Surgery, Gastroenterology and Oncology
Official journal of the International Association of Surgeons, Gastroenterologists and Oncologists
|
|
Systematic Review & Meta-Analysis of Randomized Control Trials Comparing Stapled Hemorrhoidectomy versus Trans Anal Hemorrhoidal Dearterialization for Treatment of Hemorrhoidal Disease
ABSTRACT
Background & Aims: Haemorrhoidal disease is the most common anorectal pathology affecting 50% Irish and 36.4% UK population at some stage in their life. After conservative management with dietary modification and office procedures like rubber band ligation has failed formal haemorrhoidectomy needs to be done. Conventional haemorrhoidectomy has been replaced by new techniques like stapled haemorrhoidectomy (SH) and transanal haemorrhoidal dearterialization (THD) due to its serious complications. We performed this systematic review and meta-analysis of randomised control trials (RCTs) comparing these two modalities.
Methods: The search strategy was designed with help of an experienced librarian for Ovid Medline, EMBASE, Cochrane Library and PubMed until 30th August 2021. The primary outcome of interest was recurrence and secondary outcomes were operative time, pain score and complications.
Results: 10 RCTs pooled a total of 1116 patients with 562 in THD group and 554 in SH group. Based on fixed-effect model the risk ratio (RR) of recurrence among the two groups was 2.44(95% CI 1.70 – 3.51). So, there was a statistical difference among the THD and SH groups in terms of recurrence with more in the THD group, while statistically significant fewer complications 0.57(95% CI 0.39 - 0.84) and reduction in pain scores -0.99(95% CI -1.51 to -0.48) in THD group as compared to SH group was found. Operative times for both groups were similar 4.53(95% CI -0.04 – 9.09) so not statistically significant.
Conclusions: Based on a meta-analysis of 10 RCTs it is found that THD has more recurrence than SH with a better safety profile as reduced complications and pain scores were seen.
Keywords: haemorrhoidal disease, meta-analysis, stapled Haemorrhoidectomy, systematic review
INTRODUCTION
Hemorrhoidal Disease HD is one of the most common problems of the anorectal region resulting in a huge number of appointments in general surgery clinics. HD is classified into grade 1 to 4 by Goliger. Traditionally grades 1 and 2 were treated using office procedures after conservative management has failed. But for 3rd and 4th degree haemorrhoids, surgical procedures were used. With the invention of new procedures and advancement traditional Milligan Morgan technique has been replaced by stapled haemorrhoidectomy SH and THD due to serious complications reported after the former procedure. Sphincter damage leads to incontinence which could be severely debilitating especially in younger patients. Recent network meta-analysis also showed that open procedure resulted in significantly more complications as compared to stapled haemorrhoidectomy and THD. A comparison of these two new techniques was done by Sajid et al (1) in 2012 which compared three RCTs that showed equivocal results after comparison of the two modalities. We felt there is a need to do a systematic review and meta-analysis to find out the superior technique for the treatment of this highly prevalent disease.
Protocol and Registration
The preferred reporting items for systematic reviews and meta-analysis PRISMA (2) was used for reporting of the review. The study was registered with the international prospective registry for systematic reviews PROSPERO (3,4) with registration number CRD42017080268 and is online since 21/11/2017 on the registry.
Eligibility Criteria
PICOS model was used for devising the search strategy for the meta-analysis it is explained in detail in table 1. We included the randomized control trials that compared THD and stapled haemorrhoidectomy for the treatment of haemorrhoids. The primary outcome of interest was the recurrence of haemorrhoids while secondary outcomes of interest were the number of complications, pain score and operative time. The study designs which were included in the meta-analysis were rando-mized control trials no other study type was included.
Information sources
Researcher YB designed a search strategy with the librarian DM. official search was undertaken at the end of August 2021 on bibliography databases Ovid Medline, EMBASE, Cochrane Library and PubMed. All the randomized control trials on comparison of THD with stapled haemorrhoidectomy were included. The primary outcome was the recurrence of haemorrhoids while secondary outcomes were complications, pain score and operative time.
Search Strategy
Search strategies were designed for Ovid Medline, Cochrane Library, EMBASE and PubMed. MeSH terms and EMTREE terms were used as appropriate while using the PICOS model for the structuring of the search strategies. Combination of keywords to identify published studies comparing THD and stapled haemorrhoidectomy for the treatment of haemorrhoids were used. Subject headings and keywords relating to haemorrhoids, procedure for prolapsed haemorrhoids, stapled haemorrhoidectomy and trans anal rectal dearterialization or trans anal hemorrhoidal dearterialization were used. Language, geographical and date restrictions were not applied, additional studies were identified by reference searching.
Table 1 - PICOS model used for the systematic review as per PRISMA protocol and its explanation
Study Selection
After duplicates were removed, all the studies identified in the search were screened independently by two reviewers by YB & QU. Using article title and abstract against predefined inclusion and exclusion criteria. If there was any conflict about a study, it was resolved with consensus. Conference proceedings were also included if they met the inclusion criteria and had the required information, at least primary outcome should be available in order to include the study into meta-analysis. The reviewers were not blinded regarding the authors and the institutes of the studies. If some data were not available, the authors of the study were contacted by email.
