Surgery, Gastroenterology and Oncology

|
|
Gentleman in his late 70s presented with right side abdominal pain and flank pain in the rural hospital setting with a computed tomography finding of right adrenal haemorrhage. The patient was stable throughout the admission however, was transferred to a tertiary centre for optimal care and radiology intervention services availability. He was treated conservatively and was well and asymptomatic during phone call follow up 1 month later.
Introduction
A rare case of symptomatic adrenal haemorrhage presenting to the Emergency Department in a rural hospital. Adrenal haemorrhage can present in a wide spectrum from non-specific abdominal pain to haemodynamically unstable due to active bleeding. We are reporting of a stable, symptomatic patient and discussed on actions taken with patient safety as the focus of care throughout the episode. Patient communication was another highlight in this case report as we have interviewed the patient in two different settings, during initial presentation and 1 month after discharge to provide a holistic picture of the case.
Case presentation
This is gentleman in his late 70s presented to Emergency Department in a rural hospital with right upper quadrant pain started at 2 o’clock in the morning. It was a localised pain and was aggravated with breathing. Otherwise, no fever or urinary tract symptoms and clinically stable. On examination, chest was clear, abdomen was soft and minimally tender over right upper quadrant. Murphy sign was negative, no renal angle tenderness, and no evidence of peritonism. Patient has a history of left renal carcinoma that was removed 4 years ago with oncology follow up. His last CT scan for this oncology follow up was in November 2023 and did not reveal any pathology in the right adrenal gland.
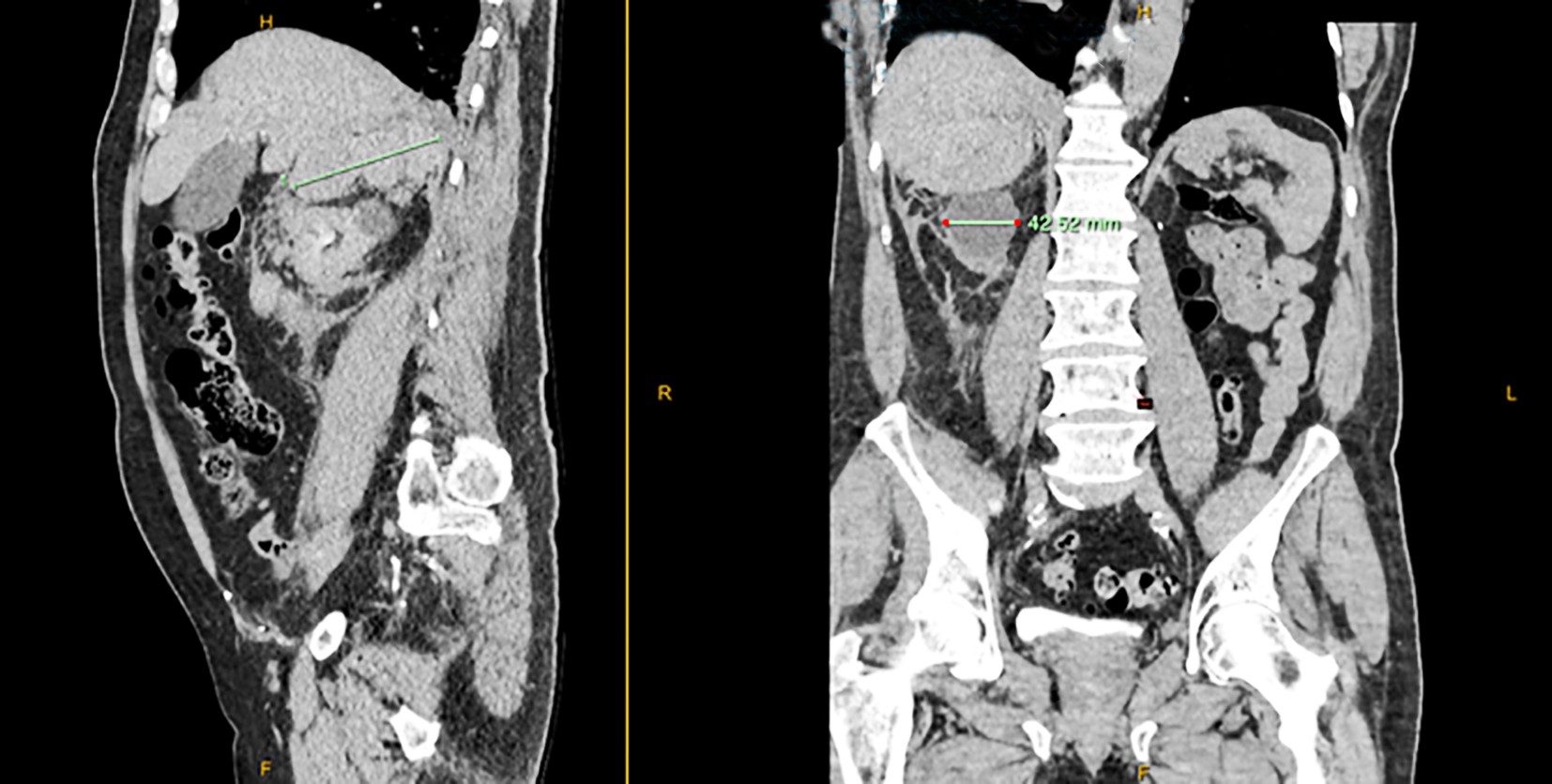
Emergency physician initial differential diagnosis was pulmonary embolism, nephrolithiasis, spontaneous pneumothorax and musculoskeletal pain or a urinary tract infection. A CTPA was ordered during which the radiology technician noticed abnormalities in right renal region and decision was made by radiologist to perform a Computed topography of the Abdomen and Pelvis with delayed contrast phase. CT showed right adrenal haemorrhage with the maximum diameter of 9 cm and mild non-specific mesenteric panniculitis (comparable stable to previous imaging) as shown in fig. 1 a, b in different view.
