Surgery, Gastroenterology and Oncology

|
|
Aim: The benefits of laparoscopic approach over open surgery have been demonstrated in recent decades and development of Single incision laparoscopic surgery (SILS) aimed to reduce invasiveness of multiport laparoscopy. Our aim is to compare results of single incision laparoscopic (SILS) appendectomy and multiport laparoscopic (MPL) appendectomy in this prospective study.
Material and Methods: 25 consecutive patients who underwent SILS appendectomy (group 1) were compared with 25 patients who underwent MPL appendectomy (group 2) during the same period. Data consisting of patient characteristics, definitive diagnosis, operation time, blood loss, hospital stay time, complications, pain scores, rate of conversion to MPL and open surgery and satisfaction rate of cosmetic outcome were collected.
Results: 23 (92%) SILS appendectomies and 22 (88%) MPL appendectomies were completed successfully. The operation time was significantly longer in groups 1 (57.60±18,99 vs. 37.20 ± 7.91 minutes, p?0.001). Higher pain scores and better cosmetic outcomes were observed in group 1 (p<0.05) with no significant difference in complication rates between groups (p>0.05).
Conclusion: SILS appendectomy seems to be an acceptable alternative to MPL appendectomy with acceptable results. SILS is a safe, feasible and effective technique for appendectomy. Despite higher postoperative pain, cosmetic satisfaction is excellent in SILS group.
INTRODUCTION
Minimally invasive surgical techniques have developed during recent decades, aiming to reduce surgical invasiveness and patient morbidity. As a minimally invasive alternative to open appendectomy, laparoscopic appendectomy was first performed by Semm in 1983 and gradually gained acceptance (1). Comparative studies result in better diagnostic accuracy, reduced use of analgesics, shorter recovery time and a lower rate of wound infection in conventional Multiport Laparoscopic Surgery (MPL) comparing to open appendectomy (2). Single-Port access Laparoscopic Surgery (SILS) is a minimally invasive technique that has been applied to several abdominal operations including appendectomy, aiming to reduce trauma of surgical access and to improve cosmetic results over MPL (2-5). The main proposed benefit of using SILS technique for appendectomy is absence of a visible scar by concealing the incision in umbilicus (6). Reduced postoperative pain, shorter recovery times, and improved cosmetic outcomes are among the anticipated benefits of SILS appendectomy compared to MPL; however, these results require prospective evaluation (7). Current research indicates that SILS appendectomy is both feasible and safe, yet additional comparative studies are needed. Consequently, we conducted a prospective comparison of the outcomes of SILS appendectomy versus conventional MPL appendectomy at our hospital.
MATERIAL AND METHODS
Study Groups and Inclusion Criteria
The study received approval from the Ethical Committee of the Turkish Ministry of Health, and informed consent was obtained from all participants. Data were collected from fifty patients diagnosed with acute appendicitis who met the inclusion criteria and were consecutively prepared for laparoscopic appendectomy by a single surgeon at our hospital from February 2019 to February 2022. The participants, comprising 38 males and 12 females, ranged in age from 21 to 64 years, with a mean age of 31.38±10.20 years. They were randomly assigned to either the SILS appendectomy group (Group 1, n=25) or the MPL appendectomy group (Group 2, n=25).
Exclusion Criteria
Patients with an ASA score of four or higher, as well as those deemed unsuitable for laparoscopic surgery, were excluded from this study. Additionally, individuals with a history of prior abdominal surgery, pregnancy, previous peritonitis, or those currently undergoing peritoneal dialysis were also excluded.
