Surgery, Gastroenterology and Oncology
Background: Hemorrhoidal disease is one of the most common anorectal conditions, significantly affecting quality of life. Current treatment trends are shifting toward minimally invasive techniques that preserve supporting tissues, reduce postoperative pain, and shorten recovery. Laser hemorrhoidoplasty (LHP) uses laser energy to vaporize, coagulate vessels, induce fibrosis, and reduce hemorrhoidal volume without excision. However, large-scale evidence on its efficacy and safety remains limited. Objectives: To evaluate the efficacy and safety of LHP, analyze factors affecting outcomes, and assess the role of TND’s vertical ligation mucopexy (TVLM) combined with LHP.
Methods: A retrospective descriptive study was conducted on 1,277 patients undergoing LHP at the Department of Colorectal and Pelvic Floor Surgery from September 2023 to February 2026.
Results: Mean age was 45.55 ± 13.97 years; 53.2% were male; grade III hemorrhoids accounted for 59.5%. TVLM was performed in 58.7% of cases. Mean operative time was 35.05 ± 10.15 minutes; hospital stay was 1.27 ± 0.90 days. The mean number of treated piles was 3.54 ± 0.68, with energy of 273.5 ± 102.8 J/pile. Mean VAS decreased from 2.96 ± 0.29 (day 1) to 1.17 ± 0.41 (discharge) and 0.18 ± 0.54 (2 weeks). Intraoperative com-plications included bleeding (2.0%), mucosal perforation (0.9%), and burn (0.9%). Postoperative complications included bleeding (6.89%), urinary retention (2.5%), defecatory disorders (3.8%), thrombosis (0.3%), anal inflammation (11.5%), abscess (0.23%), and sepsis (0.1%). Recurrence was 1.4% at 10.69 months; reoperation 0.2%; readmission 3.5%. TVLM + LHP showed improved outcomes in complex cases.
Conclusions: LHP is a safe, effective, minimally invasive technique with low pain, rapid recovery, and low complication rates. A stratified approach combining LHP with TVLM may represent a modern treatment trend.
INTRODUCTION
Hemorrhoidal disease is one of the most common benign anorectal conditions, significantly affecting patients’ quality of life. Epidemiological studies have reported a prevalence ranging from 16.6% to 34.7% in the general population, particularly among individuals with sedentary lifestyles and low-fiber diets (1,2). In recent years, the management of hemorrhoidal disease has shifted markedly toward minimally invasive and tissue-preserving approaches, aiming to reduce postoperative pain, shorten recovery time, and main-tain anorectal physiological function. In this context, Laser Hemorrhoidoplasty (LHP) has been widely adopted due to its minimally invasive nature, ability to shorten recovery time, and reduce postoperative complications (3,4). However, the effectiveness of LHP alone remains limited in advanced hemorrhoids or in cases associated with rectal mucosal prolapse, with potential risks of persistent symptoms, complications, or recurrence (5). Recently, a stratified treatment approach combining minimally invasive techniques has gained attention as a personalized strategy. In particular, the combination of LHP with TND’s Vertical Ligation–Mucopexy (TVLM) within a multimodal treatment framework has shown potential to improve postoperative outcomes, especially in patients with complex or advanced hemorrhoidal disease. This approach not only addresses both hemorrhoidal tissue and mucosal prolapse simultaneously but also optimizes treatment efficacy while preserving the advantages of LHP. Nevertheless, current evidence regarding the efficacy and safety of this strategy - especially in large cohorts with long-term follow-up - remains limited. Moreover, factors influencing treatment outcomes in real-world clinical practice have not been fully elucidated. Therefore, this study was conducted to evaluate the efficacy and safety of LHP in the treatment of hemorrhoidal disease, as well as to analyze the role of TVLM when combined with LHP in a stratified, multimodal treatment strategy. Additionally, the study aims to identify factors associated with post-operative outcomes at Hanoi Medical University Hospital.
MATERIAL AND METHODS
Study Population
Patients diagnosed with hemorrhoidal disease who underwent LHP at Hanoi Medical University Hospital from September 2023 to February 2026.
Inclusion criteria:
• Patients diagnosed with hemorrhoidal disease with an indication for surgery.
• Underwent LHP alone or in combination with TVLM, MMH, or FH.
• Complete medical records with sufficient post-operative follow-up data.
Exclusion criteria:
• Incomplete medical records or missing post-operative follow-up data.
Study Design
A retrospective descriptive study including all patients diagnosed with hemorrhoidal disease and treated with LHP at Hanoi Medical University Hospital from September 2023 to February 2026.
Convenience sampling was applied, including all eligible patients during the study period.
Data Collection and Analysis
Data were collected from medical records, including demographic characteristics, clinical features, treatment outcomes, and postoperative complications. Data were entered and analyzed using SPSS version 20.0. Quantitative variables were expressed as mean ± standard deviation, and qualitative variables as frequencies and percentages.
Stratified Lesion Approach and Surgical Strategy
Based on the biomechanical theory combined with vascular factors in the pathogenesis of hemorrhoidal disease, rectal mucosal prolapse often coexists at varying degrees, resulting in diverse clinical presentations. To simplify clinical practice, especially when applying minimally invasive and tissue-preserving techniques, hemorrhoidal disease associated with rectal mucosal prolapse was stratified as follows:
• Layer 1: Rectal mucosal prolapse of varying degrees (Grade I–III).
• Layer 2: Internal hemorrhoidal prolapse with varying grades and morphologies, located above the dentate line.
• Layer 3: External hemorrhoidal prolapse and perianal skin tags with varying degrees and morphologies, located below the dentate line.
