (75%). Acute appendicitis (77%), intestinal obstruction (8%), acute perforated diverticulitis (4%), obstructed hernia (9%), and iatrogenic colonic perforation (2%) were the main causes of lower GIT emergencies. Inferior epigastric artery injury (0.3%), urinary bladder injury (0.4%), appendicular artery bleeding (0.9%), omental hemorrhage (0.6%), intestinal injury (0.9%), splenic injury (0.3%), and duodenal injury (0.1%) were the most prevalent intraoperative complications. The conversion rate was 48 (6%), with 37 patients converted due to difficult dissection or obstructed anatomy, particularly during IO surgery, followed by appendicular surgery. In 206 (26%) of the cases, postoperative complications occurred. Pneumonia (n=55), wound infections (n=35), and ileus (n=22) were the most common postoperative complications. Re-intervention occurred in 53 cases (53/793, 6.7%), with causes including appendicular surgery (13 cases), IO surgery (12 patients), diverticulitis surgery (12 patients), and hernia surgery (12 patients), and iatrogenic perforation surgery (4 patients). The death rate was 3%.
Conclusion: In cases of acute appendicitis and obstructed hernia, as well as in the hands of skilled surgeons, the laparoscopic method is considered possible and safe; however, in other cases, such as IO, perforated diverticular disease, and iatrogenic colonic perforation, it is not.
Introduction
Acute lower abdomen is typically caused by peritoneal irritation due to inflammation, rupture, or hollow organ obstruction. Patients with severe acute lower abdominal pain either proceed to the operating room or undergo additional investigations or diagnostic laparoscopy (DL). Laparoscopy should not be used routinely in cases of acute lower abdomen due to anesthetic risks and morbidity (1).
Most hospitals perform emergency abdominal surgeries, and laparotomy in these procedures is associated with high mortality rates (14 to 20%) (2-3). Laparoscopic surgery has become a standard diagnostic and therapeutic tool in abdominal emergencies. It has been employed in some situations of lower abdominal crises in recent years (4).
General surgeons frequently face diagnostic challenges in cases of emergency abdominal conditions. Diagnosis is crucial for planning an appropriate abdominal incision and for avoiding unnecessary surgery. Non--invasive diagnostic approaches, such as radiological examinations, are not always conclusive. Furthermore, they are costly and cannot be performed 24 h a day in all hospital circumstances (5). This retrospective observational study was designed to analyze the intraoperative and postoperative outcomes of the laparoscopic technique in emergent lower GIT surgeries.
Material and Methods
Design of the study and participants
Between April 2017 and April 2020, 793 patients experienced lower GIT emergencies, including acute appendicitis, acute intestinal obstruction, complicated colonic diverticulum, complicated hernias, and iatrogenic colonic perforations. To be eligible for the study, patients must meet all of the following criteria: >18 years of age, both sexes, and have undergone laparoscopic surgery for acute lower GIT emergencies,, such as acute appendicitis, acute intestinal obstruction, complicated colonic diverticulum, complicated hernias, and iatrogenic colonic perforations. The exclusion criteria were age < 18 years and a history of open surgery. The STROBE criteria were followed for reporting work and registration in a clinical trial.
Types of outcomes (clinical endpoints)
Intraoperative complications were the primary outcome. Postoperative complications were the secondary outcome.
Method
Perioperative evaluation and approach
Plain radiography, abdominal ultrasonography, and computed tomography (CT) were performed to confirm the diagnosis (CT). For three years, all surgeries were performed in a single location. The procedures were performed as instructed (6-10). All the patients were tracked for 24 months after discharge from the hospital. Patients were approached by phone, outpatient clinic visits, or e-mails. Comprehensive history review, clinical examination, USS, and CT were performed during the follow-up period. None of the patients was lost to follow-up.
Statistical analysis
The mean SD was used for normally distributed continuous variables, and the median was used for non-normally distributed continuous variables. Percentages were used to represent categorical variables. The test results were examined to determine whether they were within the normal range. SPSS version 20 (SPSS, Chicago, IL, USA) was used for all the statistical analyses.