Preoperative Preparation and Postoperative Assessment
Preoperative assessment, anesthetic procedures, and antibiotic therapy were uniformly administered to all patients. A dosage of 1 gram of intravenous ampicillin and sulbactam was given 30 minutes prior to the skin incision. Key variables such as demographics, body mass index (BMI), ASA score, operative morbidity and mortality, duration of surgery, postoperative pain assessment results, length of hospital stay, cosmetic satisfaction rates, and occurrences of conversion to MPL or open appendectomy were meticulously recorded. For postoperative pain management, Tenoxicam (40 mg daily) was utilized, with an additional 50 mg of Tramadol provided as needed. The Visual Analogue Scale (VAS) was employed to assess postoperative pain levels at the sixth hour (POSH-VAS) and on the first postoperative day (POFD-VAS) (8). Morbidity was evaluated based on the incidence of gastrointestinal leaks, wound infections, reoperations, hospital readmissions, and incisional hernias. Cosmetic outcomes were rated on a scale from 1 (indicating the lowest satisfaction) to 5 (indicating the highest satisfaction) at the six-month postoperative mark.
Surgical Procedure
Surgical procedures were conducted under general anesthesia with orotracheal intubation. Patients were positioned supine with a slight left tilt to improve exposure of the pericaecal area. Standard intra-
peritoneal CO2 insufflation was carried out at pressures ranging from 12 to 14 mmHg in both groups. A urinary catheter was placed under general anesthesia and subsequently removed at the conclusion of the operation. In all cases, 10 mL of 0.25% Bupivacaine was infiltrated at the incision sites before skin closure to optimize postoperative pain management.
SILS Appendectomy
A 15mm vertical skin incision and a 20mm vertical fascial incision were made directly at the base of the umbilicus, with stay sutures placed on both sides. A flexible SILS port (Covidien Inc., Norwalk, CT, USA), which features an insufflation port and three trocar holes, was introduced using an open access technique to gain entry into the intraperitoneal cavity. Insufflation was initiated following the placement of the trocars. The surgeon and assistant positioned themselves to the left of the patient. Articulated instruments utilized in the procedure included 5mm graspers (Roticulator Endo-Grasp and Roticulator Endo-Dissect; Autosuture, Ascot, UK) and flexible scissors (Roticulator Endo Mini-Shears; Autosuture). After dissecting the mesoappendix with LigaSure, the base of the appendix was ligated using an Endo-Loop (Ethicon, US) and then transected. The appendix was subsequently extracted using an Endo-Catch (Covidien Inc., Norwalk, CT, USA). Following the extraction, the fascia and skin were closed with polypropylene sutures. To enhance umbilical cosmesis, subcutaneous 4/0 poliglecaprone absorbable sutures were applied. In three cases of perforated appendicitis, vacuum drains were placed through the incision, and all drains were removed on the second post-operative day.
MPL Appendectomy
A vertical skin and fascia incision, measuring 15 mm, was made at the base of the umbilicus, followed by intraperitoneal CO2 insufflation using a Veress needle. An initial exploration was conducted through an 11 mm trocar placed at the incision site, with an additional 11 mm trocar inserted in the right upper quadrant. A 5 mm trocar was also positioned along the midline, approximately 6 to 8 cm below the initial umbilical trocar. Dissection of the mesoappendix was performed with LigaSure, and the base of the appendix was ligated using an Endo-Loop. The appendix was then removed utilizing an Endo-Catch device. The closure of the umbilical fascia and skin incision was achieved with a polypropylene suture. A vacuum drain was placed through the 5 mm trocar incision and extended to the rectovesical or rectovaginal pouch. The drains were removed on the second postoperative day.
Statistical Analysis
The clinical and demographic data of the cases were analyzed using the parametric t-test. This same test was employed to evaluate operating times and the duration of hospital stays. For comparing pain scores and cosmetic outcomes, the non-parametric Mann-Whitney U test was utilized. Fisher’s exact test was applied to assess complication rates. Data analysis was conducted using SPSS statistical software (version 16.0; SPSS Inc., Chicago, IL, USA), with a significance level set at 0.05.