Data Colletion process
Data were extracted by two independent researchers YB and QU using predetermined data extraction forms independently and matched. There were two parts of the form, first gathered general information regarding the article while the second was focused on primary and secondary outcomes.
Data items
Data on primary outcome “recurrence was recorded as a number of patients having recurrence” of haemorrhoids. Secondary outcomes including “complications as number of complications, pain scores mean pain score and operative time as minutes” was recorded using the second part of pre-formed data collection form.
Risk of biasin individual studies
Individual studies were assessed using JADAD scoring also known as the Oxford quality scoring system for randomised control trials. JADAD scoring system independently assess the methodological quality of a clinical trial. It allocates trials scores between zero (very poor) to five (very rigorous).
Summary measures & Synthesis of results
For the primary outcome, risk ratio along with 95% confidence interval was calculated using meta-analysis software Review Manager Copenhagen: The Nordic COCHRANE Collaboration, 2014)(5). For secondary outcomes complications, odds ratio with 95% confidence interval was calculated, while mean difference with 95% confidence interval for operative time and pain score was calculated. Using the above-mentioned software, pool estimates of recurrence, pain score, complications and operative time were calculated. I2 was used as a measure of heterogeneity among the studies while p-value less than 0.05 was considered significant where appropriate.
Study selection
A total of 263 articles were identified using electronic databases including Ovid MEDLINE, PubMed, Cochrane Library and EMBASE. One more article was found using a hand search of the bibliographies of the relevant papers. 206 articles were left once duplicates were removed. The screening was done using titles and abstracts against a pre-determined criterion using PICOS model which is explained in detail in table 1. 14 articles were selected for full text, which were studied in detail and out of them 10 (6-15) met all the criteria and were included in systematic review and metaanalysis. PRISMA flowchart in fig. 1 can be seen for a full explanation of each step. Out of 4 which were excluded at full-text level, two were presentations which later became full articles and are included in the meta-analysis, the primary outcome of interest was not declared in one study (16) and one article was found to have unreliable data and was retracted by the journal (17).
Risk of Bias within studies
All these studies were independently assessed by two reviewers YB and QU for quality and assessment with a JADAD score (18) also known as the Oxford quality scoring system. JADAD scoring system is for assessment of RCT’s for bias scores ranging between 0 being very poor and five being very rigorous randomized control trial score for the studies range between 1 and 3. So the studies were low to moderate quality
Synthetisis of results
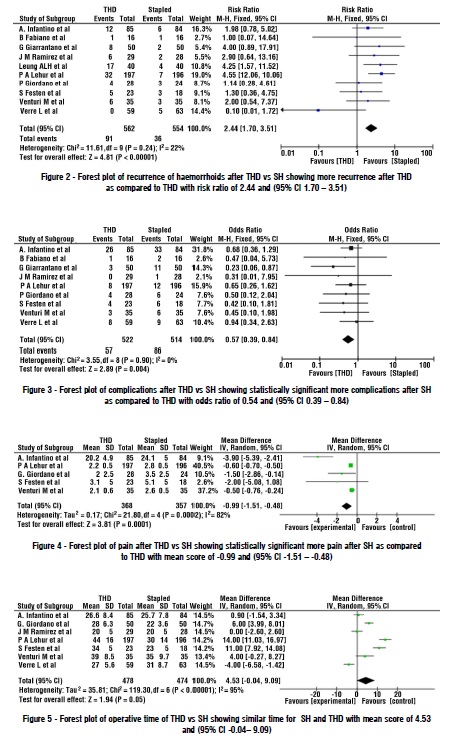
There was a total of 1116 patients pooled from 10 RCTs included in the meta-analysis. Roughly similar numbers i-e 562 and 554 patients were present in THD and stapled haemorrhoidectomy (SH) groups respectively. Based on fixed-effect model risk ratio of recurrence was found to be 2.44 (95% CI 1.70 – 3.51), showing increased recurrence with THD as compared to SH (fig. 2). I2 which is a measure of heterogeneity was 22% which is low showing significant homogeneity among the studies. Secondary outcomes of interest were complications, operative time and pain. They were analysed by the data provided by the studies. Using fixed model effect studies showed odds of 0.57(95% CI 0.39 - 0.84) showing a statistically significant reduced chance of having complications with THD as compared to Stapled haemorrhoidectomy, while I2 was 0% showing homogeneity among the studies (fig. 3). Pain scores when compared among the two modalities also showed similar results, using random-effect model mean difference among the two procedures was -0.99(95% CI -1.51 to -0.48) showing statistically reduced pain scores with THD (19) as compared to stapled group (fig. 4). While similar operative times were found between the two procedures, using random-effect model mean difference of 4.53(95% CI -0.04 – 9.09) was found, which is not statistically significant (fig. 5).