Results
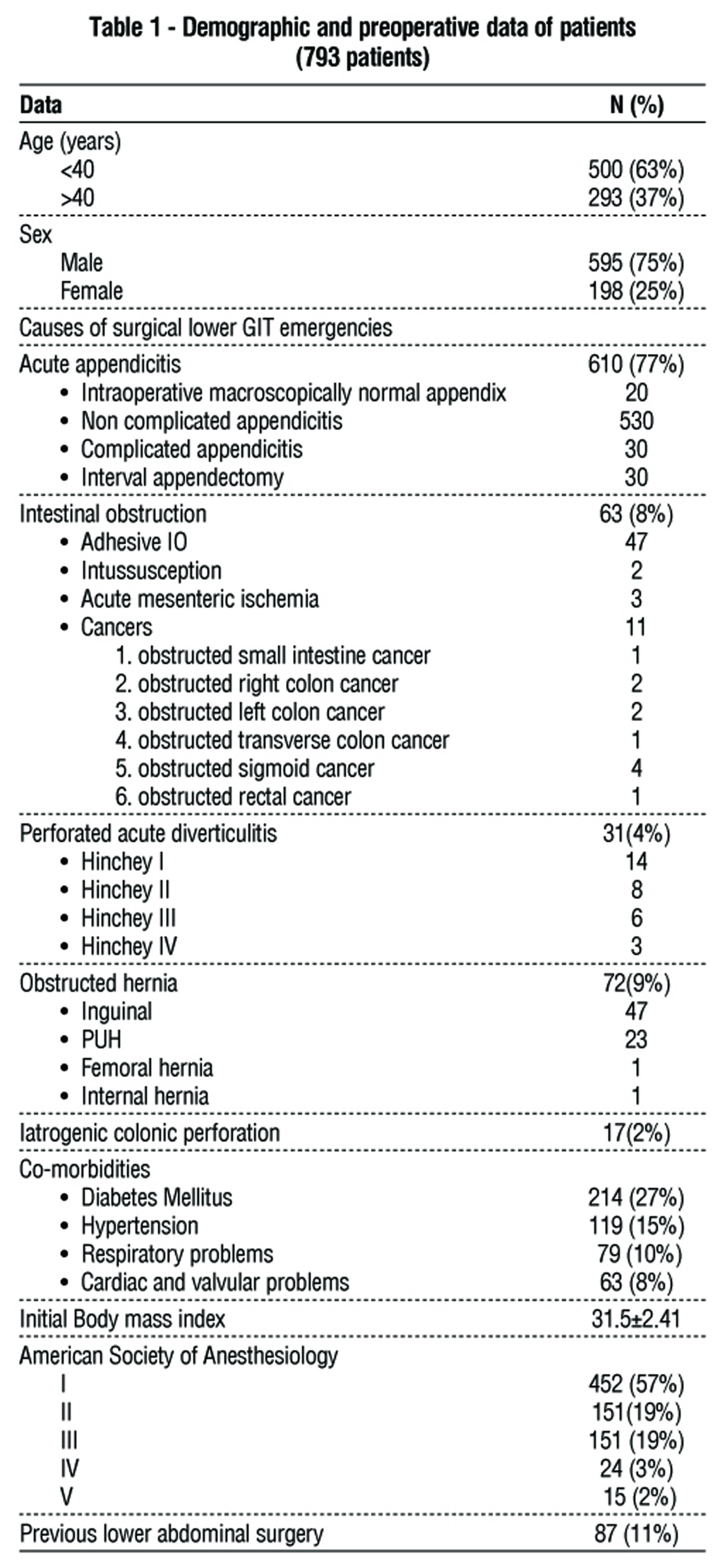
Preoperative and demographic characteristics of the study participants are shown in table 1. The most common age was under 40 (63%), with a male predominance (75%). Acute appendicitis (77%), intestinal obstruction (8%), acute perforated diverticulitis (4%), obstructed hernia (9%), and iatrogenic colonic perforation (2%) were the main causes of lower GIT emergencies. Diabetes mellitus was the most prevalent comorbidity (27%), whereas ASA I was the most common (57%). In 11% of individuals, previous lower abdominal operations were present.
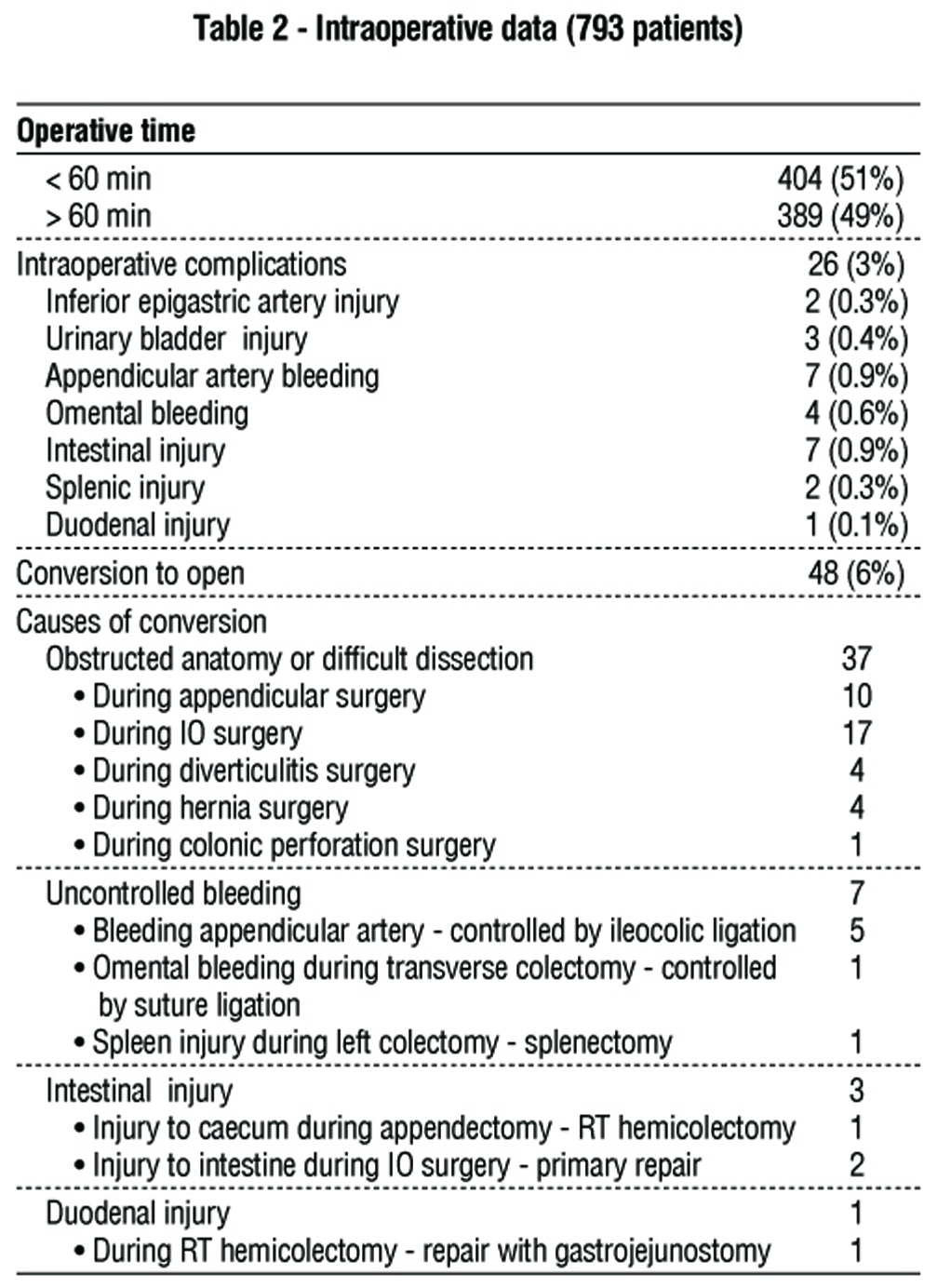
Table 2 displays intraoperative findings. In 49% of cases, the operation took more than an hour. Inferior epigastric artery injury (0.3%), urinary bladder injury (0.4%), appendicular artery bleeding (0.9%), omental hemorrhage (0.6%), intestinal injury (0.9%), splenic injury (0.3%), and duodenal injury (0.1%) were the most prevalent intraoperative problems. The conversion rate was 48 (6%), with 37 patients converted due to difficult dissection or obstructed anatomy, particularly during IO surgery, followed by appendicular surgery.
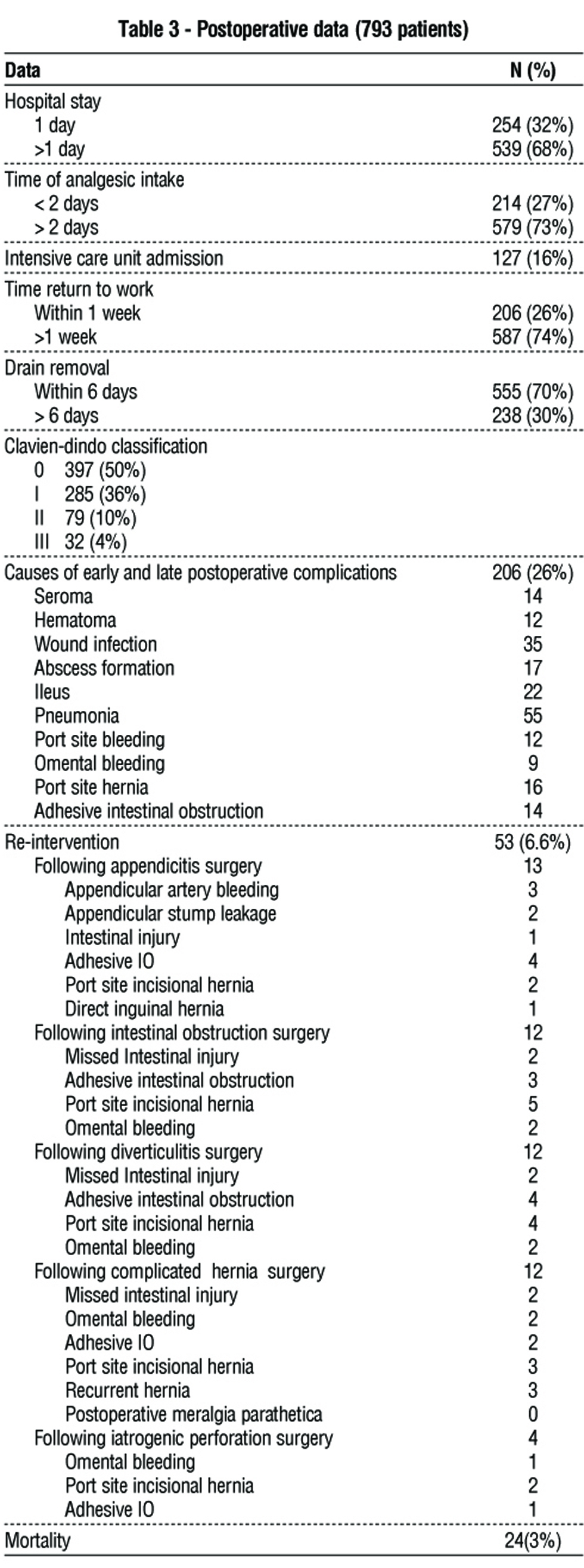
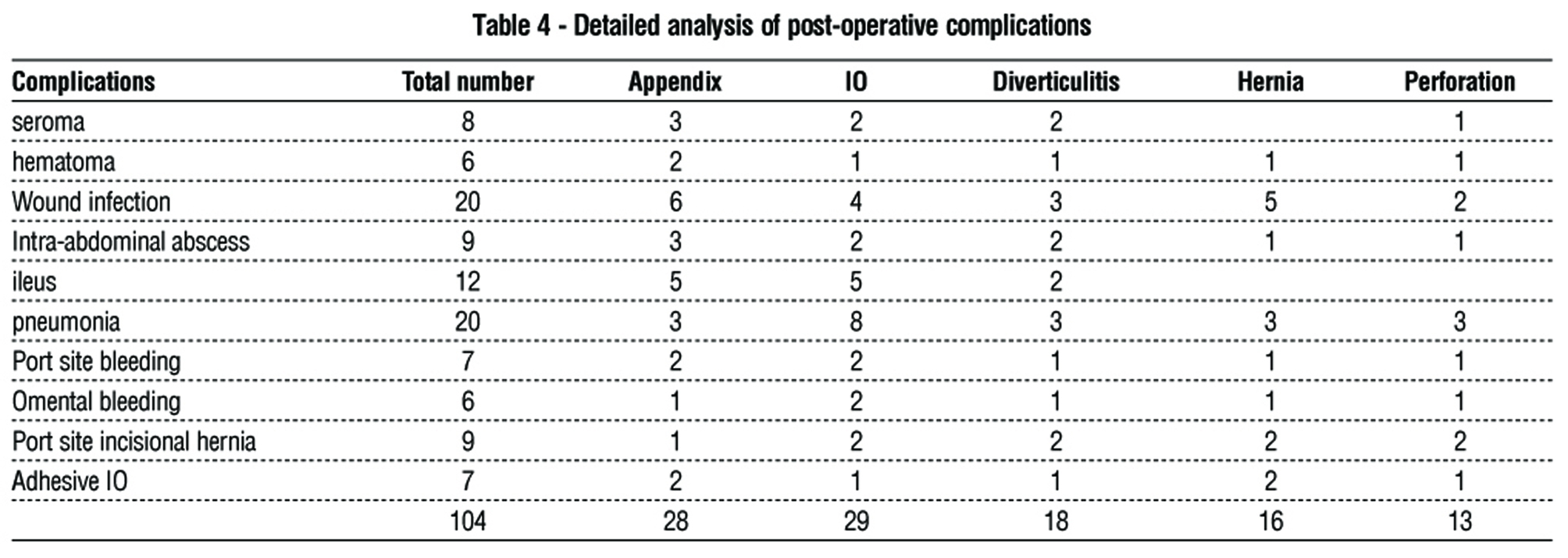
Postoperative data are shown in table 3. Most patients required more than one day in the hospital, with 16% requiring ICU admission. In 206 (26%) of the cases, postoperative complications occurred. Pneumonia (n=55), wound infections (n=35), and ileus (n=22) were the most common postoperative complications. Re-intervention occurred in 53 cases (53/793, 6.7%), with causes including appendicular surgery (13 cases), IO surgery (12 patients), diverticulitis surgery (12 patients), and hernia surgery (12 patients), and iatrogenic perforation surgery (4 patients). The death rate was 3% (table 4).
