Surgery, Gastroenterology and Oncology

|
|
Metastasis is a clinical manifestation of a malignant pathology and it is estimated that only 10% has a cutaneous presentation, which umbilical manifestation reduces to a 1-3%. One of its rarest kind being the Sister Mary Joseph nodule which typically presents by a palpable mass at the level of the umbilical scar, usually associated with advanced pathologies making it useful for clinical guidance and prognostic.
INTRODUCTION
Umbilical metastasis is a clinical manifestatiIon associated to advanced stage tumors, by being identified we can estimate a survival rate from 2 to 11 months for patients (1). It was described for the first time in 1864 (2), but it was not until Sir Hamilton Bailey granted it its eponym in honor of Sister Mary Joseph (1956-1939) who served as surgical assistant to Dr. William James Mayo who identified the umbilical nodules as a manifestation of patients with intrabdominal malignancies while serving as a surgical assistant in Mayo Clinic (3,4).
This nodule is identified in 1-3% of all abdominal neoplasm, varying in size between 0.5-15 cm (5), also presenting variations in its clinical presentation and associated in different percentages to a determined primary origin, making its clinical correlation important to determine patient prognosis.
CASE REPORT
A 71-year-old men native to Sonora, Mexico with a history of chronic kidney disease, high blood pressure, tobacco use ranging since 13 years of age to the moment he arrived to the moment of his arrival to his clinical evaluation, smoking one pack of cigarettes per day (HSI 58) and with occasionally alcohol use.
This current illness began one year prior to hospitali-zation with diarrheal stools up to 30 times a day for 3 months, presenting weight loss up to 20 kg. Thirty days prior presenting nausea and vomit whit oral intolerance and the growth of an umbilical nodule. During her clinical exploration he also presented dyspnea with medium efforts, orthopnea and paroxysmal nocturne dyspnea.
Figure 1 - Umbilical nodule evidenced during physical examination, bilobed, easily prone to bleeding upon touch
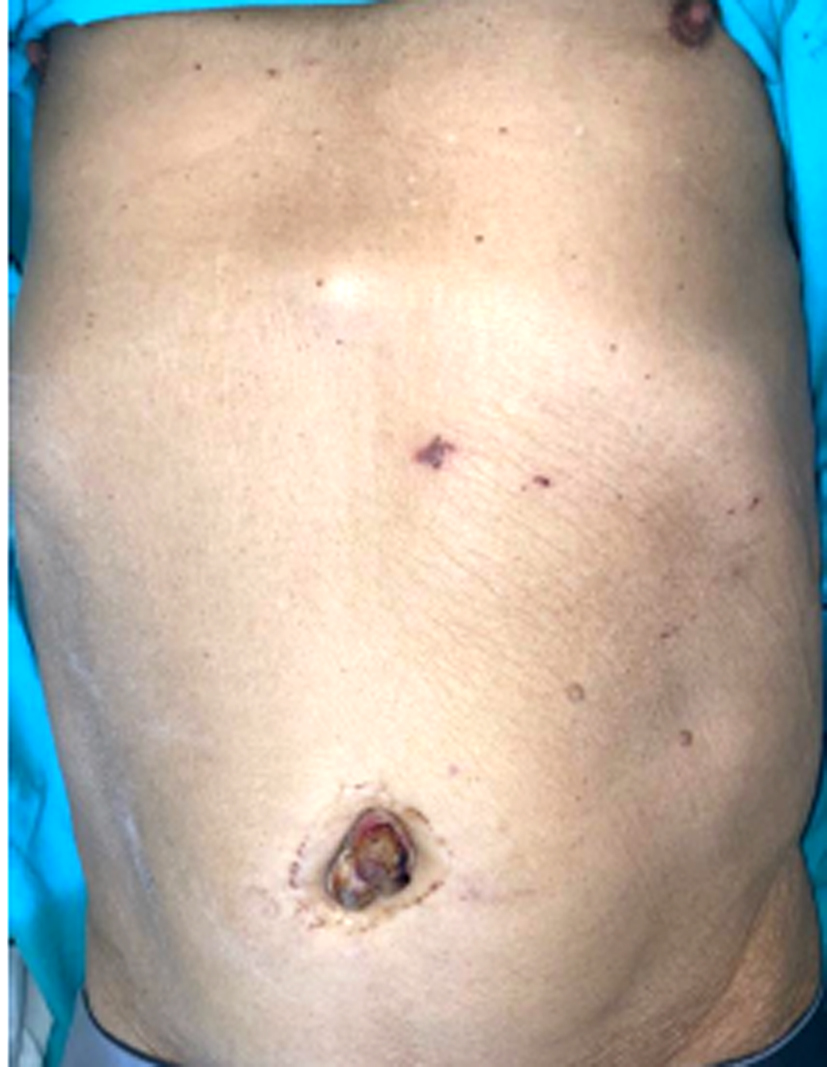
On physical patient presented extreme thinness, paleness of skin and integument. Upon abdominal examination, no visceromegaly or palpable tumors were evident, nor was any pain reported. At inspection, we observe a bilobed umbilical nodule of 4 x 3 x 2.5 cm with ulcerations and with mild pain on palpation. The nodule was apached to deep plane Gssue, easily prone to bleeding upon touch.