DISCUSSION
The haemorrhoidal disease is one of the most prevalent diseases of the anorectal region with 36.4% population of United Kingdom (20) affected by the disease, while 10 million people are affected with haemorrhoidal disease in the USA (21) at some stage in their life. 1st and 2nd - degree haemorrhoids are treated by office procedures (22) while surgical treatment is reserved for the 3rd and 4th degree haemorrhoids. In 1990s two new techniques were invented Transanal Haemorrhoidal Dearterialisation (23) and Stapled haemoroidectomy (24) and both became quite popular among surgeons. The reasons were simple, serious complications were reported secondary to the Milligan- Morgan procedure (conventional haemorroidectomy) along with severe post-op pain (25). Both of these techniques are quite promising with excellent results reported in the literature. There is only one systematic review done on the direct comparison of the two techniques by Sajid et al (1) in 2012 included 3 randomised control trials. We took this opportunity to search the literature and ascertain the randomised control trials done on comparison of the two techniques and analyse the pooled data for both. Our literature search revealed 14 articles that were analysed for full text and we included 10 RCT’s in our systematic review and meta-analysis. Our analysis of the data revealed that our meta-analysis included 562 patients in the THD group vs 554 patients pooled in stapled haemorroidectomy group. The primary outcome of interest was recurrence and when we analysed the pooled data it showed that SH. The risk ratio was 2.44 with 95% CI 1.70-3.51 between the two procedures, thus THD has more recurrence than SH. These results are consistent with results by Sajid et al in 2012 (1). A systematic review by Sajid et al reported a statistically non-significant difference in terms of complications and operative time between the two techniques. But it has been shown by the same review that was statistically signifficant difference in pain scores between them. We pooled the data for all the above-mentioned variables where available, and analysed and found that there were statistically significant more complications and pain score by stapled haemorrhoidectomy (SH) as compared to THD. While similar operative time was found between the two methods. THD procedure is less invasive as compared to stapled haemoidectomy as earlier does not involve any excision. Consequently, although statistically more complications were reported in the stapled group, the complications reported secondary to stapled haemorroidectomy are also more serious including pelvic sepsis, suture dehiscence, anal stricutres, anal strictures and incontinence secondary to the stapled haemorrhoidectomy (26,27). Also, network meta-analysis in 2015 comparing all types of treatments for haemorrhoids found significantly lower re-operation rates for THD as compared to any other form of haemorrhoidal surgery. An RCT published in 2017 by A.L.Leung et al (9) caught our attention as results shown by this RCT were quite different from the other RCTs and available literature. C.Ratto et al (28) mentioned a few weaknesses in the RCT and our surgical group also found serious discrepancies (29) which were mentioned. The objections and responses (30) to the objections can also be viewed by readers. We leave it to our readers to make their own opinion using their clinical experience and judgment. The pooled results after including RCT by Leung et al showed there is statistically significant increased recurrence after THD as compared to stapled haemorrhoidectomy. But we leave it to our readers to make decisions about the outcome.
CONCLUSIONS
To conclude, more recurrence found in THD group as compared to SH group in the pooled data of 10 RCTs but 9 trials provided data on complications and analysis showed more complications associated with stapled haemorrhoidectomy than THD. Readers should keep this in mind that the complications reported after stapled haemorrhoidectomy can range from very minimal like bleeding to very severe like pelvic sepsis while no serious life-threatening complication has been reported after THD. Some studies have also shown damage to the sphincter resulting in incontinence or soiling after stapled haemorrhoidectomy. While urine retention is the most common complication reported after THD. This result is different from the one shown by Sajid et al which mentioned no statistically significant difference in complications among the two groups. More pain postoperatively with staple haemorrhoidectomy as compared to THD was found. Analysis of operative time showed no difference between SH and THD. All studies showed less operative time for SH as compared to THD. Only Verre et al (14) showed longer operative time of SH as compared to THD. This result is consistent with results shown by Sajid at al.
REFERENCES
1. Sajid M, Parampalli U, Whitehouse P, Sains P, McFall M, Baig M. A systematic review comparing transanal haemorrhoidal de-arterialisation to stapled haemorrhoidopexy in the management of haemorrhoidal disease. Tech Coloproctol. 2012;16(1):1-8.
2. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS medicine. 2009;6(7):e1000097.
3. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and metaanalysis protocols (PRISMA-P) 2015: elaboration and explanation. Bmj. 2015;349:g7647.
4. Bashir Y, Conlon K. Step by step guide to do a systematic review and meta-analysis for medical professionals. Ir J Med Sci. 2018;187(2): 447-452. Epub 2017 Jul 22.
5. Bax L, Yu L-M, Ikeda N, Moons KG. A systematic comparison of software dedicated to meta-analysis of causal studies. BMC Med Res Methodol. 2007;7:40.
6. Infantino A, Altomare D, Bottini C, Bonanno M, Mancini S. Prospective randomized multicentre study comparing stapler haemorrhoidopexy with Doppler-guided transanal haemorrhoid dearterialization for third-degree haemorrhoids. Colorectal Dis. 2012;14(2):205-11.
7. Fabiani B, Giani I, Menconi C, Toniolo G, Martellucci J, Naldini G. Partial Stapled Haemorrhoidopexy (psh) versus Transanal Haemorrhoidal Dearterialization (thd) for Iii grade haemorrhoids: early results. Colorectal Disease. 2014;16:100.