Discussion
Role of laparoscopic approach in acute appendicitis
Laparoscopy is safe for the diagnosis and treatment of acute appendicitis (11). Laparoscopic appendectomy has many benefits, including lower abdominal wall morbidity, especially in obese patients; better assessment of the extent of sepsis (subphrenic collection, generalized peritonitis); less postoperative pain; faster recovery; earlier return to normal activity; better cosmetic results; easier localization and removal of an ectopic appendix; decreased abdominal wall morbidity; and complete evaluation of the abdominal cavity in cases of diagnostic doubt (12). While Li et al. found a low wound infection rate (3.81%) following a laparoscopic appendectomy, they also found a slightly higher incidence of intraoperative bleeding, postoperative abdominal abscess, and urinary tract infection. 9.51% of patients were converted from laparoscopy to open appendectomy (13). These benefits are particularly significant in obese patients (14).
In cases of complicated appendicitis, a previous study recommended laparoscopic appendectomy for severe appendicitis because of the low rate of surgical intra-abdominal abscess, quick recovery time, rapid return to oral intake, and brief hospital stay (15). During the Covid-19 era, there was a higher incidence of complicated appendicitis after abscess drainage, such as appendicular abscesses and recurrent appendicitis. There has been debate about the use of laparoscopy or an open approach after appendicular abscess drainage to contain virus spread (16-17).
In our analysis, The most common emergencies performed at our facility were acute appendicitis (610, 77%), predominantly non-complicated appendicitis (530/610). The number of laparoscopic appendectomies performed in our facility decreased during the COVID-19 pandemic. The most common intraoperative problems we encountered were appendicular artery hemorrhage in 7 patients (0.9%) that slipped during dissection and were treated in 2 patients, while five patients required open conversion to control the bleeding via ileocolic artery ligation. Postoperative complications occurred in 28 patients, including port-site wound infections(n = 6), ileus (n = 5), and pneumonia (n = 3). Reintervention was required in 13 patients after appendectomy due to appendicular artery bleeding (3 patients), appendicular stump leakage (2 patients), intestinal damage (1 patient), adhesive IO (4 patients), incisional hernia (2 patients), and direct inguinal hernia (1 patient). We conclude that laparoscopic repair of acute appendicitis is safe and feasible, with few intraoperative and postoperative complications. The lower incidence and safety of laparoscopy in the treatment of acute appendicitis have been accepted in previous studies (18-20). The increased rate of postoperative wound infection is attributable to the large number of patients who undergo laparoscopic appendectomy. Furthermore, we did not employ a retrieval bag to remove the inflamed appendix as in other studies (21).