RESULTS
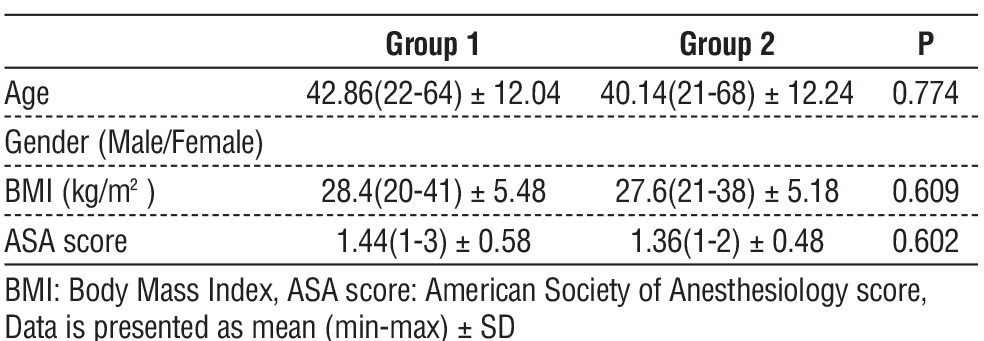
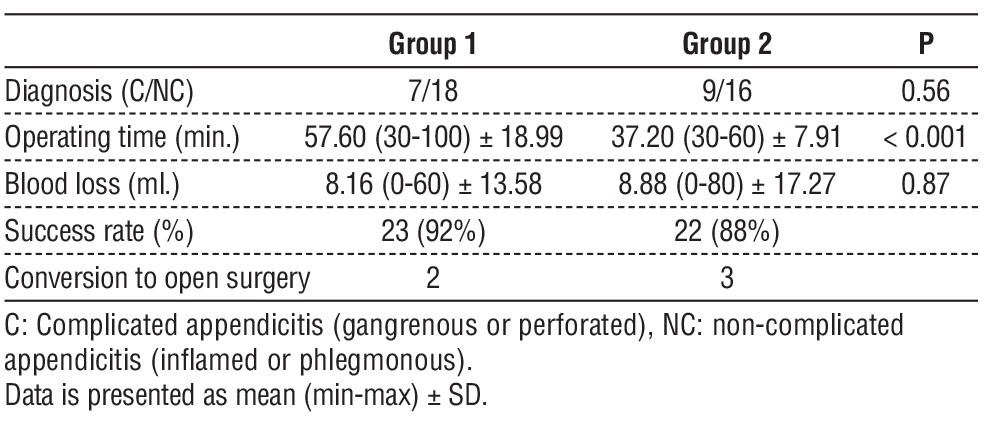
A total of 50 patients (38 male and 12 female) were enrolled with a diagnosis of acute appendicitis. Table 1 presents the characteristics of the patients. There were no significant variations in age, gender, diagnosis, ASA score, or BMI between the two groups. Successful completion rates were high, with 23 (92%) SILS appendectomies and 22 (88%) MPL appendectomies performed successfully. Two cases from the SILS group and three from the MPL group were converted to open surgery due to difficulties in dissecting the appendicular area. The correlation between diagnosis and conversion was found to be significant (p<0.001), with all conversions to open surgery occurring in cases of complicated appendicitis. Notably, one patient in group 1 was classified as morbidly obese. However, we observed no correlation between body mass index (BMI) and the conversion rate (p > 0.05).
Table 1 - Patients’ characteristics
No surgical complications, such as bleeding or injury to luminal organs, were observed during the procedure. The average blood loss remained comparable between the two groups (p = 0.87). The operating data is detailed in table 2. The mean operating time for Group 1 was 57.60±18.99 minutes, whereas for Group 2, it was 37.20±7.91 minutes. Notably, the operating time for Group 1 was significantly longer than that for Group 2 (p < 0.001).
Table 2 - Operative data
The mean operating time for the first five cases in Group 1 was 86.00 ± 8.94 minutes, compared to 50.50 ± 13.50 minutes for the subsequent cases. This decrease in operating time after the initial five cases proved to be statistically significant (p = 0.005).