8. Ramirez J, Gracia J, Aguilella V, Elia M, Casamayor M, Martinez M. Surgical management of symptomatic haemorrhoids. Colorectal Disease Supplement. 2005;7:52.
9. Leung A, Cheung T, Tung K, Tsang Y, Cheung H, Lau C, et al. A prospective randomized controlled trial evaluating the short-term outcomes of transanal hemorrhoidal dearterialization versus tissue-selecting technique. Tech Coloproctol. 2017;21(9):737-743.
10. Lehur PA, Didnée AS, Faucheron J-L, Meurette G, Zerbib P, Siproudhis L, et al. Cost-effectiveness of new surgical treatments for hemorrhoidal disease: a multicentre randomized controlled trial comparing transanal Doppler-guided hemorrhoidal artery ligation with mucopexy and circular stapled hemorrhoidopexy. Ann Surg. 2016;264(5):710-716.
11. Giordano P, Nastro P, Davies A, Gravante G. Prospective evaluation of stapled haemorrhoidopexy versus transanal haemorrhoidal dearterialisation for stage II and III haemorrhoids: three-year outcomes. Tech Coloproctol. 2011;15(1):67-73.
12. Festen S, Van Hoogstraten M, Van Geloven A, Gerhards M. Treatment of grade III and IV haemorrhoidal disease with PPH or THD. A randomized trial on postoperative complications and shortterm results. Int J Colorectal Dis. 2009;24(12):1401-5.
13. Venturi M, Salamina G, Vergani C. Stapled anopexy versus transanal hemorrhoidal dearterialization for hemorrhoidal disease: a threeyear follow-up from a randomized study. Minerva Chir. 2016;71(6): 365-371.
14. Verre L, Rossi R, Gaggelli I, Di Bella C, Tirone A, Piccolomini A. PPH versus THD: a comparison of two techniques for III and IV degree haemorrhoids. Personal experience. Minerva Chir. 2013; 68(6):543-50.
15. Giarratano G, Toscana E, Toscana C, Petrella G, Shalaby M, Sileri P. Transanal hemorrhoidal dearterialization versus stapled hemorrhoidopexy: long-term follow-up of a prospective randomized study. Surg Innov. 2018;25(3):236-241.
16. Béliard A, Labbé F, De Faucal D, Fabreguette J-M, Pouderoux P, Borie F. A prospective and comparative study between stapled hemorrhoidopexy and hemorrhoidal artery ligation with mucopexy. J Visc Surg. 2014;151(4):257-62.
17. Lucarelli R, Picchio M, Caporossi M, De Angelis F, Di Filippo A, Stipa F, et al. Transanal haemorrhoidal dearterialisation with mucopexy versus stapler haemorrhoidopexy: a randomised trial with long-term follow-up. Ann R Coll Surg Engl. 2013;95(4):246-51.
18. Moher D, Jones A, Cook DJ, Jadad AR, Moher M, Tugwell P, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet. 1998; 352(9128):609-13.
19. Cho S, Lee R-A, Chung SS, Kim KH. Early experience of Dopplerguided hemorrhoidal artery ligation and rectoanal repair (DG-HAL & RAR) for the treatment of symptomatic hemorrhoids. J Korean Surgical Society. 2010;78(1):23-8.
20. Hardy A, Chan C, Cohen C. The surgical management of haemorrhoids– a review. Dig Surg. 2005;22(1-2):26-33.
21. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation: an epidemiologic study. Gastroenterology. 1990;98(2):380-6.
22. Nisar PJ, Scholefield JH. Managing haemorrhoids. BMJ. 2003; 327(7419):847-51.
23. Morinaga K, Hasuda K, Ikeda T. A novel therapy for internal hemorrhoids: ligation of the hemorrhoidal artery with a newly devised instrument (Moricorn) in conjunction with a Doppler flowmeter. Am J Gastroenterol. 1995;90(4):610-3.
24. Fazio VW. Early promise of stapling technique for haemorrhoidectomy. Lancet. 2000;355(9206):768-9.
25. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg. 2001;88(8):1049-53.
26. Oughriss M, Yver R, Faucheron J-L. Complications of stapled hemorrhoidectomy: a French multicentric study. Gastroentérologie clinique et biologique. 2005;29(4):429-33.
27. Ravo B, Amato A, Bianco V, Boccasanta P, Bottini C, Carriero A, et al. Complications after stapled hemorrhoidectomy: can they be prevented? Techniques in coloproctology. 2002;6(2):83-8.
28. Biondo S, Trenti L, Kreisler E, Ratto C. A prospective randomized trial on transanal hemorrhoidal dearterialization versus stapler hemorrhoidectomy: methodological issues that need to be clarified. Tech Coloproctol. 2018;22(2):145-146. Epub 2017 Oct 28.
29. Bashir Y, Ulain Q, Eguare E. Short-term outcomes of transanal haemorrhoidal dearterialization versus tissue-selecting technique. Tech Coloproctol. 2018;22(2):147.