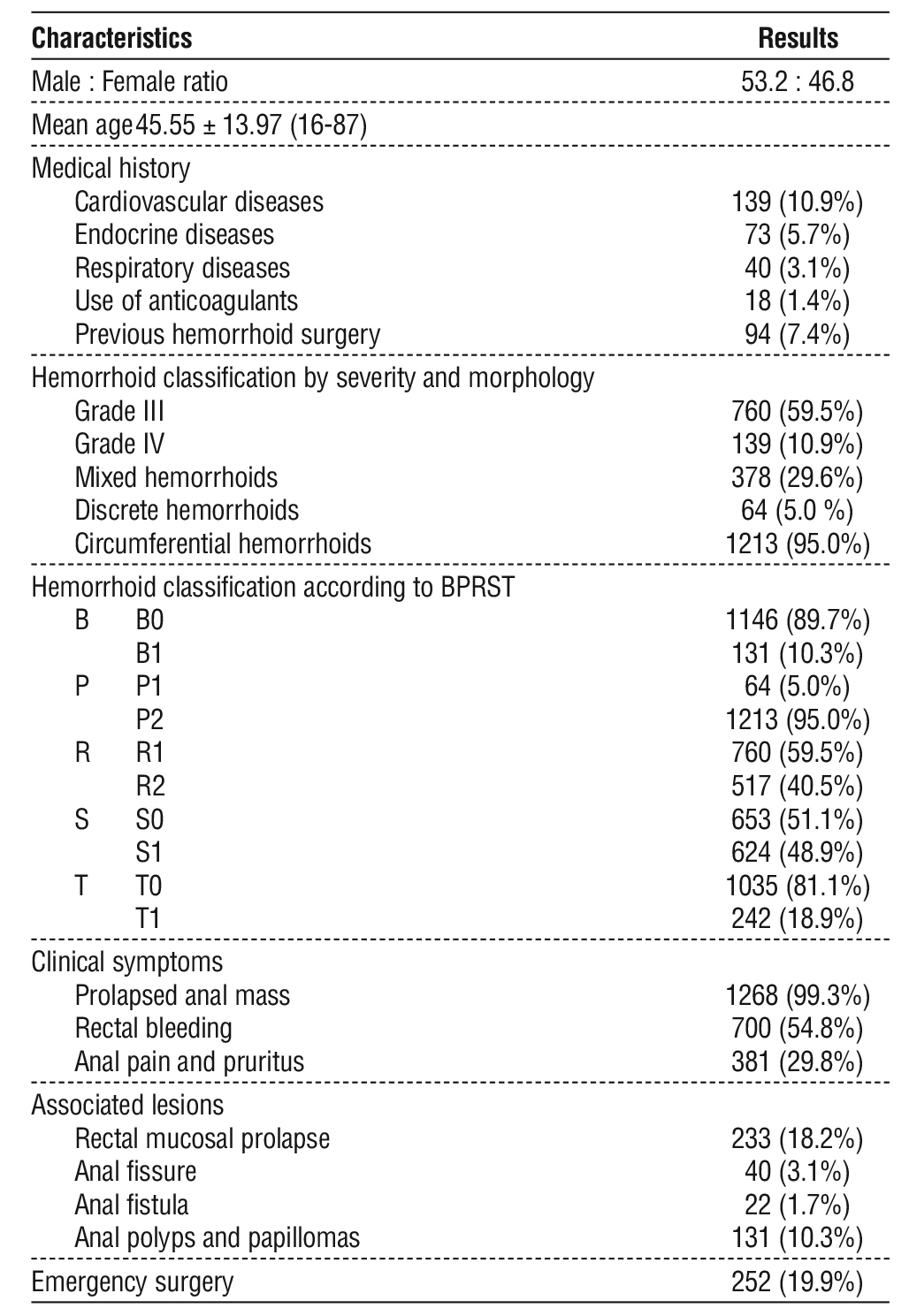
Table 1 - General characteristics of the study population
Based on this stratification model, the surgical strategy was tailored for each layer to optimize outcomes and preserve anorectal function:
• Layer 1: TVLM was performed to address rectal mucosal prolapse (if present) and restore the supporting axis (6).
• Layer 2: LHP was used for grade II–III hemorrhoids, while LHP + TVLM was indicated for grade IV hemorrhoids or grade III hemorrhoids with bleeding.
• Layer 3: LHP combined with excision of perianal skin tags when indicated, to improve symptoms and cosmetic outcomes.
Note: LHP + TVLM was mainly indicated for mixed hemorrhoids, grade IV hemorrhoids, grade III hemorrhoids with bleeding, and cases associated with rectal mucosal prolapse.
This approach allows individualized treatment based on lesion severity while maximizing the advantages of each technique in a multimodal strategy.
Ethics
This study was conducted using retrospective data from medical records and did not interfere with patient management. All personal information was kept confidential and used solely for research purposes. The study adhered to ethical principles for biomedical research in accordance with the Declaration of Helsinki and its subsequent amendments.
RESULTS
Characteristics of the Study Population (table 1)
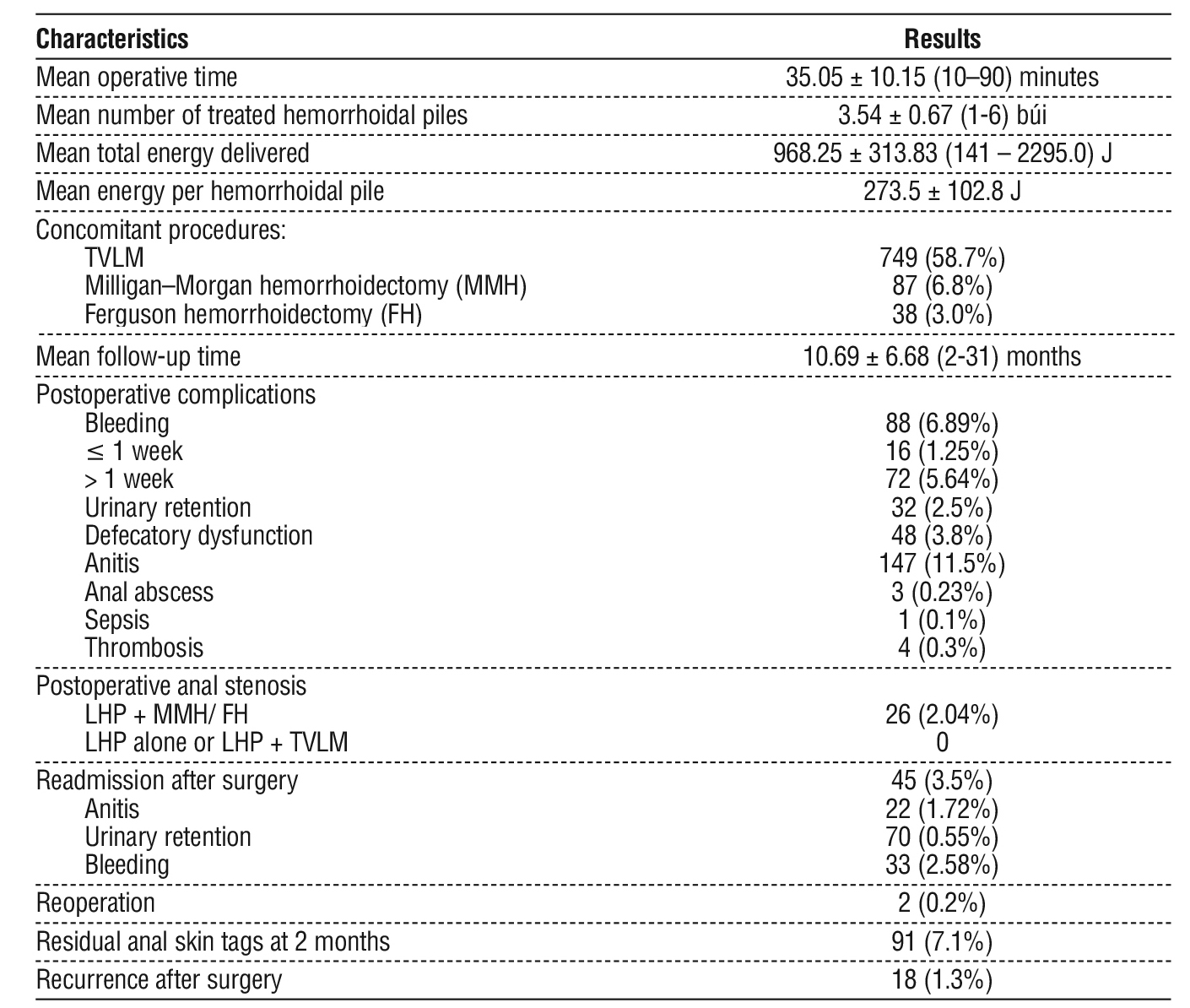
Intraoperative and Postoperative Characteristics (table 2)
Table 2 - Intraoperative and postoperative characteristics
Stratification of lesions and treatment orientation (table 3)
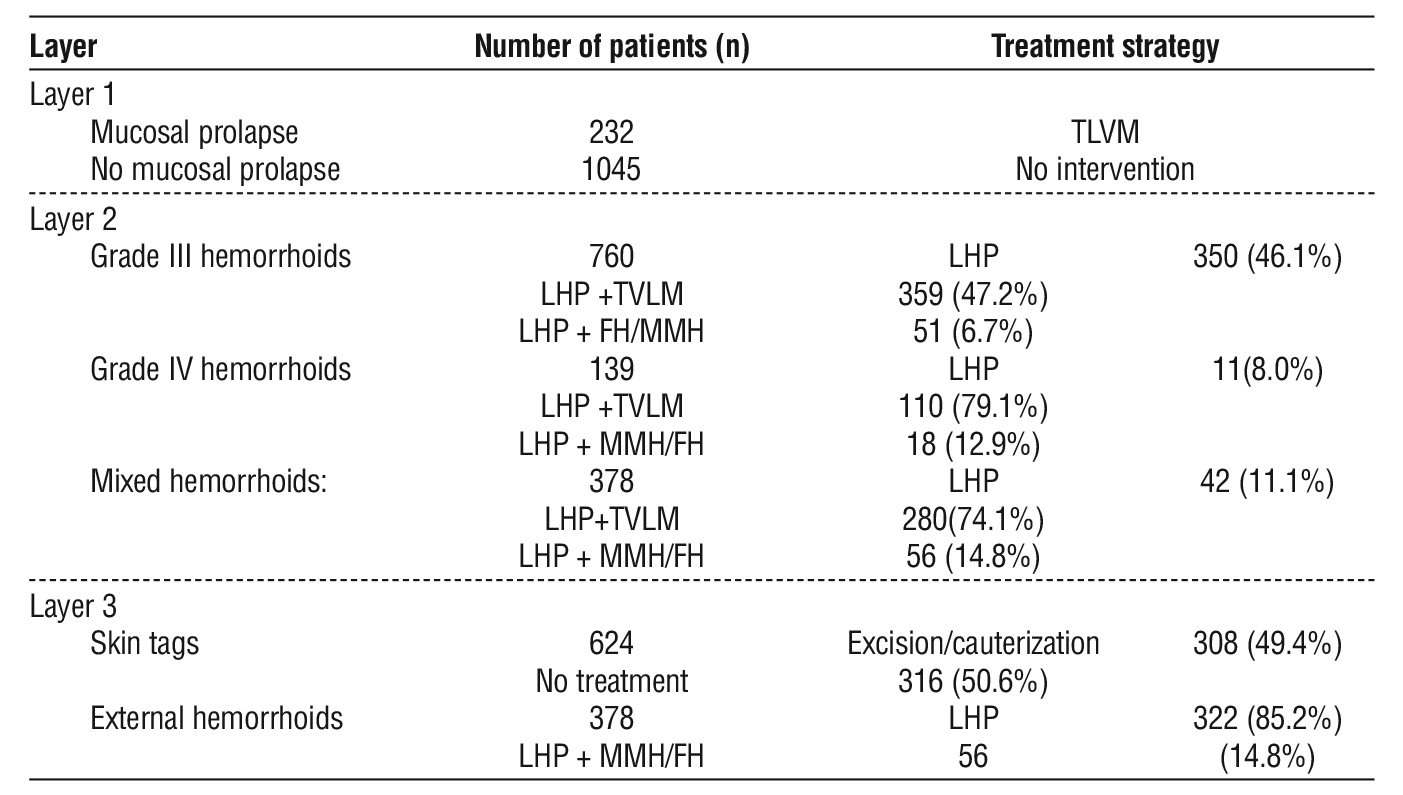
Table 3 - Lesion stratification and treatment strategies in the study population
Factors associated with postoperative outcomes (tables 4-8)
