Surgery, Gastroenterology and Oncology

|
|
Background and Aim: to compare the early outcome results of laparoscopic versus open management as laparoscopic management seems to have multiple attractions for surgeons with marked controversy.
Materials and Methods: All patients of Gastroduodenal perforation were included and randomized for laparoscopic or open repair. The data obtained from the diagnostic flowchart, operative details, postoperative morbidities, and mortalities were collected for statistical analysis.
Results: sixty-six patients were assigned to the group laparoscopic cases and 74 candidates to the open one. The rate of conversion was 45.5% (n=30/66). The finished laparoscopy group had a noticeably longer operating time, less postoperative discomfort, a lower rate of wound infection, and a shorter hospital stay than the open group. Additionally, there was a decreased incidence of pulmonary problems, wound dehiscence, leakage, ileus, intra-abdominal collection, and other complications in the laparoscopic group, and re-intervention than in the open group. The risk factors for conversion included age, preoperative shock, a high Boey score, a high Mannheim peritonitis index, and co-morbidities. However, by multivariate analysis, only preoperative shock and old age were predictors of conversion.
Conclusion: In individuals with low surgical risk, laparoscopic repair is as possible and secure as compared to open repair (Boey score 0 and 1). Laparoscopic repair has multiple advantages in comparison with open repair.
Clinical significance: laparoscopic repair of a perforated peptic ulcer has many benefits in comparison with the open repair; (lower postoperative pain, lower incidence of postoperative morbidities, better cosmetic outcome, earlier recovery, and shorter hospital stay).
Introduction
Despite improvements in perioperative care, imaging techniques, and surgical management, gastroduodenal perforations (GDP) account for 5-10% of peptic ulcer disease (PUD). They consequently account for most PUD emergency surgeries (1).
As older age, co-morbidity, and late presentation are linked with higher mortality rates, identifying, and modifying these factors are very important to enhance outcomes, such as early diagnosis and prompt resuscitation, GDP-induced mortality, and morbidity call for a well-planned therapeutic approach (2,3).
The laparoscopic repair of perforated peptic ulcers has increasingly gained popularity against open ones. Several clinical parameters should be identified for the selection of candidates for laparoscopic management (4).
A laparoscope allows easy access to the deep intraperitoneal recesses, particularly without the need to extend the abdominal incision midline (5). In this study, the aim was the re-evaluation of the status of laparoscopic management of GDP and the release of a recommendation statement about the perioperative outcome in comparison to the open approach according to our 2-center experience.
Materials and Methods
This prospective comparative experience was observed from May 2017 to October 2021, at Mansoura Emergency Hospital/Egypt and king Faisal medical complex /Saudi Arabia. The Candidates of GDP were counseled about the two surgical approaches and the study participants signed an informed consent.
All candidates fulfilling the inclusion criteria were enrolled in the study including an acute abdomen with a perforated peptic ulcer diagnosed clinically within 48 hours of the onset of symptoms, and the patient age is 16-70 years old. In addition, candidates with absolute contraindications for laparoscopy were excluded, including those with malignant ulcers, rare sites of peptic ulcer, other complications with GDP, and pregnant women with PPU.
A complete history and a full clinical examination, a laboratory analysis, and an imaging study were all conducted on all candidate patients.
A clinical assessment and investigation were conducted to determine the surgical risk based on the Boey score (6) and the American Society of Anesthesiologists Association Score (ASA) (7).
A and B were randomly assigned to laparoscopic or open pedicled omental patch repairs (8). The results were sealed inside envelopes and were randomly selected according to a computer-generated schedule.
Preoperatively, all patients received intravenous fluids, nasogastric tube decompression, parenteral analgesics, antibiotics, usual dosages of a proton pump inhibitor, and deep vein thrombosis prevention. The postoperative period saw the continuation of these measures. The two procedures were carried out by an experienced group of senior surgeons (open and laparoscopic).
All patients were positioned in a somewhat reversible Trendelenburg posture for the laparoscopic procedure. To allow the patient to change positions freely, straps around the chest and legs were fixed. Depending on the primary surgeon's preference, the patient's position was either between the patient's legs or on the left side of the patient. The first phase of the method to confirm the diagnosis was an exploration of the peritoneal cavity.
The measurement of the size of the ulcer was done in relation to the active laparoscopic tool. Depending on the diameter, a few stay sutures using absorbable sutures were placed through the healthy tissue. The stitches were knotted securely over the omental patch, as indicated in the figure after an omental patch had been applied over the ulcer location.
The ulcer edges were clipped as a biopsy when a stomach perforation was discovered. Both the air-fluid leakproof test and the methylene blue test were applied as necessary. Under direct observation,
careful peritoneal lavage with (2–6) liters of warm normal saline was carried out to thoroughly cleanse the peritoneal cavity, careful peritoneal cavity draining using one to three drains, depending on the level of peritoneal pollution. The decision to switch from a laparoscopic to an open approach was either made by the primary surgeon due to technical challenges or recommended by the anesthesia team because of cardiopulmonary instability.