We encountered a normal intraoperative appendix. Our center's procedure involved the removal of
apparently normal appendices for microscopic early mucosal inflammation, and the risk of recurrent
appendicitis was significant. According to a previous study, 10% to 15% of appendectomies are carried out for a healthy appendix (22). This concept was agreed upon in another study (23). However, other studies did not advocate appendectomy in the normal macroscopic appendix owing to the low incidence of recurrent appendicitis (1).
Laparoscopic approach in intestinal obstruction
Adhesions, tumors, strangulated hernias, intussusception, and paralytic ileus can cause intestinal obstructions. Electrolyte and fluid imbalances, intestinal ischemia and stasis, microbial proliferation in the intestinal lumen, and bacterial translocation through the intestinal wall are consequences of this condition. (24). Laparoscopic management of acute IO is challenging because of the restricted working space produced by the ileus, fragility of dilated intestinal loops, and difficulty in determining the cause of obstruction in some patients. As intestinal injuries are potentially lethal, bowel manipulation requires utmost care. The laparoscopic method's conversion rates can range from 0% to 52%, depending on surgeon’s experience and patient choice (25-26). In contrast, earlier studies have found that laparoscopy is safe and feasible for emergency colorectal obstruction, with good outcomes in terms of hospital stay and mortality reduction (4).
Intestinal obstruction occurred in 63 patients (8%) in our study, with adhesive IO being the most common cause (47/63). The most common cause of malignant obstruction is sigmoid colon obstruction. Intraoperative complications necessitated conversion in 21 patients (21/63, 33%). One patient underwent splenectomy due to splenic injury during the left hemicolectomy, one patient underwent exploration due to intestinal injury with primary resection and anastomosis, and one patient underwent exploration due to duodenal injury during the right hemicolectomy, and the tear was repaired. Pneumonia, ileus, and wound infections were the most prevalent postoperative complications. Postoperative problems necessitated reintervention in 12 patients (12/63, 19%), including missed intestinal injuries in two patients, adhesive IO in three, port site incisional hernia in five, and omental hemorrhage in two. Laborious dissection with a limited working area was the cause of the increased intraoperative and postoperative difficulties. No intraoperative enterotomy was performed. We conclude that Laparoscopy in IO is difficult and dangerous, with significant intraoperative and postoperative complications. These findings are consistent with previous studies (27). However, Li et al. (28) reported low overall complication rates, and that the laparoscopic method was safer than open treatment when performed by skilled surgeons in carefully selected patients.
Role of laparoscopy in obstructed hernia
Laparoscopic hernia repair, including TAPP repair, is a viable option for treating incarcerated inguinal hernias, provided that sufficient anatomical knowledge and expertise are available to dissect and decrease the sac with favorable outcomes (4,9). Research has also shown that emergency surgery has the same rates of intra- and postoperative problems and recurrences as elective surgery (4). Therefore, patients who meet these requirements may undergo laparoscopic treatment of incarcerated ventral hernias. Adhesiolysis must be performed appropriately; atraumatic graspers must be used; and the contents of the defect must be thoroughly inspected for blood supply, motility, and integrity.
In our study, laparoscopy was performed in 72 patients (9%), with TAPP for inguinal hernia being the most common surgery. As previously documented, we employed a percutaneous transabdominal external needle to close the hernial defect (29) and used a tacker or histoacryl to secure the mesh (9,30). Intra-operative complications necessitated open conversion in four patients (4/72,5.5%), with wound infection and pneumonia being the most prevalent postoperative sequelae. Owing to proper sac dissection with nerve sparing, no patients experienced postoperative meralgia parathetica, a finding comparable to that of a prior study examining the value of laparoscopic hernia surgery (31). Reintervention was performed in 12 patients (12/72, 16.6%) due to missed intestinal damage (n=2), omental hemorrhage (n=2), adhesive IO (n=2), port site incisional hernia (n=3), and recurring hernia (n=3). We discovered that laparoscopic repair of an obstructed hernia is safe and possible,, with few intraoperative and postoperative complications. In our investigation, the incidence of wound infection was lower than that reported in earlier studies (32) and was most likely related to differences in the approach and method.
Role of laparoscopy in acute perforated diverticulitis
Treatment of acute diverticulitis with laparoscopy is feasible and safe, with complication rates ranging from zero to 54 percent. Previous studies have described using laparoscopic surgery to treat diverticulitis, reporting positive outcomes, such as low complication rates, no deaths, and gastrointestinal (GI) healing rates of up to 90%. However, to date, only a few cases have been reported (33). A systematic review of laparoscopic peritoneal lavage for perforated diverticular diseases included 231 patients from two prospective cohort studies and nine retrospective case series. The mortality rate was 1.7%, with a morbidity rate of 10.4%. Abdominal and systemic infections were successfully treated in 95.7% of patients, with only 37.7% requiring subsequent resection (34).
Thirty-one patients with perforated colonic diverticulum underwent laparoscopic surgery. Due to obstructed anatomy or difficult dissection, conversion occurred in four patients (4/31, 13%). As previously stated, we performed intraoperative colonic lavage and resection with end-to-end or side-to-end colorectal anastomoses (35). Pneumonia and wound infections were the most prevalent postoperative consequences. Due to missed intestinal injury (2), adhesive IO (4), port site incisional hernia (4), and omental bleeding (2), 12 patients (12/31, 39%) required re-intervention. The feasibility and safety of the laparoscopic approach for perforated diverticulitis are questionable, owing to the high morbidity and re-intervention rates.