Pain score analyses indicated statistically significant differences between the groups. The POSH-VAS score was significantly higher in group 1 compared to group 2 (p = 0.002). Although the POFD-VAS score was also higher in group 1, it did not reach statistical significance (2.76 vs 2.44, p = 0.10). Additionally, the correlation between operating time and POFD-VAS was examined. The Pearson Correlation Coefficient (PCC) test revealed a significant correlation between pain scores and operating time (p < 0.001). When the POSH-VAS scores between the groups were compared after excluding the first five SILS cases, no statistical difference was found (p = 0.38). Postoperative data are presented in table 3.
No intraoperative complications occurred during the procedures. One patient in Group 1 experienced abdominal distention and ileus for two days, which was managed conservatively. There were no cases of stump leaks among the patients. The length of hospital stays was comparable between the two groups. On the seventh postoperative day, one patient in Group 2 was diagnosed with an intraabdominal abscess. Percutaneous drainage was performed, and the drain was removed after four days. Additionally, two patients from Group 1 and three patients from Group 2 were readmitted to the hospital due to superficial wound infections. These infections were treated with local wound dressing and antibiotic therapy. The complication rates are detailed in table 4.
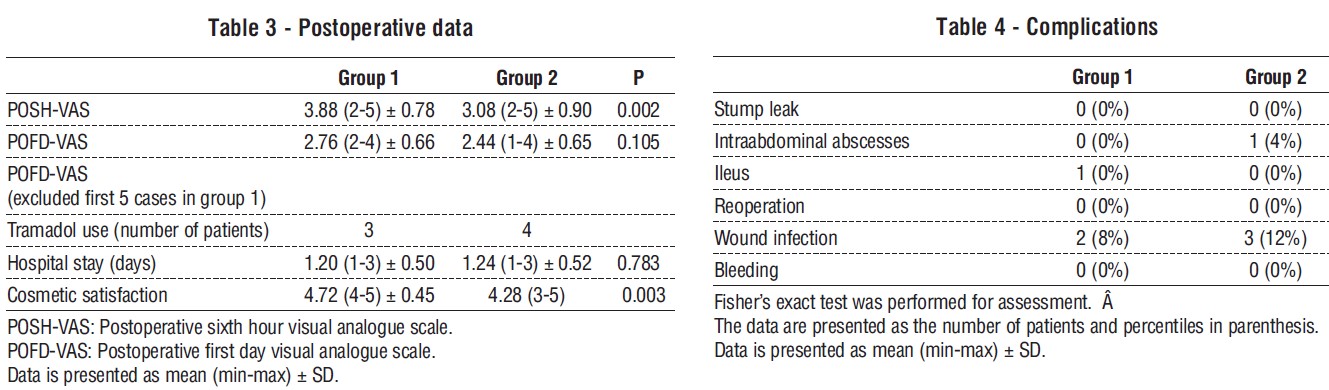
The average follow-up time was 19.68 ± 8.72 months (ranging from 2 to 36 months). There were no instances of herniation at the incision site in either group. The cosmetic satisfaction scores showed a statistically significant difference between the two groups (p = 0.003). As anticipated, patients who underwent SILS appendectomy expressed greater satisfaction with the scarless umbilical incision (refer to table 3).
DISCUSSION
Acute appendicitis is one of the most prevalent conditions necessitating surgical intervention, with a lifetime risk of developing the condition estimated to be between 6.7% and 8.6%. The preferred treatment involves early surgical removal following diagnosis. The first recorded appendectomy was carried out in 1735 by military surgeon Claudius Amyand, due to a perforated appendix with a stercoral fistula (11). In 1880, Lawson Tait performed the first appendectomy based on a correct preoperative diagnosis (12). The open appendectomy technique, employing a right gridiron incision, was introduced by McBurney in 1894 and became widely recognized for its safety and effectiveness over the decades (13).
The advent of laparoscopic appendectomy for non-inflamed appendices was first noted in 1983 by gynecologist Semm (1). Since then, numerous reports have confirmed that laparoscopic appendectomy is safe and feasible in a variety of circumstances. Its main advantages over open appendectomy include enhanced diagnostic accuracy - particularly in females where gynecologic issues can mimic acute appendicitis—superior cosmetic results, minimal tissue trauma, significantly reduced operative and postoperative complications, and a shorter recovery time.
