Surgery, Gastroenterology and Oncology

|
|
Introduction. Abdominal aortic aneurysm (AAA) is a common vascular disease. The endovascular repair, compared with open repair, was associated with early survival advantage. Objective. In this study we assess the complications of AAA within short term period of 3 months after Endovascular aneurysm repair (EVAR).
Patients and methods. This is a prospective study at Ghazi Al-Hariry Hospital in Medical City of Bagdad, deals with patients having an infrarenal AAA who underwent Endovascular aneurysm repair (EVAR) from September 2021 to September 2024 with total of 60 patients.
Results. The mean age is 64 years, with males of about 79%. Hospital stays are about 3 days. The technical success rate is 100% without conversion to the open surgery. Regarding the complications, the 30-day mortality rate is 0% and an overall mortality rate of 2(3.3%), both dead with MI after 3 days of procedure. Specific complications included myocardial infarction MI 2(3.3%) and acute lower limb ischemia 2(3.3%). Graft related complication develops type I endoleak 1(1.6%) presented after 55 days with abdominal pain, anemia and abdominal swelling.
Conclusion. The short follow-up period may not catch long-term complications and the rate of re-interventions.
Introduction
Abdominal aortic aneurysm (AAA) is a common vascular disease that affects men older than 60 years. As the size of the aneurysm increases, the risk of rupture increases (1). Minimally invasive repair was first reported in 1986 (2). AAA shows benefits of Endovascular aneurysm repair (EVAR) with respect to 30-day mortality (3). The Endovascular repair, compared with open repair, was associated with early survival advantage that gradually decreased over time (4). Endovascular repair was associated with increased rates of graft-related complications and re-interventions and was more costly (5). The peri-operative and long-term survival, re-interventions, and complications after endovascular repair compared with open repair of abdominal aortic aneurysm are less (6). In this study we assess the complications within short term period of 3 months after EVAR.
Method
This is a prospective study at Ghazi Al-Hariry Hospital in Medical City of Bagdad, deals with patients having an infrarenal AAA who underwent EVAR from September 2021 to September 2024 with total of 60 patients. The aim of the study is to look for the early and short-term complications associated with EVAR after 3 months period. Procedures were done under spinal anaesthesia in the peripheral catheterisation department by vascular surgeon specialists.
After an open and direct access to both common femoral artery (CFA), or via brachial artery approach or crossover technique, then an insertion of 6F introducer sheaths, advancing a flush catheter over a guide-wire to the suprarenal aorta, followed by an angiogram of the aorta and both iliac arteries to assess the proximal neck, angulations, and access arteries were done. An appropriated dose of intravenous heparin was given, and super-stiff wires were used for exchanges. The main body of the stent graft was introduced below the renal artery and an additional angiogram performed before the deployment of the proximal end. The contralateral iliac tube graft was advanced over another super-stiff wire and completion angiogram confirmed total exclusion of the aneurysm and ensured normal blood flow to the lower extremities. Post-procedure, for each patient, the follow-up involved clinically and with CTA angiography a 3 months later to monitor for complications and the integrity of the graft.
Ethical Approval
The Medical Ethical Committee of The Al-Najaf Cardiac Center approved this study (no.220924 on 8/7/2020). Participant consent was waived by the committee since only patient files were reviewed.
Results
In this study, 60 patients underwent EVAR during the period of study. Data shows patient with mean age of (64 ± 2) years, with males of about 47 (79%). Regarding the comorbidities, hypertension 46 (77%), diabetes mellitus 38(36.3%), chronic obstructive pulmonary disease (COPD) 9(15%) and coronary artery disease (CAD) 18(30%) and the history of smoking is 49(81.7%). The average aortic aneurysms diameter was from 5.8 – 10.3 cm. as in table 1.
Table 1 - Shows the number of patients and percentage related to co-mortalities.