Role of laparoscopy in iatrogenic colonic perforationIatrogenic colonic perforation is the most serious risk associated with diagnostic and therapeutic colonoscopy. If the bacterial load in the colon spreads to the peritoneal cavity, peritoneal contamination,peritonitis, and systemic sepsis can develop rapidly, dramatically increasing the risk of morbidity and fatality. Colonic perforation rates have increased over the past decade owing to the increasing use of colono-scopy for diagnostic and therapeutic purposes (36-40). Iatrogenic perforation is a rare, but serious complication of several surgical procedures. The Literature reports a risk of up to 0.66% during diagnostic colonoscopy and up to 2.14% during therapeutic procedures (10,37,38,41), with mortality risk up to 25.6%.(37). Although this is a relatively rare complication, advances in treatment over the past decade have made it more manageable and have opened up new options for surgeons and endoscopists.
If the patient's colon has already been prepped, they have the option of primary repair or non-operative treatment. Preparing the colon reduces the number of bacteria present within the colon and the risk of peritoneal contamination. For perforations < 1 cm in size, endoscopists are advised to perform endoscopic clipping to close the perforation promptly. (42-43).
Few studies have investigated the use of laparoscopic access for managing iatrogenic colonic perforation, despite recent suggestions that laparoscopic procedures may be safe and successful in this setting (44-46). Previous studies have reported no morbidity or mortality rates (47-50).
We included 17 patients who underwent laparoscopic treatment for iatrogenic colonic perforations. One patient (1/17,6%) required conversion to open surgery because of difficult dissection and the failure to locate perforations. Most patients who experienced postoperative complications developed pneumonia (3/17, or 17.6%). Four patients (23.5%) required additional surgery after the first procedure failed. Wounds can be repaired with simple colonorrhaphy (1 or 2-layer stitches) or tangential resection. Primary colonic repairs are more likely to be successful and can be accomplished as soon as possible after diagnosis; therefore, timely diagnosis and surgery are essential. When stitched, there were two layers. Laparoscopic resection or colonic diversion, such as the Hartmann operation (Patient 2), can be performed effectively if a primary colonic suture is not possible, owing to the state of the colon and peritoneal contamination. Bowel resection, ileostomy, or colonic diversion may be necessary because of high levels of peritoneal contamination and colon anomalies. If the perforation is in the retroperitoneum, it is critical to wash the abdomen thoroughly (we used to perform lavage with 6 to 8 L of saline solution) and observe the precise location of the perforation with broad mobilization of the colon. The actual non--invasive treatment is conservative therapy, which some authors recommend for particular patients (51). On the other hand, it is not completely risk free. Owing to the increased risk of peritoneal infection, poor outcome, significant morbidity, and death from sepsis, more extensive surgical operations may be required if conservative treatment fails or the surgical approach is delayed (42). Laparoscopic surgery is not recommended for the treatment of colonic perforations.
Conclusion
In cases of acute appendicitis and obstructed hernia, as well as in the hands of skilled surgeons, the laparos-copic method is considered possible and safe. However, this is not the case in other cases, such as IO, perforated diverticular disease, and iatrogenic colonic perforation.
Strength and limitations
The retrospective nature and limited scope of the study due to being conducted at a single center are two significant limitations. We ensured that the information was accurate, and reduced the possibility of bias.
Registration
Criteria for registering on the quality control review protocol on clinicaltrials.gov protocol.
Conflict of interest
All author declare that they have no conflict ofinterest.
Funding
No funding sources.
Ethical statement
The Faculty of Medical Ethics Committee of Zagazig University provided ethical consent. All participants provided written informed consent for publication. All authors contributed to the conception and design of the study, acquisition of data, analysis, interpretation of data, drafting of the article, critical revision for important intellectual content, and final approval of the version to be submitted.
This study was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
References
1. Sauerland S, Agresta F, Bergamaschi R, Borzellino G, Budzynski A, Champault G, et al. Laparoscopy for abdominal emergencies: evidence-based guidelines of the European Association for Endoscopic Surgery. Surg Endosc. 2006;20(1):14-29.
2. Saunders DI, Murray D, Pichel AC, Varley S, Peden CJ; UK Emergency Laparotomy Network. Variations in mortality after emergency laparotomy: the first report of the UK Emergency Laparotomy Network. Br J Anaesth. 2012;109(3):368-75.
3. Stoneham M, Murray D, Foss NB. Emergency surgery: the big three - abdominal aortic aneurysm, laparotomy and hip fracture. Anaesthesia. 2014;69 Suppl 1:70-80.
4. Agresta F, Ansaloni L, Baiocchi GL, Bergamini C, Campanile FC, Carlucci M, et al. Laparoscopic approach to acute abdomen from the Consensus Development Conference of the Società Italiana di Chirurgia Endoscopica e nuove tecnologie (SICE), Associazione Chirurghi Ospedalieri Italiani (ACOI), Società Italiana di Chirurgia (SIC), Società Italiana di Chirurgia d’Urgenza e del Trauma (SICUT), Società Italiana di Chirurgia nell’Ospedalità Privata (SICOP), and the European Association for Endoscopic Surgery (EAES). Surg Endosc. 2012; 26(8):2134-64.
5. Memon MA, Fitzgibbons Jr RJ. The role of minimal access surgery in the acute abdomen. Surg Clin North Am. 1997;77(6):1333-53.
6. Habeeb TAAM, Hussain A, Schlottmann F, Kermansaravi M, Aiolfi A, Matic I, et al. Recurrent appendicitis following successful drainage of appendicular abscess in adult without interval appendectomy during COVID-19. Prospective cohort study. Int J Surg. 2022; 97:106200.