The Mannheim Peritonitis Index (MPI), which was created to predict fatality in cases with secondary peritonitis (9), is used to evaluate several intraoperative parameters, including the location and diameter of the perforation, nature of the peritoneal fluid (clear, purulent, pus), amount of lavage fluids, and operative time (minutes). Clinical evaluation of the patient’s postoperative recovery allowed for post-operative monitoring (Examination of the chest and abdomen, vital signs, urine production, drain volume, and fluid nature).
When bowel movement resumed, the nasogastric tube was removed, and the patients were then given permission to sip oral fluids before having complete oral intake as tolerated. To determine the nature of the stomach ulcer, a biopsy that was collected was histopathologically examined (peptic or malignant). To eliminate Helicobacter pylori, a two-week course of triple therapy with (Omeprazole, Tinidazole, and Clarithromycin) was administered, followed by an eight-week term of oral (PPI) medicine. Patients were released for follow-up in the outpatient department once they were pain-free, had no vomiting, were able to tolerate oral intake, and had no drains.
The endpoints of the study were conversion rate, operating time, postoperative discomfort, hospital stay duration, morbidities, and fatalities. Age, gender, length of symptoms, co-morbidities of the patients, prior abdominal surgeries, history of anti-ulcer therapy, history of NSAID use, presence of shock, preoperative data; operative data; MPI with its variables and post-operative data; postoperative analgesia requirement, surgical site infection (SSI), and morbidities. The proper approval was obtained as the study was ethically conducted in accordance with the Declaration of Helsinki.
Using SPSS version 26, statistical analysis of the collected data was performed. Descriptive statistics were computed and provided for continuous variables. Frequency distributions were used to explain categorical variables. An appropriate statistical test was employed to compare the outcomes. If the p-value was less than 0.05, the difference was deemed statistically significant.
Results
Our study comprised 160 individuals who were randomly assigned to laparoscopic or open exploration and had a clinical diagnosis of acute abdomen owing to GDP. After randomization, 82 candidates were included in the open group and 78 cases underwent a laparoscopic approach. Twenty patients were examined, and 12 from the laparoscopic cases (15.3%) and 8 from the open patients (9.7%) were eliminated because of the finding of other disorders (There were 6 cases with perforated diverticular disease of the colon and 2 cases with perforated cancer transverse colon, 4 ones with perforated cancer recto-sigmoid, 8 ones with perforated small intestine).