Table 4 - Multivariable regression analysis of factors associated with postoperative pain (VAS on day 1)
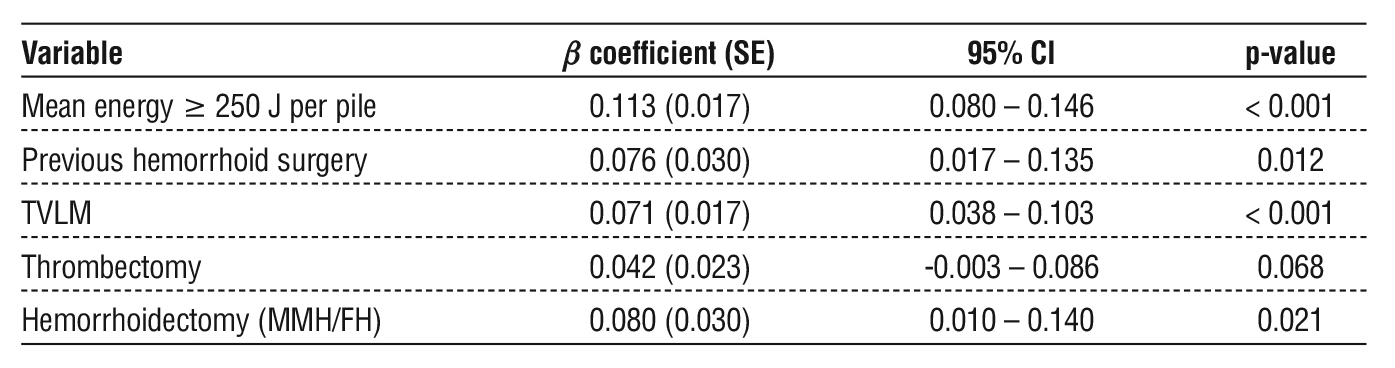
Table 5 - Multivariable regression analysis of factors associated with postoperative bleeding
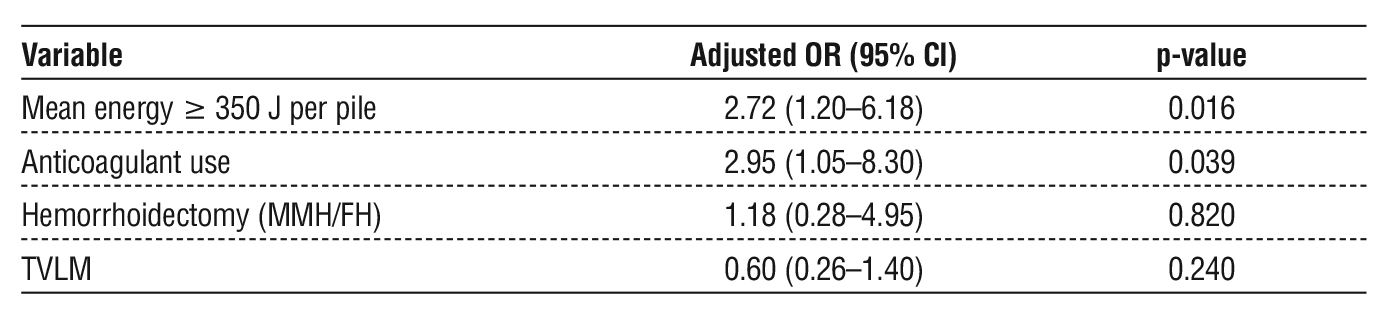
Table 6 - Multivariable regression analysis of factors associated with postoperative anitis
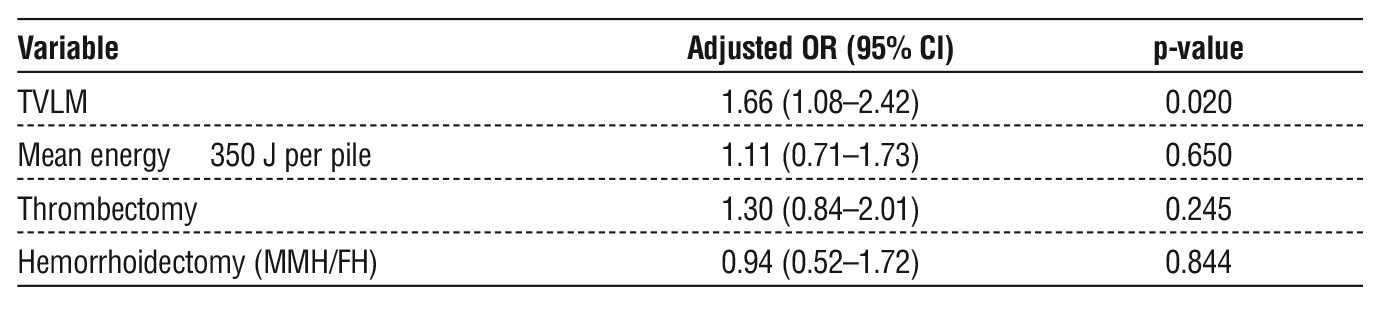
Table 7 - Multivariable regression analysis of factors associated with postoperative urinary retention
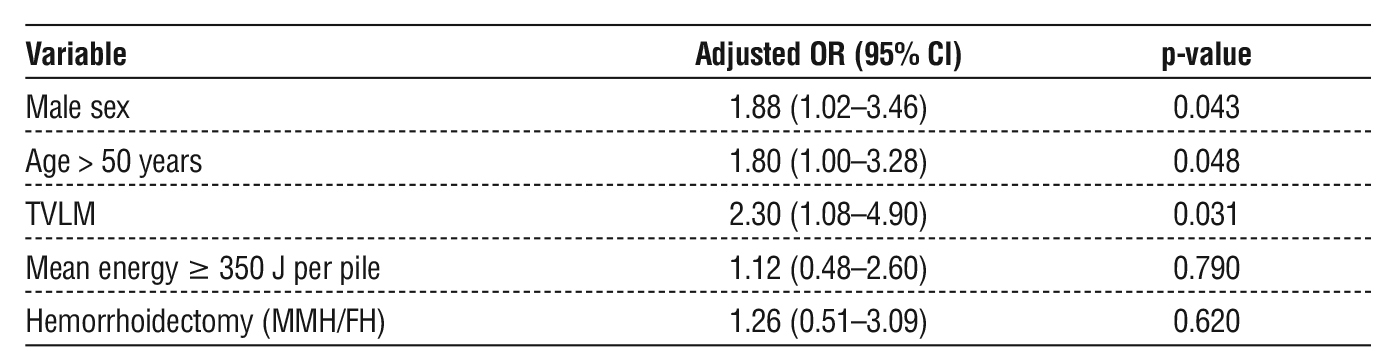
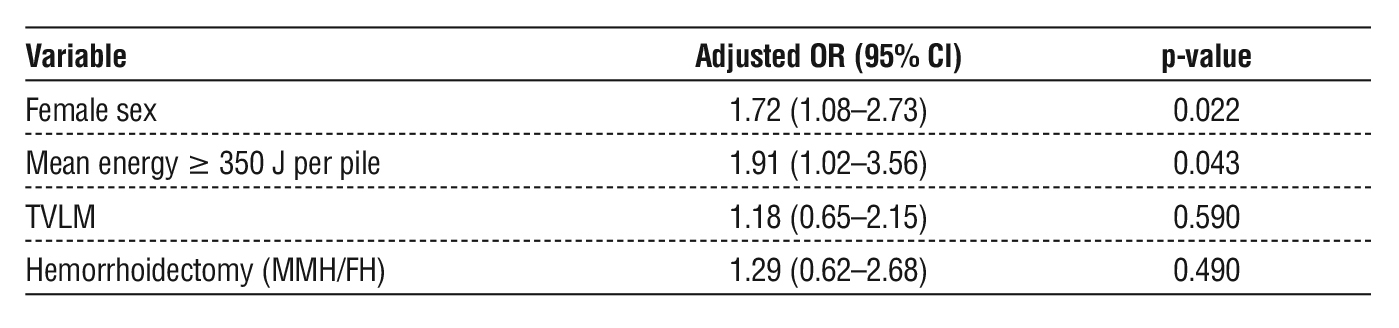
Table 8 - Multivariable regression analysis of factors associated with postoperative defecatory dysfunction
DISCUSSION
General Characteristics of the Study Population
In our study, the mean age of patients was 45.55 ± 13.97 years, which is consistent with the epidemiological characteristics of hemorrhoidal disease. Johanson and Sonnenberg, in a large epidemiological study involving 10 million individuals in the United States, reported that the highest prevalence occurred in the 45–65 age group (7). The maletofemale ratio in our study was relatively balanced (53.2% vs. 46.8%). This finding is consistent with several recent epidemiological studies that reported no significant gender differences in hemorrhoidal disease (8). These results suggest that hemorrhoidal disease affects both sexes similarly, in contrast to earlier assumptions that it predominates in males. This shift may be attributed to modern lifestyle factors, where both men and women are exposed to similar risks, including lowfiber diets, physical inactivity, prolonged sitting, and occupational stress. Furthermore, in women, specific factors such as pregnancy, childbirth, and hormonal changes may increase the risk of disease, thereby reducing gender disparities observed in recent studies.