7. Jensen SA-MS, Fonnes S, Gram-Hanssen A, Andresen K, Rosenberg J. Long-term mortality and intestinal obstruction after laparoscopic cholecystectomy: A systematic review and meta-analysis. Int J Surg. 2022;105:106841.
8. Gregori M, Cassini D, Depalma N, Miccini M, Manoochehri F, Baldazzi GA. Laparoscopic lavage and drainage for Hinchey III diverticulitis: review of technical aspects. Updates Surg. 2019;71(2): 237-246.
9. Habeeb TAAM, Mokhtar MM, Sieda B, Osman G, Ibrahim A, Metwalli A-EM, et al. Changing the innate consensus about mesh fixation in trans-abdominal preperitoneal laparoscopic inguinal hernioplasty in adults: Short and long term outcome. Randomized controlled clinical trial. Int J Surg. 2020;83:117-124.
10. Bleier JI, Moon V, Feingold D, Whelan RL, Arnell T, Sonoda T, et al. Initial repair of iatrogenic colon perforation using laparoscopic methods. Surg Endosc. 2008;22(3):646-9.
11. Habeeb TAAM, Mokhtar MM, Lotfy M, Osman G, Ibrahim A, Riad M, et al. Grey Zone Appendicitis (Intermediate Risk Alvarado Score 5-6): Role of Blood Test Biomarkers to Detect Early Appendicitis and to Decrease the Incidence of Negative Appendectomy. Cost and Effectiveness. Randomized Controlled Trial. Surg Chron 2020;25(4): 339-342.
12. Wang YC, Yang HR, Chung PK, Jeng LB, Chen RJ. Laparoscopic appendectomy in the elderly. Surg Endosc. 2006;20:887-9.
13. Li X, Zhang J, Sang L, Zhang W, Chu Z, Li X, et al. Laparoscopic versus conventional appendectomy: a meta-analysis of randomized controlled trials. BMC Gastroenterol. 2010;10:129.
14. Mason RJ, Moazzez A, Moroney JR, Katkhouda N. Laparoscopic vs open appendectomy in obese patients: outcomes using the American College of Surgeons National Surgical Quality Improvement Program database. J Am Coll Surg 2012;215(1): 88-99.
15. Takami T, Yamaguchi T, Yoshitake H, Hatano K, Kataoka N, Tomita M, et al. A clinical comparison of laparoscopic versus open appendectomy for the treatment of complicated appendicitis: Historical cohort study. Eur J Trauma Emerg Surg. 2020;46(4):847-851.
16. Habeeb TAAM, Hussain A, Schlottmann F, Kermansaravi M, Aiolfi A, Matic I, et al. Recurrent appendicitis following successful drainage of appendicular abscess in adult without interval appendectomy during COVID-19. Prospective cohort study. Int J Surg. 2022; 97:106200.
17. Shaker SE, Habeeb TAAM, Wasefy T, Fiad AA, Elgohary M, Rashad NM, et al. The Commonest Medical, Surgical, and Oncological Causes of Acute Abdomen in Adults with COVID-19. A prospective observational study. Surg. Gastroenterol. Oncol. 2022;27(3):182-190.
18. Ibrahim EM, Alnaimy TA, Elkilanty M. Advancement in the role of laparoscopy in complicated appendicitis. Kasr El Aini Journal of Surgery.2018;19(3):1-5.
19. Di Saverio S, Podda M, De Simone B, Ceresoli M, Augustin G, Gori A, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020; 15(1):27.
20. Werkgartner G, Cerwenka H, El Shabrawi A, Bacher H, Hauser H, Mischinger HJ, et al. Laparoscopic versus open appendectomy for complicated appendicitis in high risk patients. Int J Colorectal Dis. 2015;30(3):397-401.
21. Lasheen AE, Elaziz OA, Elaal SA, Alkilany M, Sieda B, Alnaimy T. Surgical wound infections after laparoscopic appendectomy with or without using reusable retrieval bag: a retrospective study. J Minim Invasive Surg Sci. In Press(In Press):e36894.
22. Fingerhut A, Millat B, Borrie F. Laparoscopic versus open appendectomy: time to decide. World J Surg. 1999;23(8):835-45.
23. Navez B, Therasse A. Should every patient undergoing Laparoscopy for clinical diagnosis of appendicitis have an appendicectomy ? Acta Chir Belg. 2003;103(1):87-9.
24. Rana SV, Bhardwaj SB. Small intestinal bacterial overgrowth. Scand J Gastroenterol 2008;43(9):1030-7.
25. Farinella E, Cirocchi R, La Mura F, Morelli U, Cattorini L, Delmonaco P, et al. Feasibility of laparoscopy for small bowel obstruction. World J Emerg Surg. 2009;4:3.
26. Koh FH, Tan KK, Tsang CB, Koh DC. Laparoscopic versus an open colectomy in an emergency setting: a case-controlled study. Ann Coloproctol. 2013;29(1):12-6.
27. Dindo D, Schafer M, Muller MK, Clavien PA, Hahnloser D. Laparoscopy for small bowel obstruction: the reason for conversion matters. Surg Endosc. 2010;24(4):792-7.
28. Li MZ, Lian L, Xiao LB, Wu WH, He YL, Song XM. Laparoscopic versus open adhesiolysis in patients with adhesive small bowel obstruction: a systematic review and meta-analysis. Am J Surg. 2012;204(5):779-86.