In the 66 cases in the laparoscopic group and the 74 cases in the open one that were included in the final analysis, the clinical diagnosis of GDP was verified. Table 1 displays the patient characteristics for the two groups. Regarding age, gender, the length of the symptoms, prior anti-ulcer medication, prior NSAID use, preoperative shock, co-morbidities, and past abdominal procedures, there were no statistically significant differences between the two groups.
Table 1 - Demographic data of the studied groups with ASA and Boey scores
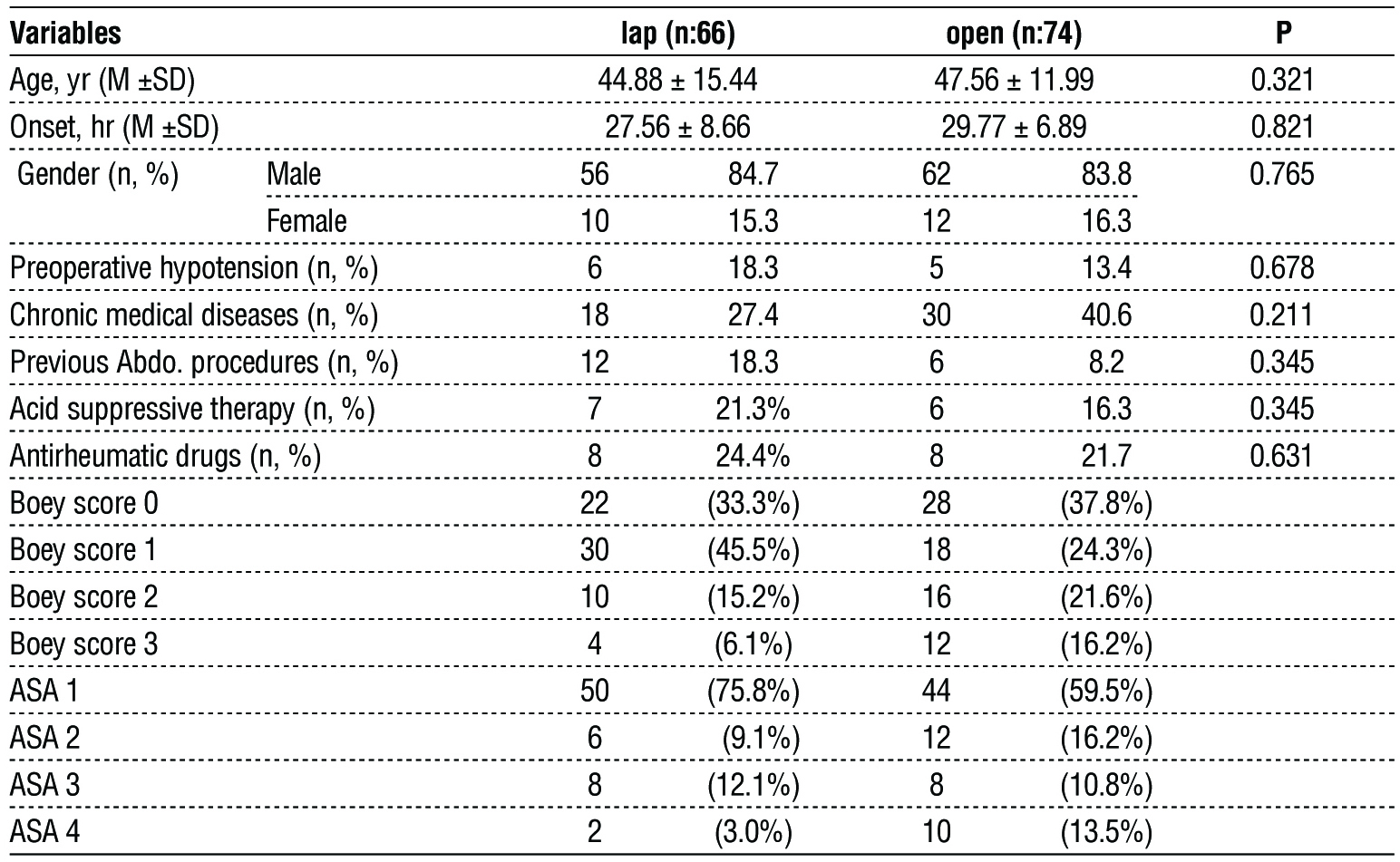
Preoperatively, the surgical risk was calculated for the patients who were included using the Boey score and the American Society of Anesthesiologists (ASA) score (table 1). No statistically significant difference in surgical risk between the two groups was found.
Apart from the distribution of gastric ulcers, which were more common in the open group, there were no statistically significant differences between the two groups in terms of the MPI, the mean size of the ulcers, or the location of ulcer distribution, as shown in table 2.
Table 2 - Size, location, and MPI of the ulcers in each group.

In this study, 15 cases (45.5%) underwent the first laparoscopic approach before switching to an open procedure. The etiology of conversion is shown in table 2. Following conversion to the open procedure, the converted cases were shifted to the open group, which reduced the sum of laparoscopic cases to 36 while increasing the number of patients in the open cases to 104. After conversion, the surgical risk was reevaluated in the two groups using the Boey score, ASA score, and MPI. By having a greater percentage of patients with Boey scores of 2 or 3 and a higher Mannheim Peritonitis index, as indicated in table 5, the cases in the open group had a higher surgical risk than those in the laparoscopic group.
The distribution of complications between the two groups was uneven. In the laparoscopic group, there were 10 complications (in 6 patients), whereas, in the open group, there were 10 complications (in 38 patients) (distributed as shown in table 3). Surgical site infection, several pulmonary problems, and wound dehiscence had the highest rates of sequelae.
Table 3 - Morbidities, fatalities, and the likelihood of reoperation in the groups.