Regarding comorbidities, a considerable proportion of patients had underlying chronic conditions, including cardiovascular diseases (10.9%), endocrine disorders (5.7%), and respiratory diseases (3.1%). Additionally, 1.4% of patients were receiving anticoagulant therapy. Notably, despite these risk factors, patients were safely treated with laser surgery and achieved favorable outcomes, demonstrating the feasibility and safety of this technique in patients with comorbidities. With respect to surgical history, 94 patients (7.4%) had undergone previous hemorrhoid surgery, among whom stapled hemorrhoidopexy (Longo procedure) accounted for 46 cases (48.9%). In this subgroup, most patients
presented with postoperative anal stenosis, which caused defecatory difficulty and negatively impacted quality of life. Therefore, the selection of LHP was considered appropriate, as it minimizes the risk of exacerbating stenosis while maintaining therapeutic efficacy. In terms of clinical presentation, prolapsed anal mass was the most common symptom (99.3%), followed by rectal bleeding (54.8%) and anal pain or pruritus (29.8%). According to severity classification, grade III hemorrhoids accounted for 59.5%, grade IV for 10.9%, and mixed hemorrhoids for 29.6%, with circumferential hemorrhoids representing 95.0% of cases. Associated lesions were relatively diverse. The most common were rectal mucosal prolapse (18.2%) and anal polyps/papillomas (10.3%), followed by anal fissure (3.1%) and anal fistula (1.7%). These conditions often required concomitant management during the same surgical session. Additionally, the rate of emergency surgery was 19.9%, mainly in cases of thrombosed hemorrhoids or active bleeding. Nevertheless, laser treatment remained safe and effective in this subgroup of patients.