29. Lasheen AE, Abd Elaal S, Alkilany M, Alnaimy T, Ibrahim A, Baiomy T, et al. Percutaneous transabdominal external needle for hernia defect closure in laparoscopic repair. Edorium J Surg 2016;3:18–23.
30. Refaat DO, Al naimy TA, Boghdady MA, Mahmoud AM. Tack versus Cyanoacrylate Mesh Fixation in Laparoscopic Inguinal Hernioplasty. 2022;28(4):679-685.
31. Sieda B, Riad M, Alnaimy T. A comparative study of the incidence of postoperative meralgia paraesthetica after open inguinal hernioplasty and after laparoscopic transabdominal preperitoneal approach repair for recurrent inguinal hernia. The Egyptian Journal of Surgery. 2015;34(3):127-134.
32. Abul futoh Abdel Karim AK, Mustafa IM, Lotfy W, Alnaimy TA. Repair of Strangulated Umbilical Hernia with or without Mesh. Zagazig University Medical Journal. 2023;29(1,2):119-124.
33. Cirocchi R, Arezzo A, Vettoretto N, Cavaliere D, Farinella E, Renzi C, et al. Role of damage control surgery in the treatment of Hinchey III and IV sigmoid diverticulitis: a tailored strategy. Medicine (Baltimore). 2014;93(25):e184.
34. Toorenvliet BR, Swank H, Schoones JW, Hamming JF, Bemelman WA. Laparoscopic peritoneal lavage for perforated colonic diverticulitis: a systematic review. Colorectal Dis. 2010;12(9):862-7.
35. Habeeb TAAM, Mohammad H, Wasefy T, Mansour MI. Outcomes of side-to-end versus end-to-end colorectal anastomosis in non-emergent sigmoid and rectal cancers: randomized controlled clinical trial. Ann Coloproctol. 2022 Mar 11.
36. Yang DH, Byeon JS, Lee KH, Yoon SM, Kim KJ, Ye BD, et al. Is endoscopic closure with clips effective for both diagnostic and therapeutic colonoscopyassociated bowel perforation? Surg Endosc. 2010;24(5):1177-85.
37. Iqbal CW, Chun YS, Farley DR. Colonoscopic perforations: a retrospective review. J Gastrointest Surg. 2005;9(9):1229-35: discussion 1236.
38. Hagit T, Madhala-Givon O, Wasserberg N, Lelcuk S, Niv Y. Incidence and management of colonoscopic perforations: 8 years' experience. World J Gastroenterol. 2006;12(26):4211-3.
39. Ker TS, Wasserberg N, Beart RW Jr. Colonoscopic perforation and bleeding of the colon can be treated safely without surgery. Am Surg. 2004;70(10):922-4.
40. Taku K, Sano Y, Fu KI, Saito Y, Matsuda T, Uraoka T, et al. Iatrogenic perforation associated with therapeutic colonoscopy: a multicenter study in Japan. J Gastroenterol Hepatol. 2007;22(9):1409-14.
41. Avgerinos DV, Llaguna OH, Lo AY, Leitman IM. Evolving management of colonoscopic perforation. J Gastrointest Surg. 2008; 12(10):1783-9.
42. Trecca A, Gaj F, Gagliardi G. Our experience with endoscopic repair of large colonoscopic perforations and review of the literature. Tech Coloproctol. 2008;12(4):315-21; discussion 322.
43. Heresbach D. Prise en charge des perforations coliques au cours de la coloscopie en 2009. Treatment of colonic perforations during colonoscopy in 2009. Acta Endosc. 2009;39:92-99.
44. Alfonso-Ballester R, Lopez-Mozos F, Marti-Obiol R, Garcia-Botello SA, Lledo-Matoses S. Laparoscopic treatment of endoscopic sigmoid colon perforation: a case report and literature review. Surg Laparosc Endosc Percutan Tech. 2006;16(1):44-6.
45. Hansen AJ, Tessier DJ, Anderson ML, Schlinkert RT. Laparoscopic repair of colonoscopic perforations: indications and guidelines. J Gastrointest Surg. 2007;11(5):655-9.
46. Kilic A, Kavic SM. Laparoscopic colotomy repair following colonoscopic polypectomy. JSLS. 2008;12(1):93-6.
47. Pilgrim CH, Nottle PD. Laparoscopic repair of iatrogenic colonic perforation. Surg Laparosc Endosc Percutan Tech. 2007;17(3):215-7.
48. Busi? Z, Lovri? Z, Busi? V, Cavka M, Lemac D. Laparoscopic treatment of iatrogenic endoscopic sigmoid colon perforation: a case report and literature review. J Laparoendosc Adv Surg Tech A. 2007;17(3):324-5.
49. Volpe A, Piccoli M, Colli G, Mecheri F, Melotti G. Laparoscopic treatment of colonoscopic perforation: a case report. Chir Ital. 2007;59(4):587-90. Italian
50. Mattei P, Alonso M, Justinich C. Laparoscopic repair of colon perforation after colonoscopy in children: report of 2 cases and review of the literature. J Pediatr Surg. 2005;40(10):1651-3.
51. Lüning TH, Keemers-Gels ME, Barendregt WB, Tan ACITL, Rosman C. Colonoscopic perforations: a review of 30,366 patients. Surg Endosc. 2007;21(6):994-7.
Full Text Sources:
Abstract:
Views: 5794

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.