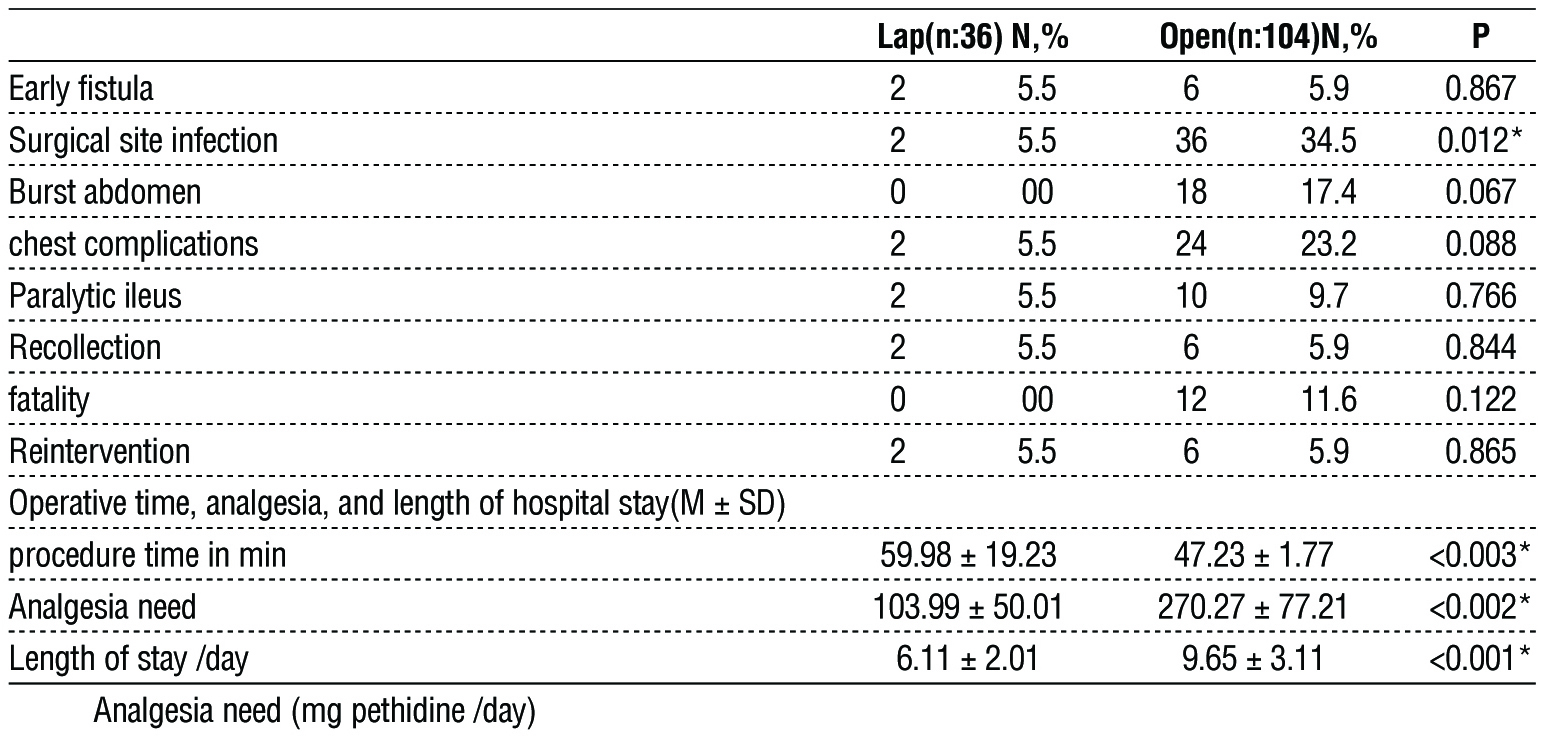
Table 3 demonstrates that, although not statistically significant, the incidence of leakage, ileus, intra-abdominal collections, and reoperation was lower in the laparoscopic cases than in the open ones. Eight patients had leakage (two underwent laparoscopic surgery and six underwent open surgery), and they were all treated with open re-exploration. Eight patients (two in the laparoscopic group and six in the open group) had intra-abdominal collections that were all treated with ultrasound-guided tube drainage.
In the group that underwent laparoscopic surgery, all the patients survived. On the other hand, there were 12 fatalities (11.5%) in the open group because of pulmonary issues, including pneumonia, sepsis, and multi-organ failure.
Table 3 shows that the completed operating time in the laparoscopic group was much longer than the open groups. According to the decreased daily analgesia required, postoperative pain in the laparoscopic cases was much lower than that in the open ones. In comparison to the open group, hospital stay of the laparoscopic group was dramatically reduced.
In this study, the converted group (30 patients) and the group that underwent successful laparoscopy were compared to establish the determinants of conversion (36 patients). Table 4 displays the patient characteristics for both groups.
Table 4 - Characteristics of the cases of converted and completed laparoscopy groups.