The main limitation of this study is the relatively low number of cases in the groups examined. This suggests that future research should broaden the scope of their objectives and involve a larger patient population to enhance the reliability of the results.
The comparison of pain scores between groups reveals a strong correlation between operating time and postoperative pain levels. By considering Single Incision Laparoscopic Surgery (SILS) as a new routine technique for our surgical team, we found that excluding the first five SILS cases, which had longer operating times, led to significantly comparable post-operative pain scores and operative times. Additionally, our findings indicated no increase in surgical complications associated with the SILS method. From this refined comparison, we can draw two key conclusions. First, the transition to SILS as a new technique presents a steep learning curve for the surgical team, but adaptation can minimize the risk of surgical complications during this period. Second, MPL should be the preferred approach for patients with pre-operative conditions that favor shorter operative times during this adaptation phase.
Single-incision laparoscopic surgery (SILS), also referred to as laparo-endoscopic single-site surgery or single-port access surgery, represents an innovative approach in the realm of abdominal surgery. SILS was designed to reduce the invasiveness commonly associated with traditional laparoscopic techniques. The benefits of a SILS appendectomy align closely with the primary goals of minimally invasive surgery (MIS) appendectomy, including decreased surgical trauma, superior cosmetic outcomes, and enhanced patient satisfaction.
CONCLUSION
This study demonstrates the anticipated advantages of Single Incision Laparoscopic Surgery (SILS) over the conventional Multi-Port Laparoscopy (MPL) method through a statistical analysis of the results. Additionally, the pronounced steepness of the learning curve has been highlighted. As anticipated, during the surgical team's learning phase, SILS procedures typically require more time. Therefore, patients with co-morbidities that necessitate a shorter operative duration are more suitable candidates for MPL or open surgery during the initial adaptation period of the surgical team.
Conflict of Interest
All authors declare that they have no conflicts of interest.
Funding
The authors did not receive any financial support for the research, authorship, or publication of this article.
REFERENCES
-
Semm K. Endoscopic Appendectomy. Endoscopy. 1983;15(2): 59-64.
-
Lin YM, Hsieh CH, Cheng CI, Tan BL, Liu HT. Laparoscopic appendectomy for complicated acute appendicitis does not result in increased surgical complications. Asian J Surg. 2012;35(3):113-6.
-
Barbaros U, Dinççag A. Single incision laparoscopic splenectomy: the first two cases. J Gastrointest Surg. 2009;13(8):1520-3.
-
Castellucci SA, Curcillo PG, Ginsberg PC, Saba SC, Jaffe JS, Harmon JD. Single port access adrenalectomy. J Endourol. 2008;22(8): 1573-6.
-
Vilallonga R, Barbaros U, Sümer A, Demirel T, Fort JM, González O, et al. Single-port transumbilical laparoscopic cholecystectomy: A prospective randomised comparison of clinical results of 140 cases. J Minim Access Surg. 2012;8(3):74–8.
-
Dutta S. Early experience with single incision laparoscopic surgery: eliminating the scar from abdominal operations. J Pediatr Surg. 2009;44(9):1741-5.
-
Malik AM. The Laparoscopic Appendectomy – A Recent Trend. Advances in Laparoscopic Surgery. Available from: www.intechopen.com
-
Wewers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health. 1990; 13(4):227–36.
-
Jones MW, Lopez RA, Deppen JG. Appendicitis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Feb 26].
-
Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132(5):910–25.
-
Amyand C. VIII. Of an inguinal rupture, with a pin in the appendix coeci, incrusted with stone; and some observations on wounds in the guts. Philosophical Transactions. 1997;39(443):329–42.
-
Seal A. Appendicitis: a historical review. Can J Surg. 1981;24(4): 427–33.
-
Herrod PJJ, Kwok AT, Lobo DN. Three Centuries of Appendicectomy. World J Surg. 2023;47(4):928–36.
Full Text Sources:
Abstract:
Views: 4650

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.