Intraoperative and Postoperative Characteristics and Factors Affecting Postoperative Outcomes
Based on the analysis of the first 262 cases, we found that the effectiveness of Laser Hemorrhoidoplasty (LHP) is closely associated with lesion characteristics, particularly the degree of mucosal prolapse (6). Since laser-induced fibrosis requires several weeks to achieve full therapeutic effect and daily postoperative care is not always feasible in Vietnam, LHP alone may be insufficient in advanced hemorrhoids or cases associated with rectal mucosal prolapse, leading to persistent symptoms or recurrence. Therefore, we developed and applied a lesion stratification strategy to guide the selection of appropriate surgical techniques for each patient group.
Layer 1: All 232 patients with rectal mucosal prolapse (including 121 cases of grade III hemorrhoids, 41 cases of grade IV hemorrhoids, and 80 cases of mixed hemorrhoids) were treated with TVLM.
Layer 2: Treatment strategies were individualized according to disease severity. Among patients with grade III hemorrhoids (n = 760), LHP alone was performed in 350 cases (46.1%), while 359 cases (47.2%) underwent LHP combined with TVLM (including 111 cases with mucosal prolapse and 242 cases with bleeding or congested hemorrhoids), and 51 cases (6.7%) underwent LHP combined with MMH/FH. In patients with grade IV hemorrhoids (n = 139), most were treated with LHP + TVLM (79.1%), followed by LHP + MMH/FH (12.9%) and LHP alone (8.0%). Similarly, in mixed hemorrhoids (n = 378), LHP + TVLM was the predominant approach (74.1%), followed by LHP alone (11.1%) and LHP + MMH/FH (14.8%).