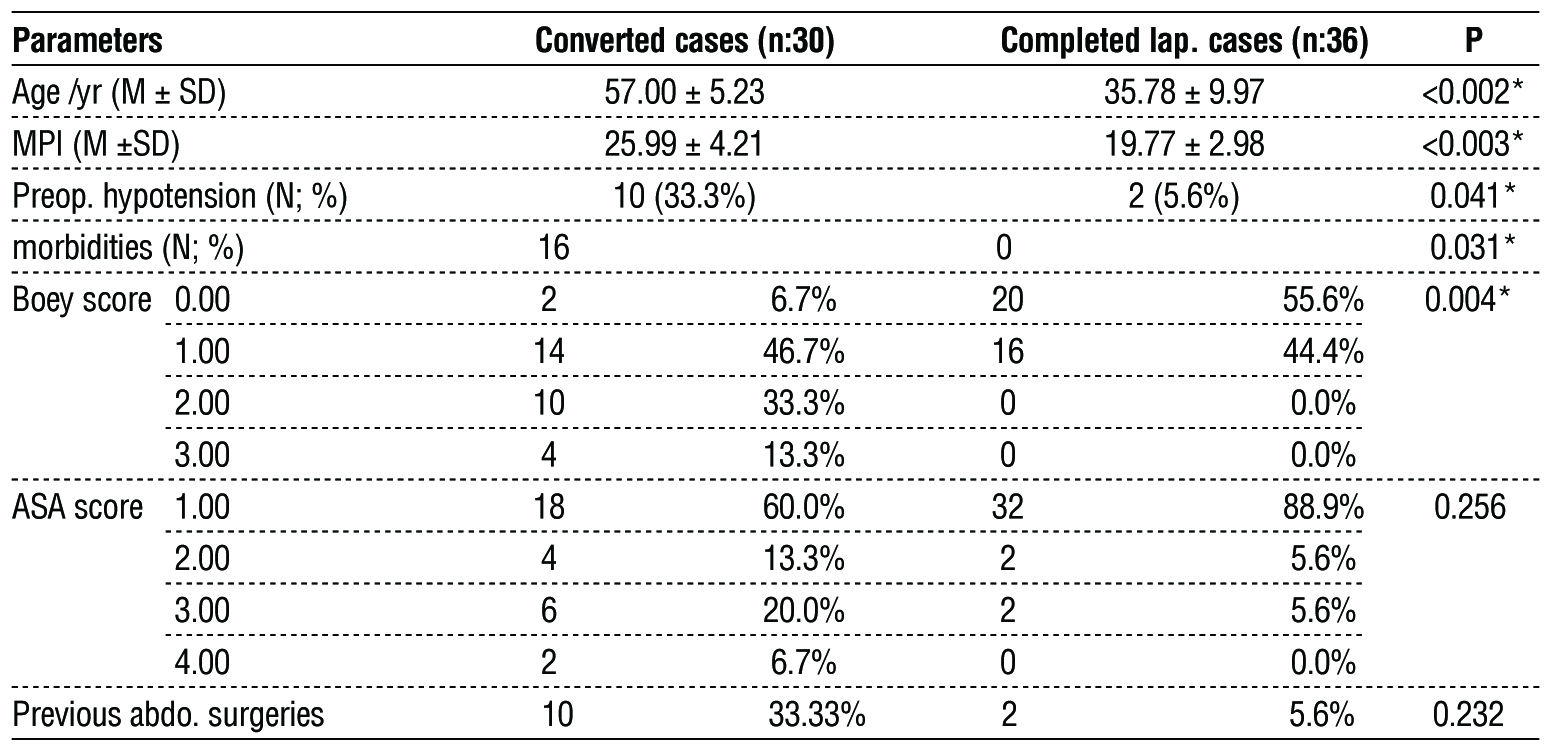
Table 4 demonstrates that the converted laparos-copy group had considerably higher rates of age, MPI, preoperative shock, co-morbidities, and Boey score, all of which were risk factors for conversion. The converted group also had a more delayed presentation than the completed laparoscopy group (35 versus 25 hours; respectively), however not reaching the level of statistical significance.
By calculating their odds ratios (OR) and 95% confidence intervals (95% CI) to establish the predictors for conversion, characteristics that had been found to be significant by univariate analysis were examined by multivariate analysis (stepwise logistic regression test). Following multivariate analysis, it was discovered that age and preoperative shock were predictors of conversion, as indicated in table 5.
Table 5 - Age, ulcer size, the risk for conversion, preoperative shock, and the MPI

The preoperative shock was present in 12 participants in the laparoscopic group in this study. Only two patients successfully finished the laparoscopic approach, while ten of them were switched to the open technique.
Discussion
Since Mouret et al. (1990) performed the first laparoscopic repair of a perforated peptic ulcer, numerous clinical trials across the globe have proved the viability and safety of the procedure (4,10). Regarding the actual advantages of laparoscopic repair over open repair, there is still considerable debate. The goal of the current prospective randomized trial was to compare the usual open approach to laparoscopic GDP repair to determine its feasibility and safety.
All patients admitted to our centers during a 48-month period with a clinical diagnosis of perforated peptic ulcer were included in this study. Of the 160 patients, 20 were removed from this study because of their additional pathologies. As a result, 66 individuals underwent the laparoscopic operation and 74 underwent the open procedure.
Age, sex, the length of the symptoms, preoperative shock, co-morbidities, prior abdominal surgeries, Boey score, and ASA grade were equivalent between the two groups of patients in our study after randomization. In contrast to the retrospective study, the results are more reliable due to the comparable patient features in the two groups (11), where the authors chose 222 patients (60 in the laparoscopy group and 162 in the open group). According to the Boey score and ASA grade, the patients in their study who were part of the open group were considerably of older ages, delayed presentations, and surgical risks, which caused their findings to be biased in favor of the laparoscopic approach.