30. Leung LH. Reply to the letter to the editor regarding: A prospective randomized trial evaluating the outcomes of transanal hemorrhoidal dearterialization versus tissue-selecting technique. Tech Coloproctol. 2018;22(2):149-150.
Full Text Sources:
Abstract:
Views: 8596

Background & Aims: Haemorrhoidal disease is the most common anorectal pathology affecting 50% Irish and 36.4% UK population at some stage in their life. After conservative management with dietary modification and office procedures like rubber band ligation has failed formal haemorrhoidectomy needs to be done. Conventional haemorrhoidectomy has been replaced by new techniques like stapled haemorrhoidectomy (SH) and transanal haemorrhoidal dearterialization (THD) due to its serious complications. We performed this systematic review and meta-analysis of randomised control trials (RCTs) comparing these two modalities.
Methods: The search strategy was designed with help of an experienced librarian for Ovid Medline, EMBASE, Cochrane Library and PubMed until 30th August 2021. The primary outcome of interest was recurrence and secondary outcomes were operative time, pain score and complications.
Results: 10 RCTs pooled a total of 1116 patients with 562 in THD group and 554 in SH group. Based on fixed-effect model the risk ratio (RR) of recurrence among the two groups was 2.44(95% CI 1.70 – 3.51). So, there was a statistical difference among the THD and SH groups in terms of recurrence with more in the THD group, while statistically significant fewer complications 0.57(95% CI 0.39 - 0.84) and reduction in pain scores -0.99(95% CI -1.51 to -0.48) in THD group as compared to SH group was found. Operative times for both groups were similar 4.53(95% CI -0.04 – 9.09) so not statistically significant.
Conclusions: Based on a meta-analysis of 10 RCTs it is found that THD has more recurrence than SH with a better safety profile as reduced complications and pain scores were seen.
Keywords: haemorrhoidal disease, meta-analysis, stapled Haemorrhoidectomy, systematic review
INTRODUCTION
Hemorrhoidal Disease HD is one of the most common problems of the anorectal region resulting in a huge number of appointments in general surgery clinics. HD is classified into grade 1 to 4 by Goliger. Traditionally grades 1 and 2 were treated using office procedures after conservative management has failed. But for 3rd and 4th degree haemorrhoids, surgical procedures were used. With the invention of new procedures and advancement traditional Milligan Morgan technique has been replaced by stapled haemorrhoidectomy SH and THD due to serious complications reported after the former procedure. Sphincter damage leads to incontinence which could be severely debilitating especially in younger patients. Recent network meta-analysis also showed that open procedure resulted in significantly more complications as compared to stapled haemorrhoidectomy and THD. A comparison of these two new techniques was done by Sajid et al (1) in 2012 which compared three RCTs that showed equivocal results after comparison of the two modalities. We felt there is a need to do a systematic review and meta-analysis to find out the superior technique for the treatment of this highly prevalent disease.
Protocol and Registration
The preferred reporting items for systematic reviews and meta-analysis PRISMA (2) was used for reporting of the review. The study was registered with the international prospective registry for systematic reviews PROSPERO (3,4) with registration number CRD42017080268 and is online since 21/11/2017 on the registry.
Eligibility Criteria
PICOS model was used for devising the search strategy for the meta-analysis it is explained in detail in table 1. We included the randomized control trials that compared THD and stapled haemorrhoidectomy for the treatment of haemorrhoids. The primary outcome of interest was the recurrence of haemorrhoids while secondary outcomes of interest were the number of complications, pain score and operative time. The study designs which were included in the meta-analysis were rando-mized control trials no other study type was included.
Information sources
Researcher YB designed a search strategy with the librarian DM. official search was undertaken at the end of August 2021 on bibliography databases Ovid Medline, EMBASE, Cochrane Library and PubMed. All the randomized control trials on comparison of THD with stapled haemorrhoidectomy were included. The primary outcome was the recurrence of haemorrhoids while secondary outcomes were complications, pain score and operative time.
Search Strategy
Search strategies were designed for Ovid Medline, Cochrane Library, EMBASE and PubMed. MeSH terms and EMTREE terms were used as appropriate while using the PICOS model for the structuring of the search strategies. Combination of keywords to identify published studies comparing THD and stapled haemorrhoidectomy for the treatment of haemorrhoids were used. Subject headings and keywords relating to haemorrhoids, procedure for prolapsed haemorrhoids, stapled haemorrhoidectomy and trans anal rectal dearterialization or trans anal hemorrhoidal dearterialization were used. Language, geographical and date restrictions were not applied, additional studies were identified by reference searching.