Figure 1 a, b - The computed topography image of the adrenal haemorrhage
Investigations
Normal haemoglobin value and other blood parameters within normal range. Vital signs were within normal range throughout presentation and admission.
Differential Diagnosis Prior to CT Scan
1. Nephron/uretheric lithiasis;
2. Musculoskeletal pain;
3. Urinary tract infection;
4. Spontaneous pneumothorax.
Treatment
Strict bed rest during presentation to Emergency department and close monitoring. He was kept fasted with maintenance intravenous fluids in addition to adequate pain relief with the regular Paracetamol and Endone as per needed.
Outcome and Follow-up
Patient was treated conservatively and transferred to a tertiary hospital after discussing with the relevant surgical team. Interventional radiology services are about 3 hours away although this patient didn’t require any intervention at that stage, it was thought best to observe him in a unit where they can do definitive care should he experience a re-bleed. He was transferred and admitted for observation for 2 days prior to discharge with general practitioner follow up. A follow up call was made 1 month later and the patient was asymptomatic and able to perform daily activities without restriction.
Discussion
Adrenal haemorrhage is rare disease with estimation of 0.14% to 1.8% found to have bilateral adrenal haemorrhage in post-mortem examinations (1).
Diagnosis is challenging as presentation can be non-specific and, in most cases, they do have a pre-disposing factor such as recent surgery or trauma as a cause (2). Other risk factors would be anticoagulation therapy, sepsis (example Waterhouse-Frederichsen syndrome), metastasis, and recent trauma. However, we do not see any of the risk factors in this gentleman and we did consider adrenal metastasis that may have caused a spontaneous bleed (3). Imaging such as computed tomography (CT) remains essential in diagnosing this disease. As we can see from this case, the initial suspicion of pulmonary embolism was ruled out and subsequently picking up abnormality at the right adrenal region with the usage of CT scan (4). Given his history of left renal cancer and uncertainty around the extent of his renal oncological surgery, we had to keep in mind that he may not have a left adrenal gland and that haemorrhage in the right adrenal could have cause acute adrenal insufficiency. Most patients presenting to Emergency Department having abdominal pain with certain degree of risk factors, unlike the case we have here (5,6).
Conclusions
-
Adrenal haemorrhage should remain one of the differential diagnoses despite patient having normal vital signs, normal blood count and no risk factor.
2. Early recognition and diagnosis of adrenal haemorrhage will allow better planning, in this case is transferring from a rural hospital to a tertiary centre with the capability to perform arterial embolization.
3. Explaining the pathology in simple terms to the patient to improve their understanding, reducing their anxiety and stress demand as physiological stress may provide certain amount of risk in adrenal haemorrhage, especially if at risk of adrenal insufficiency.
Conflict of Interest
No conflict of interest.
Funding
No funding sources.
Ethical Statement
Not applicable.
References
1. Kovacs KA, Lam YM, Pater JL. Bilateral massive adrenal hemorrhage. Assessment of putative risk factors by the case-control method. Medicine (Baltimore). 2001;80(1):45-53.
2. Roupakias S, Papoutsakis M, Tsikopoulos G. Adrenal injuries following blunt abdominal trauma in children: report of two cases. Ulus Travma Acil Cerrahi Derg. 2012;18(2):171-4.
3. Guarner J, Paddock CD, Bartlett J, Zaki SR. Adrenal gland hemorrhage in patients with fatal bacterial infections. Mod Pathol. 2008;21(9):1113-20.
4. Dunnick NR, Korobkin M. Imaging of adrenal incidentalomas: current status. AJR Am J Roentgenol. 2002;179(3):559-68.
5. Nasser B, Bughrara MS, Alakhras H, Nasser Z, Jameel OF. Unilateral Adrenal Hemorrhage: A Rare Complication of Anticoagulant Use. Cureus. 2022;14(6):e25821.
6. Mangone A, Yousuf Q, Arlt W, Prete A, Shaheen F, Krishnasamy S, et al. A case of unilateral post-COVID-19 adrenal haemorrhage and follow-up during pregnancies. Endocrinol Diabetes Metab Case Rep. 2022;2022:22-0337.
Full Text Sources:
Abstract:
Views: 2093

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.