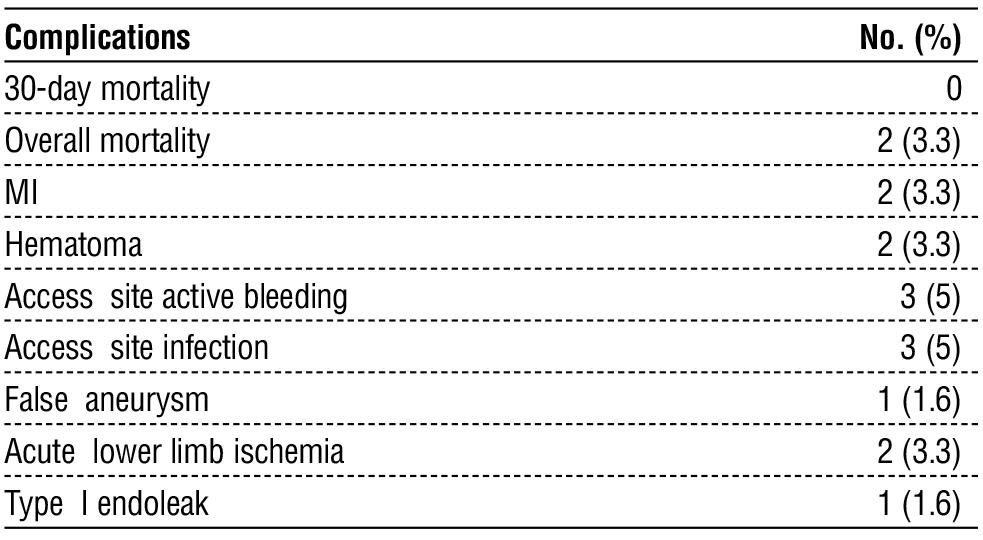
Hospital stays are about 3 days. The technical success rate is 100% without conversion to the open surgery. Regarding the complications, the 30-day mortality rate is 0% and an overall mortality rate of 2(3.3%), both dead with MI after 3 days of procedure. Specific complications included myocardial infarction MI 2(3.3%), various wound complications include (hematoma 2(3.3%), access site active bleeding 3(5%), access site infection 3(5%) and false aneurysm 1(1.6%)) and acute lower limb ischemia 2(3.3%). Graft related complication develops type I endoleak 1(1.6%) presented after 55 days with abdominal pain, anemia and abdominal swelling as in table 2.
Table 2 - The complications and mortality rate.
Discussion
This study, primarily composed of males (79%) with an average age of 64, shows the procedure’s efficacy. This demographic is unlike the findings of Felice et al. who reported 98% male with average ages over 70 years (7) and T Ohki study in which 86.8% were male with age of 72.3 years (8).
Common comorbidities included hypertension 46 (77%), diabetes mellitus 38 (36.3%), chronic obstructive pulmonary disease (COPD) 9 (15%) and coronary artery disease (CAD) 18 (30%) and the history of smoking is 49 (81.7%) which are comparable to from Abdulrasak et al. This is related to various sample size and some cultural factors (9).
The procedural outcomes have a success rate of 100% with patients staying an average of 3 days in the hospital. The 30-day mortality rate was 0% and an overall mortality rate was 3.3% that is higher than Rajesh et al study in which the overall mortality was 1·1 deaths per 100 person-years (10) and comparable to EVAR trial participants (11). This is may be due to small sample size and highest co morbidities of our patients.
Graft related complication develops type I endoleak occur because of an incompetent seal at the proximal (1.6%) presented after 3 months with abdominal pain and anemia, so the patients need for postoperative monitoring and the treatment involves placement of an aortic cuff extension. This is unlike Cernohorsky et al study in which the endoleak 1-3 types account 15-30% (12). The sample size and short time follow up are related causes.
The acute lower limb ischemia occurs in 2 (3.3%), both are caused by embolism. This is unlike Maldonado et al study in which the ischemia occurs in 9% (13).
Conclusion
The short follow-up period may not catch long-term complications and the rate of re-interventions, so the future researches should involve larger patient numbers, multi-centers and longer follow-up to provide more detailed efficacy and safety of EVAR for aortic aneurysms.