Layer 3: A total of 378 external hemorrhoids were treated, including 304 cases managed with LHP (19 bleeding, 125 thrombosed), 59 cases treated with MMH (37 bleeding, 22 thrombosed), and 15 cases treated with FH (3 bleeding, 12 thrombosed). Additionally, 624 patients presented with anal skin tags, of which 308 cases (49.4%) underwent excision or cauterization.
Other procedures were performed depending on lesion characteristics, including polypectomy or papilloma excision and fistulotomy in 22 cases (1.7%). The mean operative time for LHP was 35.05 ± 10.15 minutes. LHP alone had a shorter operative time (30.04 ± 8.98 minutes), compared to LHP + TVLM (36.87 ± 10.45 minutes) and LHP + FH/MMH (39.13 ± 10.37 minutes), with a statistically significant difference (p < 0.001). The mean hospital stay was 1.27 ± 0.89 days. In the study by Islam et al. (2024), the mean operative time was 14.70 ± 4.70 minutes and the mean hospital stay was 1.01 ± 0.24 days, suggesting that LHP is a daycase procedure with rapid recovery (9). The difference in operative time between our study and that of Islam et al. (2024) may be explained by differences in patient characteristics. While our study included 100% of patients with grade III–IV hemorrhoids and diverse associated lesions, the Bangladesh study included patients with grade II hemorrhoids.
Regarding intraoperative complications, our study recorded bleeding in 26 cases (2.0%), mucosal burns in 12 cases (0.9%), and mucosal perforation in 12 cases (0.9%). Notably, these complications primarily occurred during the early phase of technique implementation, within approximately the first 50 cases, before overcoming the learning curve (10). Intraoperative complications were mainly related to technical factors, with three common errors identified: (1) laser application too close to the mucosal surface, resulting in mucosal burns; (2) inadequate control of hand force during fiber insertion, leading to penetration of the rectal mucosa; and (3) insertion of the needle too deeply into the muscular layer, causing injury to submucosal vessels and intraoperative bleeding.
Regarding postoperative pain in our study, the mean VAS score on postoperative day 1 was 2.96 ± 0.29, decreasing to 1.17 ± 0.41 at discharge. The group undergoing LHP combined with TVLM had a mean VAS score of 2.99 ± 0.10 on postoperative day 1 compared to 2.93 ± 0.14 in the nonTVLM group, with no statistically significant difference (p > 0.05). These findings are comparable to those reported by Tolksdorf et al. (2022), who applied radiofrequency ablation (RFA) and reported a mean VAS score of 2.5 ± 2.7 immediately after the procedure, with approximately 60% of patients not requiring analgesics (11). Our results were lower than those reported by Tran Ngoc Dung (2025), in which patients undergoing TVLM had a postoperative day 1 VAS score of 3.23 ± 1.03, and also lower than those reported by Khanna (2010), who documented postoperative VAS scores of 6.8 ± 1.8 for Ferguson hemorrhoidectomy (FH) and 4.1 ± 0.8 for Milligan– Morgan or Ligasure hemorrhoidectomy (MMH/LH) (p < 0.001) (6,12). Multivariable regression analysis identified several independent factors associated with postoperative pain on day 1. Mean laser energy ≥ 250 J per pile was the most influential factor (β = 0.113; p < 0.001), followed by previous hemorrhoid surgery (β = 0.076; p = 0.012) and hemorrhoidectomy procedures (MMH/FH) (β = 0.080; p = 0.021). TVLM was also associated with a slight increase in VAS score (β = 0.071; p < 0.001); however, the magnitude of this effect was smaller and not clinically significant. In contrast, thrombectomy did not show statistical significance (p = 0.068). At 2 weeks, the mean VAS score decreased to 0.18 ± 0.54, with 14.2% of patients reporting mild residual pain. Ghani et al. (2025), in a study on patients undergoing LHP, reported that 90% of patients were painfree after 6 weeks, demonstrating the early and sustained analgesic effect of this technique (13) Conversely, conventional surgical techniques are typically associated with a significantly longer duration of postoperative pain. In the study by Fang et al. (2018), the mean duration of postoperative pain was 19.65 days following Milligan–Morgan hemorrhoidectomy (MMH) and 16.36 days following stapled hemorrhoidopexy (PPH) (14).
Regarding postoperative complications in our study, the overall rates were low, and most cases could be managed conservatively. Bleeding was the most common complication, occurring in 88 cases (6.89%), with the majority being delayed bleeding after 1 week (5.64%) compared to early bleeding (1.25%). Among these, 33 patients (2.58%) required readmission for monitoring, and 2 cases required blood transfusion; however, no cases required reoperation. These findings suggest that although bleeding is a relatively common complication, it is generally mild and can be effectively managed with medical treatment. Multi-variable regression analysis identified two independent risk factors associated with an increased risk of post-operative bleeding: mean laser energy ≥ 350 J per pile (OR = 2.72; 95% CI: 1.20–6.18; p = 0.016) and the use of anticoagulants (OR = 2.95; 95% CI: 1.05–8.30; p = 0.039). These results indicate that higher energy levels may increase the risk of mucosal injury and delayed necrosis, while systemic factors such as anticoagulant use directly affect hemostasis. In contrast, combined procedures such as hemorrhoidectomy (MMH/FH) (p = 0.820) and TVLM (p = 0.240) were not associated with a statistically significant increase in bleeding risk. Regarding postoperative anitis, this was a relatively common complication (11.5%) but was mostly mild and responded well to conservative treatment. In our study, 22 cases (1.72%) required readmission for treatment. The management protocol primarily included topical antiinflammatory agents and analgesics, combined with supportive therapies such as plasma application to promote mucosal healing and reduce inflammatory response. Multivariable regression analysis showed that TVLM was an independent factor associated with an increased risk of postoperative anitis (OR = 1.61; 95% CI: 1.08–2.42; p = 0.020), while other factors such as mean laser energy ≥ 350 J per pile, thrombectomy, and combined hemorrhoidectomy (MMH/FH) were not significantly associated. Regarding postoperative urinary retention, the incidence in our study was 2.5%, occurring mainly in the early post-operative period and resolving rapidly. Compared with other surgical techniques, our findings also demonstrate the advantage of minimally invasive approaches. Qing Long (2025) reported a postoperative urinary retention rate of up to 12.6% in patients undergoing MMH, while other studies on FH and conventional hemorrhoidectomy techniques have reported rates ranging from 10% to 30% (15). Multivariable regression analysis identified several independent factors associated