Investigations revealed anemia with hemoglobin of 7.4 mg/dl, creatinine of 6.2. A simple CT scan was performed since the CT scan with contrast wasn’t possible due to the elevated creatinine.
Figure 2 - Simple computed tomography revealing abundant intraabdominal lymph node chains and an umbilical nodule (a, b)
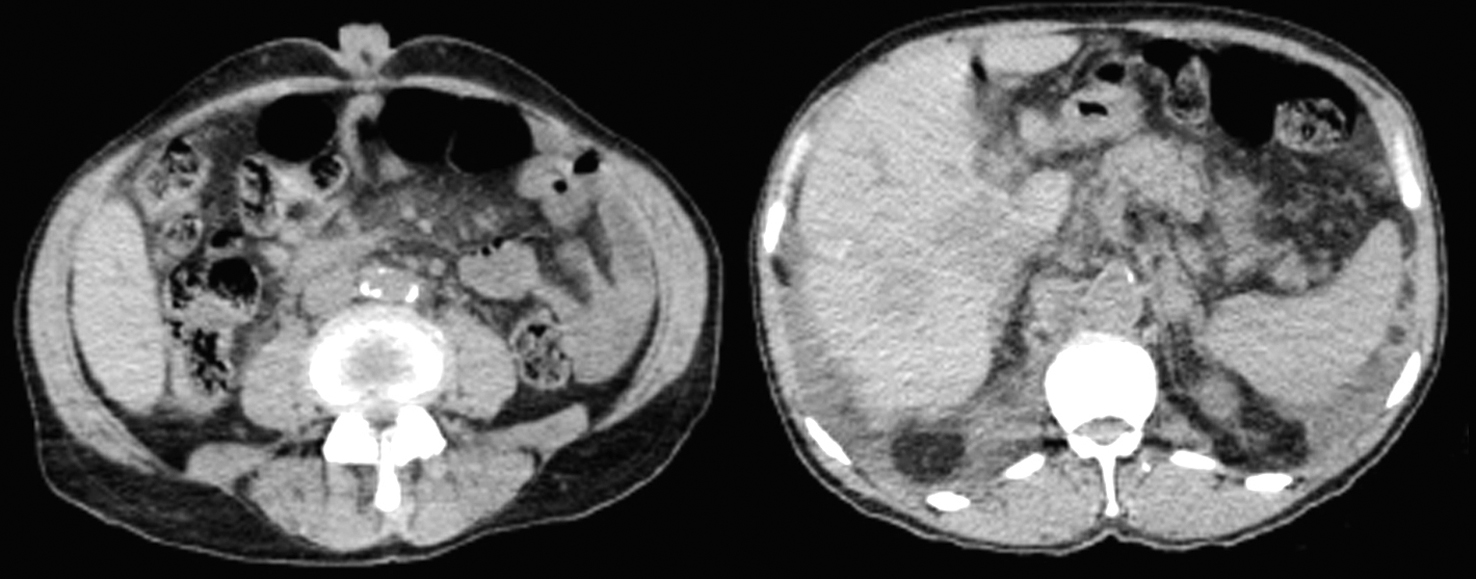
The CT scan revealed atypical lymphatic activity at abdominal, retroperitoneal, supraclavicular, mediastinal, mesenteric, peripancreatic level which is associated to hepatic density changes of infiltrative appearance, considered secondary to neoplastic activity. Presence of nonspecific morphologic changes of the pancreatic head with the possibility of primary activity being at this level. Bilateral pleural effusion of a 40% and pericardial effusion. Centrilobular emphysema type COPD, cholelithiasis, bilateral renal hypertrophy data but there is no mention of the umbilical nodule.