Table 1 - PICOS model used for the systematic review as per PRISMA protocol and its explanation
| PICOS | Inclusion and Exclusion criteria |
| Patient | Inclusion: Patients suffering from haemorrhoids Exclusion: Patients under the age of 18. |
| Intervention | Patients treated with Transanal Haemorrhoidal Dematerialisation (THD) |
| Comparison | Patients treated with Stapled Haemorrhoidectomy (SH) |
| Outcome | Primary outcome: Recurrence Secondary outcome: Complications, Pain score, Operative time. |
| Study Design | Inclusion: Randomized controlled trials. Exclusion: All other study designs, Animal studies were excluded |
Study Selection
After duplicates were removed, all the studies identified in the search were screened independently by two reviewers by YB & QU. Using article title and abstract against predefined inclusion and exclusion criteria. If there was any conflict about a study, it was resolved with consensus. Conference proceedings were also included if they met the inclusion criteria and had the required information, at least primary outcome should be available in order to include the study into meta-analysis. The reviewers were not blinded regarding the authors and the institutes of the studies. If some data were not available, the authors of the study were contacted by email.
Data Colletion process
Data were extracted by two independent researchers YB and QU using predetermined data extraction forms independently and matched. There were two parts of the form, first gathered general information regarding the article while the second was focused on primary and secondary outcomes.
Data items
Data on primary outcome “recurrence was recorded as a number of patients having recurrence” of haemorrhoids. Secondary outcomes including “complications as number of complications, pain scores mean pain score and operative time as minutes” was recorded using the second part of pre-formed data collection form.
Risk of biasin individual studies
Individual studies were assessed using JADAD scoring also known as the Oxford quality scoring system for randomised control trials. JADAD scoring system independently assess the methodological quality of a clinical trial. It allocates trials scores between zero (very poor) to five (very rigorous).
Summary measures & Synthesis of results
For the primary outcome, risk ratio along with 95% confidence interval was calculated using meta-analysis software Review Manager Copenhagen: The Nordic COCHRANE Collaboration, 2014)(5). For secondary outcomes complications, odds ratio with 95% confidence interval was calculated, while mean difference with 95% confidence interval for operative time and pain score was calculated. Using the above-mentioned software, pool estimates of recurrence, pain score, complications and operative time were calculated. I2 was used as a measure of heterogeneity among the studies while p-value less than 0.05 was considered significant where appropriate.
Study selection
A total of 263 articles were identified using electronic databases including Ovid MEDLINE, PubMed, Cochrane Library and EMBASE. One more article was found using a hand search of the bibliographies of the relevant papers. 206 articles were left once duplicates were removed. The screening was done using titles and abstracts against a pre-determined criterion using PICOS model which is explained in detail in table 1. 14 articles were selected for full text, which were studied in detail and out of them 10 (6-15) met all the criteria and were included in systematic review and metaanalysis. PRISMA flowchart in fig. 1 can be seen for a full explanation of each step. Out of 4 which were excluded at full-text level, two were presentations which later became full articles and are included in the meta-analysis, the primary outcome of interest was not declared in one study (16) and one article was found to have unreliable data and was retracted by the journal (17).
Risk of Bias within studies
All these studies were independently assessed by two reviewers YB and QU for quality and assessment with a JADAD score (18) also known as the Oxford quality scoring system. JADAD scoring system is for assessment of RCT’s for bias scores ranging between 0 being very poor and five being very rigorous randomized control trial score for the studies range between 1 and 3. So the studies were low to moderate quality
Synthetisis of results
There was a total of 1116 patients pooled from 10 RCTs included in the meta-analysis. Roughly similar numbers i-e 562 and 554 patients were present in THD and stapled haemorrhoidectomy (SH) groups respectively. Based on fixed-effect model risk ratio of recurrence was found to be 2.44 (95% CI 1.70 – 3.51), showing increased recurrence with THD as compared to SH (fig. 2). I2 which is a measure of heterogeneity was 22% which is low showing significant homogeneity among the studies. Secondary outcomes of interest were complications, operative time and pain. They were analysed by the data provided by the studies. Using fixed model effect studies showed odds of 0.57(95% CI 0.39 - 0.84) showing a statistically significant reduced chance of having complications with THD as compared to Stapled haemorrhoidectomy, while I2 was 0% showing homogeneity among the studies (fig. 3). Pain scores when compared among the two modalities also showed similar results, using random-effect model mean difference among the two procedures was -0.99(95% CI -1.51 to -0.48) showing statistically reduced pain scores with THD (19) as compared to stapled group (fig. 4). While similar operative times were found between the two procedures, using random-effect model mean difference of 4.53(95% CI -0.04 – 9.09) was found, which is not statistically significant (fig. 5).