with postoperative urinary retention. Specifically, male sex (OR = 1.88; p = 0.043), age > 50 years (OR = 1.80; p = 0.048), and the use of TVLM (OR = 2.30; p = 0.031) were associated with an increased risk. In contrast, mean laser energy ≥ 350 J per pile, thrombectomy, and combined hemorrhoidectomy procedures (MMH/FH) were not significantly associated (p > 0.05). These findings are consistent with those of Qing Long et al. (2025), who suggested that postoperative urinary retention may be related to spinal anesthesia causing inhibition of sacral nerve roots (S2– S4), postoperative pain leading to urethral sphincter spasm, agerelated decline in bladder function, male sex or prostate enlargement causing urinary outflow obstruction, and excessive intraoperative fluid administration increasing bladder pressure (15). Regarding postoperative defecatory dysfunction, the incidence was 3.8%, primarily presenting as difficulty in defecation during the early postoperative period. Most cases were mild and responded well to conservative management, including dietary modification with increased fiber intake, use of stool softeners, and guidance on appropriate bowel habits. Multivariable regression analysis showed that postoperative defecatory dysfunction was independently associated with female sex (OR = 1.72; 95% CI: 1.08–2.73; p = 0.022) and mean laser energy ≥ 350 J per pile (OR = 1.91; 95% CI: 1.02– 3.56; p = 0.043). In contrast, other factors such as TVLM and combined hemorrhoidectomy (MMH/FH) were not significantly associated (p > 0.05). Additionally, several relatively rare complications were observed. Anal abscess occurred in 3 cases (0.23%), all of which were successfully managed with drainage, debridement, and adjunctive plasma therapy, resulting in good recovery. Thrombosis was observed in 4 cases (0.3%), among which 2 cases required reoperation using the MMH technique, while the remaining 2 cases were managed conservatively with plasma therapy and close followup. Notably, one case of postoperative sepsis caused by Escherichia coli was recorded. The patient developed persistent high fever after surgery, with positive blood cultures for Escherichia coli, while the surgical site showed only mild local inflammation without signs of spreading infection. The patient was treated with intensive medical therapy, including antibiotics and supportive care, and achieved full recovery. Sepsis following hemorrhoid treatment is a very rare but potentially lifethreatening complication that requires prompt management. A systematic review by McCloud et al. reported 38 cases of sepsis across 29 studies, including 10 deaths. These cases occurred following various treatment modalities, including rubber band ligation, sclerotherapy, hemorrhoidectomy, and stapled hemorrhoidopexy (PPH) (16). Regarding postoperative anal stenosis, we recorded 26 cases in patients who underwent combined hemorrhoidectomy (MMH/FH) with LHP, whereas no cases were observed in patients treated with LHP alone or LHP combined with TVLM. This difference may be explained by the underlying surgical mechanisms. Conventional excisional techniques such as MMH and FH involve removal of hemorrhoidal tissue along with the rectal mucosa and anoderm, which may lead to fibrosis and scar contraction during wound healing, resulting in anal canal narrowing, particularly when mucocutaneous bridges are not adequately preserved or when closure is under tension. In contrast, LHP is a tissuepreserving technique that maintains the integrity of the anal cushions and mucosa, thereby reducing the risk of fibrosis and stenosis. In addition, TVLM has been shown not to cause anal stenosis, as its longitudinal suturing along the anal canal helps distribute tension evenly and minimizes scar contraction, as reported by Tran Ngoc Dung (2025) (6).
The mean followup duration in our study was 10.69 ± 6.68 months, with the longest followup reaching 31 months, during which the recurrence rate was 1.3%. Notably, most recurrence cases occurred among the first 256 patients treated, when the stratification strategy had not yet been consistently applied (10). These findings are consistent with the study by Islam et al. (2024), in which, although LHP provided effective pain relief and symptom improvement, additional mucopexy was required in all patients with grade IV hemorrhoids and in some cases of grade III hemorrhoids to control prolapse and reduce recurrence (9). Porwal et al., in a large study of 1,088 patients treated with LHP alone, reported a very low recurrence rate of approximately 0.55% after 2 years of followup (17). However, this difference may be explained by the characteristics of the study population, as most patients in Porwal’s study had grade II–III hemorrhoids, representing milder disease stages with less pronounced mucosal prolapse. In contrast, our study included a high proportion of patients with grade III–IV hemorrhoids, particularly those with associated rectal mucosal prolapse. Similarly, Tomas Pokus (2020) reported a significantly higher recurrence rate in patients with grade III-IV hemorrhoids treated with LHP alone. Thus, the lesion stratification strategy, particularly the combination of LHP with TVLM, appears to effectively address advanced hemorrhoids and cases associated with mucosal prolapse, thereby representing a promising approach to improving longterm treatment outcomes in clinical practice. When compared with other techniques, LHP demonstrates relatively favorable outcomes. Zhang et al. reported a recurrence rate of 8.4% at 12 months for stapled hemorrhoidopexy (PPH), while Lauricella et al. reported an increased rate of 15.7% at 24 months (18). The rate of residual anal skin tags at 2 months in our study was 7.1%. Notably, patients who underwent TVLM had a significantly lower incidence of residual anal skin tags compared to those who did not (24 vs. 67 cases, p < 0.05), highlighting the role of TVLM in improving postoperative morphology.
CONCLUSION
Laser Hemorrhoidoplasty (LHP) is a minimally invasive and safe technique that reduces postoperative pain, shortens recovery time, and provides stable shortand midterm outcomes with low complication and recurrence rates. Notably, the lesion stratification strategy, particularly the combination of LHP with TVLM, demonstrated superior outcomes compared to LHP alone by overcoming its inherent limitations. This comprehensive approach enables a more effective management of hemorrhoidal disease and represents a promising trend in current clinical practice.
Authorship
All authors made substantial contributions to one or more critical aspects of the study (conceptualization and design; data acquisition, analysis, or interpretation; drafting the manuscript or critical scholarly revision), approved the final version, and agree to be accountable for all aspects of the work. All authors confirm that they meet the ICMJE authorship criteria.