In the current study, the rate of conversion from laparoscopic to open procedure was 45.5%, which was better than the work done in their prospective analysis, which showed a conversion rate of up to (60%)(12). Additionally, it was higher than the 28.5 percent conversion rate that was reported in their prospective nonrandomized trial of 374 patients (155 laparoscopic versus 219 open)(13). In our study, only a small number of patients were randomly assigned to each of the two groups due to the learning curve, as opposed to the selective and non-randomized design of previous studies, which can be blamed for the higher conversion rate.
Despite the low insufflation pressure and low flow rate that was used, the most frequent cause of conversion in the current investigation was cardio-pulmonary distress after initiating insufflation (21.2%). In individuals with severe co-morbidities, the preoperative septic shock had been used to explain this cardiovascular instability. This was in line with a prior retrospective study (10) that found cardiovascular instability to be the main factor leading to conversion.
Failure to adequately drain the peritoneal cavity accounted for the second cause of conversion in our study due to severe intraperitoneal adhesions, heavy pyogenic membranes because of the delayed presentation, and considerable ileus. These factors rendered the surgery technically challenging and time consuming, which was inappropriate for patients with such severe sepsis. These results were in line with those from the retrospective analysis, which involved 114 patients who underwent laparoscopic repair and had a 25% conversion rate (14).
Despite the much longer surgical duration in the converted group, there was no discernible difference in the frequency of postoperative morbidities or fatalities between that group and the one that began exploration by open technique. This was in line with the findings of a prospective non-randomized trial (15), which comprised 156 cases for laparoscopic repair and had a conversion rate of (27%). The authors attributed this less favorable outcome to the higher hole size in the converted group and technological challenges. They highlighted that conversion lengthened operations, raised costs, and scars left at trocar locations.
Age, preoperative shock, a high Boey score, a high MPI, and co-morbidities all significantly increased the probability of conversion in the current study, according to the univariate analysis. However, only preoperative shock and advanced age were found to be predictive of conversion by multivariate analysis. Comparable research involved 46 patients (30 underwent laparoscopic procedures versus 16 who underwent open suture repairs) in a non-randomized prospective analysis with a 17% conversion rate. Preoperative shock raised the conversion rate up to 50% against 8% in patients with hemodynamic stability, according to reports (13,16).
By using multivariate analysis, this study showed that age was a statistically important predictor of conversion. This conclusion can be explained by the higher prevalence of severe co-morbidities in this age group, which had a negative impact on the general health of the patients and, consequently, their readiness for anesthesia during laparoscopy and delayed presentation. Contrarily, much earlier research did not include the impact of age on the rate of conversion (4,16).
According to Lee et al. (2001), the Boey score was found to be a predictor of conversion (Boey scores of 1, 2, and 3 points, respectively, resulting in 21.4%, 30.2%, and 81.8% conversion rates)(17). The multivariate analysis failed to approach significance as a predictor of conversion, despite the fact that the Boey score in our study was significantly higher in the converted laparoscopy group (Boey score 2, 3) than in the completed laparoscopy group (Boey score 0, 1). The lack of patients in the laparoscopy group can be used to explain this.
With a varying cut-off limit between research, some investigations had found ulcer size as a predictor for conversion (8-10 mm)(4,16). On the other hand, the conversion rate in our study was unaffected by the size of the ulcer, which can be attributed to the fact that the procedure used (pedicled omentoplasty) was effective for treating all types of ulcers.
The operating time of the completed laparoscopy group (61 min) was equivalent to the reported operating time of roughly 65 min of the prospective study (13). This can be due to the smaller patient population and the better laparoscopic capabilities of our center.
The peritoneal lavage with a considerable amount of warm saline (2-6 liters) intended to clear deep peritoneal recesses can be used to explain why operations took longer to complete in the laparoscopy group. Another significant factor was the intra-corporeal stitching, which took longer, particularly if the edges of the perforation were friable. These factors were equivalent to the factors mentioned in earlier studies (13,16).
As seen by the lower postoperative analgesia needs, this study showed that postoperative pain in the successfully performed laparoscopic group was much lower than that in the open group. This can be explained by the minimally invasive design of the laparoscopes and low degree of tissue stress. This was in line with the findings of other earlier studies (4,16).
In comparison to the open group, the laparoscopic group had a much lower rate of wound infection.
This was due to the septic peritoneal material contaminating big abdominal incisions during open exploration. This outcome was in line with the majority of the other research findings (16-19). However, only a small number of patients (60 open vs. 32 laparoscopic) were included in this study.