Ganglion cytology revealed adenocarcinoma moderately differentiated whith intestinal phenotype, immunohistochemistry reported negative for CK7 and positive for CK20, CK19, CDX2, SATB2, and ACE, indicating, based on the guidelines of the European Society for Medical Oncology (ESMO), a probable colorectal or Meckel cell origin.
The patient passed away one month ater diagnosis, at the onset of chemotherapy treatment, due to disease progression.
DISCUSSION
Sister Maria Jose's nodule, within its macroscopic characteristics, has been described in various articles as a mass located at the level of the umbilical scar with irregular borders, changes in coloration, bleeding, discharge of exudate, either serous or sanguineous, and ulcerations, predominantly identified in the female gender6. The umbilical lesion often preceed the primary diagnosis of cancer, serving as the initial presentation of malignancy, as is the case with our patient.
Regarding the causes of metastatic spread to this area, it has been suggested that the main cause is due to connections of lymphatics specifically with the axillary and inguinal lymph nodes (7). Also mentioned is the venous drainage of the abdominal wall or contiguous extension (8).
Histopathologically, the most common variant identified is adenocarcinoma (80%), showing variation in the primary origin of cancer according to gender, primarily located in the stomach in men (26%) and ovaries in women (20%), with smaller amounts in the colon, rectum, anus, and uterus. However, many umbilical metastases do not have an identified origin.
Among the differential diagnoses are various benign pathologies such as umbilical hernia, granuloma, epidermoid cysts, umbilical endometriosis, pyoderma gangrenosum, and omphalitis, which must be related through medical history (9,10). However, when there is suspicion, a directed medical history should be conducted to identify symptoms that can more precisely guide towards a diagnosis, identifying those patients who will require referral to a higher level of care for further evaluation and management.
In managing patients, a biopsy of the nodule can support a histological diagnosis along with immuno-histochemistry. Contrast-enhanced CT scans or MRIs can help identify the extent and probable primary origin of the disease. The prognosis for patients presenting with Sister Maria Jose's nodule is usually unfavorable, often leading to palliative care, considering that the survival of our patient post-identification of the umbilical lesion was two months.
CONCLUSION
Sister Maria Jose's nodule is a finding in physical examination that points towards the presence of advanced intra-abdominal neoplasms, indicating a poor prognosis upon presentation.
Therefore, timely diagnosis will allow for the initiation of appropriate management to potentially improve the patient's survival.
Conflicts of interest and source funding
The article did not receive funding and authors declare that they have no conflicts of interest.
REFERENCES
- Chalya Rambau PF, McHembe MD, Mabula JB. Sister Mary Joseph’s nodule at a University teaching hospital in northwestern Tanzania: a retros-pective review of 34 cases. World J Surg Oncol. 2013;11:151.
- Quenu l. Secondary cancer in the umbilicus. Rev chir 1896;16: 97-133.
- Bailey h. Demonstrations of physical signs in clinical surgery, 13th edit. Baltimore: Williams & Wilkins; 1960, p. 356.
- Mayo wj. Metastasis in cancer. Proceedings of the staff meetings of the Mayo Clinic. 1928;3:327.
- Tso S, Brockley J, Recica H, Ilchyshyn A. Sister Mary Joseph's nodule: an unusual but important physical finding characteristic of widespread internal malignancy. Br J Gen Pract. 2013;63(615):551-2.
- Dubreuil A, Dompmartin A, Barjot P, Louvet S, Leroy D. Umbilical metastasis or Sister Mary Joseph's nodule. Int J Dermatol. 1998; 37(1):7-13.
- Chakraborty AK, Reddy AN, Grosberg SJ, Wapnick S. Pancreatic carcinoma with dissemination to umbilicus and skin. Arch Dermatol. 1977;113(6):838-9.
- Goodheart RS, Cooke CT, Tan E, Matz LR. Sister Mary Joseph's nodule. Med J Aust. 1986;145(9):477-8.
- Schnipper EF, Nissenblatt MJ, Schwartz M, Ludwig SL. Sister Mary Joseph Node-a clue to internal malignancy. J Med Soc N J. 1981; 78(6):453-4.
- Scarpa FJ, Dineen JP, Boltax RS. Visceral neoplasia presenting at the umbilicus. J Surg Oncol. 1979;11(4):351-9.
Full Text Sources:
Abstract:
Views: 4606

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.