Acknowledgements
We gratefully thank Hanoi Medical University Hospital and our colleagues at the Department of Coloproctology and Pelvic Floor Surgery for their support throughout the study.
Competing Interests
The authors declare no competing interests.
Funding
This research received no external funding.
Ethical Approval
This study is a retrospective analysis of fully anonymized data extracted from electronic medical records. Under the regulations of Hanoi Medical University Hospital, the study did not require institutional ethics approval, and individual informed consent was waived because there was no direct intervention in patient care and only coded archival data were used. All procedures complied with institutional policies and the ethical principles of the 1964 Helsinki Declaration and its later amendments.
Consent to Participate
Waived due to the retrospective design and anonymized data.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
REFERENCES
1. Hong YS, Jung KU, Rampal S, Zhao D, Guallar E, Ryu S, et al. Risk factors for hemorrhoidal disease among healthy young and middle-aged Korean adults. Sci Rep. 2022;12(1):129.
2. Hùng NX, Ánh NN. TÌNH HÌNH B?NH TR? TRONG C?NG ??NG VÀ M?T S? Y?U T? LIÊN QUAN. VMJ; 529. Epub ahead of print 30 August 2023. DOI: 10.51298/vmj.v529i1B.6422.
3. Poskus T, Danys D, Makunaite G, Mainelis A, Mikalauskas S, Poskus E, et al. Results of the double-blind randomized controlled trial comparing laser hemorrhoidoplasty with sutured mucopexy and excisional hemorrhoidectomy. Int J Colorectal Dis. 2020;35(3): 481-490. doi: 10.1007/s00384-019-03460-6. Epub 2020 Jan 8.
4. Lie H, Franca Caesarini E, Agung Purnama A, Irawan A, Sudirman T, Saditya Jeo W, et al. Laser hemorrhoidoplasty for hemorrhoidal
disease: a systematic review and meta-analysis. Lasers Med Sci. 2022;37(9):3621-3630. doi: 10.1007/s10103-022-03643-8. Epub 2022 Sep 12.
5. Abdulfattah A, de Oliveira FDP . Laser hemorrhoidoplasty in focus: a modern alternative to conventional surgical techniques for symptomatic hemorrhoids. World J Surg Proced 2025;15(2): 109348. DOI: 10.5412/wjsp.v15.i2.109348
6. Tran DN, Nguyen AT, Nguyen PD, Luu DQ, Nguyen QA, Van Nguyen L, et al. TND’s Vertical Ligation- Mucopexy: A Minimally Invasive Approach for Circumerential Hemorrhoids. Surg. Gastroenterol. Oncol. 2025;30(3):159-166. DOI: 10.21614/sgo-782
7. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation. An epidemiologic study. Gastroenterology. 1990;98(2):380-6. doi: 10.1016/0016-5085(90)90828-o.
8. Chen P-C, Chen C-I. Exploring factors impacting patient decisions in hemorrhoid surgery: A questionnaire survey in Taiwan. Surg Open Sci. 2024;20:214-221. doi: 10.1016/j.sopen.2024.07.009. eCollection 2024 Aug.
9. Islam MdS, Shrestha AB, Chowdhury F, Ziko MRK. Outcomes of laser hemorrhoidoplasty for grade II–IV hemorrhoidal disease in Bangladesh. Ann Med Surg (Lond). 2024;86(11):6514-6520. doi: 10.1097/MS9.0000000000002621. eCollection 2024 Nov.
10. Tran DN, Nguyen AN, Nguyen AT, Nguyen QA, Luu DQ, Nguyen PD, et al. Preliminary Outcomes of Laser Hemorrhoidoplasty for Hemorrhoidal Disease at Hanoi Medical University Hospital. Surg. Gastroenterol. Oncol. 2025;30(4):217-223. DOI: 10.21614/sgo-825
11. Tolksdorf S, Tübergen D, Vivaldi C, Pisek M, Klug F, Kemmerling M, et al. Early and midterm results of radiofrequency ablation (Rafaelo® procedure) for third-degree haemorrhoids: a prospective, two-centre study. Tech Coloproctol. 2022;26(6):479-487. doi: 10.1007/ s10151-022-02608-x. Epub 2022 Mar 19.
12. Khanna R, Khanna S, Bhadani S, Singh S, Khanna AK. Comparison of Ligasure Hemorrhoidectomy with Conventional Ferguson’s Hemorrhoidectomy. Indian J Surg. 2010;72(4):294-7. doi: 10.1007/ s12262-010-0192-3. Epub 2010 Nov 18.
13. Ghani R, Sarwar Z, Niazi SK, Khan RH, Qureshi A. Laser hemorrhoidoplasty(lhp) twisting trend, a study in a small-town hospital. J Postgrad Med Inst. 2025;39(2):134-40. http://doi.org/10.54079/ jpmi.39.2.3540
14. Fang Y, Zhang Y, Zhang D, Zhao Q-l, Li L. Clinical observation on treatment of mixed hemorrhoids with milligan morgan hemorrhoi-dectomy combined with purse-string suture. 2018; https://api. semanticscholar.org/CorpusID:195808305}
15. Long Q, Wen Y, Li J. Milligan-Morgan hemorrhoidectomy combined with rubber band ligation and polidocanol foam sclerotherapy for the management of grade III/IV hemorrhoids: a retrospective study. BMC Gastroenterol. 2025;25(1):355. doi: 10.1186/s12876-025-03963-3.
16. McCloud JM, Jameson JS, Scott AND. Life-threatening sepsis following treatment for haemorrhoids: a systematic review. Colorectal Dis. 2006;8(9):748-55.
17. Porwal A, Gandhi P, Kulkarni D. Laser hemorrhoidopexy: An observational study of 1088 patients treated at single center. Indian J Colo Rectal Surg 2022;5:61 7.
18. Zhang C, Zhang W, Xu J. Comparison of the outcomes of hemorrhoidectomy and PPH in the treatment of grades III and IV hemorrhoids. Medicine (Baltimore). 2022;101(11):e29100. doi: 10.1097/MD.0000000000029100.
Full Text Sources:
Abstract:
Views: 287

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.