In this study, the open group experienced a high incidence of abdominal wall dehiscence (17.3%), whereas there was no wound affection in the laparoscopic group. This difference can be attributed to the higher rate of SSI (34.6%) that affected large laparotomy incisions in this group of patients with
compromised general health. This was in line with the findings of other studies, which demonstrated a lower incidence of wound dehiscence in the laparoscopic cases compared to the open one, but not statistically significantly lower rates (13,19).
In this study, the laparoscopic group experienced less leakage than the open approach, however, the difference was statistically insignificant. This was consistent with the research, which showed that the open group saw a leakage rate of roughly 6% whereas the laparoscopic group experienced no suture site leak at all (20).
In our study, the rate of pulmonary complications was lower in the laparoscopic approach (5.6% vs. 23% in the open group - but a statistically insignificant lower rate. The possible causes were the smaller patient population, delayed presentation, and higher frequency of co-morbidities in the open approach (8 cases of COPD in the open approach compared to 0 in the laparoscopic one). This was similar to previous research (21).
Though not statistically significant, the rate of intra-abdominal collections was lower in the laparoscopic approach than in the open one. This can be explained by the successful irrigation of the laparoscopic procedure and draining of the peritoneal cavity, which reaches deep peritoneal recesses. This was in line with the findings of another study which showed that laparoscopy had a lower risk of intraabdominal collection than open surgery (n=2/66 vs. n=4/68) (22).
This study showed that, although not statistically significant, the rate of ileus was lower in the laparoscopic approach than in the open one. When compared to the open approach, this was explained by greater abdominal cavity drainage with less manipulation.
This was in line with the findings of several earlier investigations (18).
There were no deaths in the laparoscopic group in this trial, whereas there were 12 deaths (11.5%) in the open approach, a result that was statistically significant. Older age, concomitant co-morbidities, late presentation, and severe sepsis of the open group, which explained the greater fatality rate, were not connected to the procedure itself. This was in line with the earlier work that was done (19).
In this study, the hospital stay of the laparoscopic group was dramatically reduced compared to the open (6.11 ± 2.01 versus 9.65 ± 3.11) one. This was similar to the findings of other earlier investigations (14,23).
The cosmetic results of the laparoscopic operation are one advantage. This was mentioned in several earlier research (10,13). Due to the increased rates of SSI, wound dehiscence, and lengthy laparotomy incisions with consequent unsightly scars in the open approach of our experience, there was a significant difference in the cosmetic outcome between the laparoscopic and open approaches.
In our analysis, only two patients with laparoscopy and six patients with open surgery required additional exploration due to leakage that was clearly present. This was in line with the findings of the study by Bertleff et al., 2009, in which only one case underwent a laparoscopy, and two cases underwent an open procedure (13).
There are a lot of drawbacks to this study, namely the learning curve and the small number of patients enrolled. Future multicentric prospective randomized studies are required to verify the results of this study, especially the predictors of conversion. These studies with larger number of included patients may prove other risk factors detected by the univariate analysis like Boey score, Mannheim peritonitis index and co-morbidities to be independent predictors of conversion which will help for better selection of patients for laparoscopic repair and decrease the rate of conversion.
Conclusion
In patients with low surgical risk, laparoscopic repair of a GDP is equally viable and safe as the open repair (Boey score 0 and 1). For eligible individuals, laparoscopic repair of a perforated peptic ulcer has many benefits in comparison with the open repair; (lower postoperative pain, lower incidence of postoperative morbidities, better cosmetic outcome, earlier recovery, and shorter hospital stay). Old age, severe co-morbidities, high Boey score, high Mannheim peritonitis index, and preoperative shock are risk factors for conversion. Preoperative shock and old age are specifically independent predictors for conversion.
Clinical significance
In individuals with low surgical risk, laparoscopic repair is as possible and secure as compared to open repair (Boey score 0 and 1). Laparoscopic repair has multiple advantages in comparison with open repair. Laparoscopic repair of a perforated peptic ulcer has many benefits in comparison with open repair (lower postoperative pain, lower incidence of postoperative morbidities, better cosmetic outcome, earlier recovery, and shorter hospital stay).
Conflicts of interest: none
Funding: none.
Availability of data and materials: available.
References
1. Chung KT, Shelat VG. Perforated peptic ulcer - an update. World J Gastrointest Surg. 2017;9(1):1-12.
2. Albaqawi ASB, El-Fetoh NMA, Alanazi RFA, Alanazi NSF, Alrayya SE, Alanazi ANM, et al. Profile of peptic ulcer disease and its risk factors in Arar, Northern Saudi Arabia. Electron Physician. 2017; 9(11):5740-5745.
3- Tarasconi A, Coccolini F, Biffl WL, Tomasoni M, Ansaloni L, Picetti E, et al. Perforated and bleeding peptic ulcer: WSES guidelines. World J Emerg Surg. 2020;15:3.