DISCUSSION
The haemorrhoidal disease is one of the most prevalent diseases of the anorectal region with 36.4% population of United Kingdom (20) affected by the disease, while 10 million people are affected with haemorrhoidal disease in the USA (21) at some stage in their life. 1st and 2nd - degree haemorrhoids are treated by office procedures (22) while surgical treatment is reserved for the 3rd and 4th degree haemorrhoids. In 1990s two new techniques were invented Transanal Haemorrhoidal Dearterialisation (23) and Stapled haemoroidectomy (24) and both became quite popular among surgeons. The reasons were simple, serious complications were reported secondary to the Milligan- Morgan procedure (conventional haemorroidectomy) along with severe post-op pain (25). Both of these techniques are quite promising with excellent results reported in the literature. There is only one systematic review done on the direct comparison of the two techniques by Sajid et al (1) in 2012 included 3 randomised control trials. We took this opportunity to search the literature and ascertain the randomised control trials done on comparison of the two techniques and analyse the pooled data for both. Our literature search revealed 14 articles that were analysed for full text and we included 10 RCT’s in our systematic review and meta-analysis. Our analysis of the data revealed that our meta-analysis included 562 patients in the THD group vs 554 patients pooled in stapled haemorroidectomy group. The primary outcome of interest was recurrence and when we analysed the pooled data it showed that SH. The risk ratio was 2.44 with 95% CI 1.70-3.51 between the two procedures, thus THD has more recurrence than SH. These results are consistent with results by Sajid et al in 2012 (1). A systematic review by Sajid et al reported a statistically non-significant difference in terms of complications and operative time between the two techniques. But it has been shown by the same review that was statistically signifficant difference in pain scores between them. We pooled the data for all the above-mentioned variables where available, and analysed and found that there were statistically significant more complications and pain score by stapled haemorrhoidectomy (SH) as compared to THD. While similar operative time was found between the two methods. THD procedure is less invasive as compared to stapled haemoidectomy as earlier does not involve any excision. Consequently, although statistically more complications were reported in the stapled group, the complications reported secondary to stapled haemorroidectomy are also more serious including pelvic sepsis, suture dehiscence, anal stricutres, anal strictures and incontinence secondary to the stapled haemorrhoidectomy (26,27). Also, network meta-analysis in 2015 comparing all types of treatments for haemorrhoids found significantly lower re-operation rates for THD as compared to any other form of haemorrhoidal surgery. An RCT published in 2017 by A.L.Leung et al (9) caught our attention as results shown by this RCT were quite different from the other RCTs and available literature. C.Ratto et al (28) mentioned a few weaknesses in the RCT and our surgical group also found serious discrepancies (29) which were mentioned. The objections and responses (30) to the objections can also be viewed by readers. We leave it to our readers to make their own opinion using their clinical experience and judgment. The pooled results after including RCT by Leung et al showed there is statistically significant increased recurrence after THD as compared to stapled haemorrhoidectomy. But we leave it to our readers to make decisions about the outcome.
CONCLUSIONS
To conclude, more recurrence found in THD group as compared to SH group in the pooled data of 10 RCTs but 9 trials provided data on complications and analysis showed more complications associated with stapled haemorrhoidectomy than THD. Readers should keep this in mind that the complications reported after stapled haemorrhoidectomy can range from very minimal like bleeding to very severe like pelvic sepsis while no serious life-threatening complication has been reported after THD. Some studies have also shown damage to the sphincter resulting in incontinence or soiling after stapled haemorrhoidectomy. While urine retention is the most common complication reported after THD. This result is different from the one shown by Sajid et al which mentioned no statistically significant difference in complications among the two groups. More pain postoperatively with staple haemorrhoidectomy as compared to THD was found. Analysis of operative time showed no difference between SH and THD. All studies showed less operative time for SH as compared to THD. Only Verre et al (14) showed longer operative time of SH as compared to THD. This result is consistent with results shown by Sajid at al.
REFERENCES
1. Sajid M, Parampalli U, Whitehouse P, Sains P, McFall M, Baig M. A systematic review comparing transanal haemorrhoidal de-arterialisation to stapled haemorrhoidopexy in the management of haemorrhoidal disease. Tech Coloproctol. 2012;16(1):1-8.
2. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS medicine. 2009;6(7):e1000097.
3. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and metaanalysis protocols (PRISMA-P) 2015: elaboration and explanation. Bmj. 2015;349:g7647.
4. Bashir Y, Conlon K. Step by step guide to do a systematic review and meta-analysis for medical professionals. Ir J Med Sci. 2018;187(2): 447-452. Epub 2017 Jul 22.
5. Bax L, Yu L-M, Ikeda N, Moons KG. A systematic comparison of software dedicated to meta-analysis of causal studies. BMC Med Res Methodol. 2007;7:40.
6. Infantino A, Altomare D, Bottini C, Bonanno M, Mancini S. Prospective randomized multicentre study comparing stapler haemorrhoidopexy with Doppler-guided transanal haemorrhoid dearterialization for third-degree haemorrhoids. Colorectal Dis. 2012;14(2):205-11.
7. Fabiani B, Giani I, Menconi C, Toniolo G, Martellucci J, Naldini G. Partial Stapled Haemorrhoidopexy (psh) versus Transanal Haemorrhoidal Dearterialization (thd) for Iii grade haemorrhoids: early results. Colorectal Disease. 2014;16:100.
8. Ramirez J, Gracia J, Aguilella V, Elia M, Casamayor M, Martinez M. Surgical management of symptomatic haemorrhoids. Colorectal Disease Supplement. 2005;7:52.
9. Leung A, Cheung T, Tung K, Tsang Y, Cheung H, Lau C, et al. A prospective randomized controlled trial evaluating the short-term outcomes of transanal hemorrhoidal dearterialization versus tissue-selecting technique. Tech Coloproctol. 2017;21(9):737-743.