Authors’ Contributions
Abdulameer M. Hussein; Conceptualization; Data Curation; Investigation; Methodology; Project administration; Resources; Software; Writing – original draft and Writing – review & editing. Sabah Noori Jaber; Conceptualization; Data Curation; Investigation; Methodology; Project administration; Resources; Writing – original draft and Writing – review & editing. Ahmed Muhi Fahad; Conceptualization; Data Curation; Investigation; Methodology; Project administration; Resources; Writing – original draft and Writing – review & editing.
Conflicts of Interest
The authors declare no conflict of interest regarding this article.
Funding: None.
References
1. Meuli L, Zimmermann A, Menges AL, Stefanikova S, Reutersberg B, Makaloski V. Prognostic model for survival of patients with abdominal aortic aneurysms treated with endovascular aneurysm repair. Sci Rep. 2022;12(1):19540.
2. Buck DB, van Herwaarden JA, Schermerhorn ML, Moll FL. Endovascular treatment of abdominal aortic aneurysms. Nat Rev Cardiol. 2014;11(2):112-23. Epub 2013 Dec 17. Erratum in: Nat Rev Cardiol. 2014;11(2):i.
3. AlOthman O, Bobat S. Comparison of the Short and Long-Term Outcomes of Endovascular Repair and Open Surgical Repair in the Treatment of Unruptured Abdominal Aortic Aneurysms: Meta-Analysis and Systematic Review. Cureus. 2020;12(8):e9683.
4. O'Donnell TFX, Patel VI, Deery SE, Li C, Swerdlow NJ, Liang P, et al. The state of complex endovascular abdominal aortic aneurysm repairs in the Vascular Quality Initiative. J Vasc Surg. 2019;70(2): 369-380.
5. Keegan A, Hicks CW. Surgical Decision-Making and Outcomes in Open Versus Endovascular Repair for Various Vascular Diseases. Anesthesiol Clin. 2022;40(4):627-644.
6. England A, Mc Williams R. Endovascular aortic aneurysm repair (EVAR). Ulster Med J. 2013;82(1):3-10.
7. Mirabella D, Evola S, Dinoto E, Setacci C, Pakeliani D, Setacci F, et al. Outcome Analysis of Speed Gate Cannulation during Standard Infrarenal Endovascular Aneurysm Repair. J Clin Med. 2023;12(19): 6263.
8. Silva NP, Amin B, Dunne E, Hynes N, O'Halloran M, Elahi A. Implantable Pressure-Sensing Devices for Monitoring Abdominal Aortic Aneurysms in Post-Endovascular Aneurysm Repair. Sensors (Basel). 2024;24(11):3526.
9. Yamanaka K, Hamaguchi M, Chomei S, Inoue T, Kono A, Tsujimoto T, et al. Japanese single-center experience of abdominal aortic aneurysm repair over 20 years: should open or endovascular aneurysm repair be performed first? Surg Today. 2023;53(10): 1116-1125.
10. Kulig P, Lewandowski K, Rudel B, Chwa?a M, Piwowarczyk M, Mrowiecki W. Clinical evaluation of endovascular repair of abdominal aortic aneurysm based on long-term experiences. Wideochir Inne Tech Maloinwazyjne. 2021;16(1):191-198.
11. Imaeda Y, Ishibashi H, Orimoto Y, Maruyama Y, Mitsuoka H, Arima T. Randomized Controlled Trial of Oral Tranexamic Acid Intervention for the Prevention of Type II Endoleak after Endovascular Abdominal Aneurysm Repair. Ann Thorac Cardiovasc Surg. 2022;28(4):286-292.
12. Padmanabhan C, Poddar A. Infections of the aorta. Indian J Thorac Cardiovasc Surg. 2022;38(Suppl 1):101-114.
13. Yanamaladoddi VR, Sarvepalli SS, Vemula SL, Aramadaka S, Mannam R, Sankara Narayanan R, et al. The Challenge of Endoleaks in Endovascular Aneurysm Repair (EVAR): A Review of Their Types and Management. Cureus. 2023;15(5):e39775.
Full Text Sources:
Abstract:
Views: 738

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.