4. Siu WT, Leong HT, Law BK, Chau CH, Li AC, Fung KH, et al. Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial. Ann Surg. 2002;235(3):313-9.
5. Gurusamy KS, Cassar Delia E, Davidson BR. Peritoneal closure versus no peritoneal closure for patients undergoing non-obstetric abdominal operations. Cochrane Database Syst Rev. 2013;2013(7): CD010424.
6- Boey J, Choi SK, Poon A, Alagaratnam TT. Risk stratification in perforated duodenal ulcers: a prospective validation of predictive factors. Ann Surg. 1987;205:22-6.
7- Doyle DJ, Hendrix JM, Garmon EH. American Society of Anesthesiologists Classification. [Updated 2022 Dec 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/ NBK441940/
8. Cellan-Jones CJ. A rapid method of treatment in perforated duodenal ulcer. BMJ. 1929;36:1076-7.
9. Muralidhar VA, Madhu CP, Sudhir S, Srinivasarangan M. Efficacy of Mannheim Peritonitis Index (MPI) Score in Patients with Secondary Peritonitis. J Clin Diagn Res. 2014;8(12):NC01-3.
10. Lagoo SA, Pappas TN. Laparoscopic repair for perforated peptic ulcer. Ann Surg. 2002;235(3):320-1.
11. Mirabella A, Fiorentini T, Tutino R, Falco N, Fontana T, De Marco P, et al. Laparoscopy is an available alternative to open surgery in the treatment of perforated peptic ulcers: a retrospective multicenter study. BMC Surg. 2018;18(1):78.
12. Kim CW, Kim JW, Yoon SN, Young Oh B, Mo Kang B. Laparoscopic repair of perforated peptic ulcer: a multicenter, propensity score matching analysis. BMC Surg. 2022;22(1):230.
13. Bertleff MJ, Lange JF. Laparoscopic correction of perforated peptic ulcer: first choice? A review of literature. Surg Endosc. 2010;24(6): 1231-9.
14. Thorsen K, Glomsaker TB, von Meer A, Søreide K, Søreide JA. Trends in diagnosis and surgical management of patients with perforated peptic ulcer. J Gastrointest Surg. 2011;15(8):1329-35.
15. Lee DJ, Ye M, Sun KH, Shelat VG, Koura A. Laparoscopic versus Open Omental Patch Repair for Early Presentation of Perforated Peptic Ulcer: Matched Retrospective Cohort Study. Surg Res Pract. 2016;2016:8605039.
16. Lau JYW, Barkun A, Fan DL, Ernst J Kuipers, Yun-sheng Yang, Francis K L Chan. Challenges in the management of acute peptic ulcer bleeding. Lancet. 2013;381:2033–43.
17. Lee FY, Leung KL, Lai BS, Ng SS, Dexter S, Lau WY. Predicting mortality and morbidity of patients operated on for perforated peptic ulcers. Arch Surg. 2001;136(1):90-4.
18. Lunevicius R, Morkevicius M, Stanaitis J. Prakiurusiu dvylikapirstes zarnos opu laparoskopines operacijos ir ankstyvieji gydymo rezultatai bei komplikacijas itakojantys veiksniai [Laparoscopic repair of perforated duodenal ulcer: early postoperative results and risk factors]. Medicina (Kaunas). 2004;40(11):1054-68.
19. Lunevicius R, Morkevicius M. Risk factors influencing the early outcome results after laparoscopic repair of perforated duodenal ulcer and their predictive value. Langenbecks Arch Surg. 2005; 390(5):413-20.
20. Wang YH, Wu YT, Fu CY, Liao CH, Cheng CT, Hsieh CH. Potential use of peptic ulcer perforation (PULP) score as a conversion index of laparoscopic-perforated peptic ulcer (PPU) repair. Eur J Trauma Emerg Surg. 2022;48(1):61-69.
21. Celik S, Y?lmaz EM. Effects of Laparoscopic and Conventional Methods on Lung Functions in Colorectal Surgery. Med Sci Monit. 2018;24:3244-3248.
22. Paik PS, Towson JA, Anthone GJ, Ortega AE, Simons AJ, Beart RW Jr. Intra-abdominal abscesses following laparoscopic and open appendectomies. J Gastrointest Surg. 1997;1(2):188-92; discussion 192-3.
23. Naesgaard JM, Edwin B, Reiertsen O, Trondsen E, Faerden AE, Rosseland AR. Laparoscopic and open operation in patients with perforated peptic ulcer. Eur J Surg. 1999;165(3):209-14.
24. Critchley AC, Phillips AW, Bawa SM, Gallagher PV. Management of perforated peptic ulcer in a district general hospital. Ann R Coll Surg Engl. 2011;93(8):615-9.
Full Text Sources:
Abstract:
Views: 4381

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.