10. Lehur PA, Didnée AS, Faucheron J-L, Meurette G, Zerbib P, Siproudhis L, et al. Cost-effectiveness of new surgical treatments for hemorrhoidal disease: a multicentre randomized controlled trial comparing transanal Doppler-guided hemorrhoidal artery ligation with mucopexy and circular stapled hemorrhoidopexy. Ann Surg. 2016;264(5):710-716.
11. Giordano P, Nastro P, Davies A, Gravante G. Prospective evaluation of stapled haemorrhoidopexy versus transanal haemorrhoidal dearterialisation for stage II and III haemorrhoids: three-year outcomes. Tech Coloproctol. 2011;15(1):67-73.
12. Festen S, Van Hoogstraten M, Van Geloven A, Gerhards M. Treatment of grade III and IV haemorrhoidal disease with PPH or THD. A randomized trial on postoperative complications and shortterm results. Int J Colorectal Dis. 2009;24(12):1401-5.
13. Venturi M, Salamina G, Vergani C. Stapled anopexy versus transanal hemorrhoidal dearterialization for hemorrhoidal disease: a threeyear follow-up from a randomized study. Minerva Chir. 2016;71(6): 365-371.
14. Verre L, Rossi R, Gaggelli I, Di Bella C, Tirone A, Piccolomini A. PPH versus THD: a comparison of two techniques for III and IV degree haemorrhoids. Personal experience. Minerva Chir. 2013; 68(6):543-50.
15. Giarratano G, Toscana E, Toscana C, Petrella G, Shalaby M, Sileri P. Transanal hemorrhoidal dearterialization versus stapled hemorrhoidopexy: long-term follow-up of a prospective randomized study. Surg Innov. 2018;25(3):236-241.
16. Béliard A, Labbé F, De Faucal D, Fabreguette J-M, Pouderoux P, Borie F. A prospective and comparative study between stapled hemorrhoidopexy and hemorrhoidal artery ligation with mucopexy. J Visc Surg. 2014;151(4):257-62.
17. Lucarelli R, Picchio M, Caporossi M, De Angelis F, Di Filippo A, Stipa F, et al. Transanal haemorrhoidal dearterialisation with mucopexy versus stapler haemorrhoidopexy: a randomised trial with long-term follow-up. Ann R Coll Surg Engl. 2013;95(4):246-51.
18. Moher D, Jones A, Cook DJ, Jadad AR, Moher M, Tugwell P, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet. 1998; 352(9128):609-13.
19. Cho S, Lee R-A, Chung SS, Kim KH. Early experience of Dopplerguided hemorrhoidal artery ligation and rectoanal repair (DG-HAL & RAR) for the treatment of symptomatic hemorrhoids. J Korean Surgical Society. 2010;78(1):23-8.
20. Hardy A, Chan C, Cohen C. The surgical management of haemorrhoids– a review. Dig Surg. 2005;22(1-2):26-33.
21. Johanson JF, Sonnenberg A. The prevalence of hemorrhoids and chronic constipation: an epidemiologic study. Gastroenterology. 1990;98(2):380-6.
22. Nisar PJ, Scholefield JH. Managing haemorrhoids. BMJ. 2003; 327(7419):847-51.
23. Morinaga K, Hasuda K, Ikeda T. A novel therapy for internal hemorrhoids: ligation of the hemorrhoidal artery with a newly devised instrument (Moricorn) in conjunction with a Doppler flowmeter. Am J Gastroenterol. 1995;90(4):610-3.
24. Fazio VW. Early promise of stapling technique for haemorrhoidectomy. Lancet. 2000;355(9206):768-9.
25. Shalaby R, Desoky A. Randomized clinical trial of stapled versus Milligan-Morgan haemorrhoidectomy. Br J Surg. 2001;88(8):1049-53.
26. Oughriss M, Yver R, Faucheron J-L. Complications of stapled hemorrhoidectomy: a French multicentric study. Gastroentérologie clinique et biologique. 2005;29(4):429-33.
27. Ravo B, Amato A, Bianco V, Boccasanta P, Bottini C, Carriero A, et al. Complications after stapled hemorrhoidectomy: can they be prevented? Techniques in coloproctology. 2002;6(2):83-8.
28. Biondo S, Trenti L, Kreisler E, Ratto C. A prospective randomized trial on transanal hemorrhoidal dearterialization versus stapler hemorrhoidectomy: methodological issues that need to be clarified. Tech Coloproctol. 2018;22(2):145-146. Epub 2017 Oct 28.
29. Bashir Y, Ulain Q, Eguare E. Short-term outcomes of transanal haemorrhoidal dearterialization versus tissue-selecting technique. Tech Coloproctol. 2018;22(2):147.
30. Leung LH. Reply to the letter to the editor regarding: A prospective randomized trial evaluating the outcomes of transanal hemorrhoidal dearterialization versus tissue-selecting technique. Tech Coloproctol. 2018;22(2):149-150.
Full Text Sources:
Abstract:
Views: 8596
Watch Video Articles
For Authors
Journal Subscriptions

Current Issue
Mar 2026
Supplements
Instructions for authors
Online submission
Contact
ISSN: 2559 - 723X (print)
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Open Access Statement
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Journal Metrics
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.