Surgery, Gastroenterology and Oncology
Official journal of the International Association of Surgeons, Gastroenterologists and Oncologists
|
|
The Impact of the ERAS Protocol on Laparoscopic Gastric Cancer Surgery in the West. A Retrospective Study
ABSTRACT
Background: We determined the feasibility of the ERAS protocol in laparoscopically operated patients for early and advanced gastric cancer.
Methods: Fifty-eight patients were included in the study (19 in the ERAS and 39 in the CC group). In both groups, only laparoscopic technique was used. Postoperative recovery parameters and serum CRP levels were compared.
Results: The CC group had significantly more complications (0% in the ERAS vs. 25.6% in the CC group; p=0.018). Patients in the ERAS group had a significantly shorter hospital stay (8.5±2 days in the ERAS vs. 11.3±4 days in the CC; p=0.002) and significantly lower pain scores on days one to three compared to the CC. The total medical cost was higher in the ERAS group (p<0.0001). The multivariate logistic regression model identified shorter hospital stay (HR: 0.567; 95% CI: 0.326-0.985; p=0.044), and lower pain scores on day one (HR: 0.12; 95% CI: 0.022-0.662; p=0.015) and two (HR: 0.134; 95% CI: 0.026-0.693; p=0.017), as significantly related to the ERAS protocol.
Conclusion: ERAS protocol is feasible for laparoscopic gastrectomy. It reduces postoperative pain on days one and two which allows faster mobilization and earlier discharge.
Key words: ERAS protocol, laparoscopy, gastric cancer
INTRODUCTION
The success of the enhanced recovery after surgery (ERAS) protocol in major abdominal operations has been widely acknowledged (1). Reports from ERAS implementation in colorectal surgery reported favourable results in terms of faster recovery of the bowel function, less postoperative pain, reduced postoperative morbidity and mortality, shorter hospital length as well as lower costs and postoperative inflammatory response (1). These results have sparked the desire to achieve the same goals in gastric cancer surgery. Indeed, the first studies confirmed many benefits compared to the conventional care surgery (2-5). However, only open approach was used in the first reports. Meanwhile, laparoscopic surgery has become an established part of gastric cancer treatment with proven benefits for patients (6-11). Laparoscopy reduces the tissue trauma and postoperative pain as well as speeds up recovery (6-11). Studies have only recently begun to take laparoscopic gastrectomy combined with the ERAS protocol into account, albeit they did not exclude open surgery (2-5). This makes an assessment of the impact of the ERAS protocol difficult. As the experience has grown in the field of laparoscopic gastric cancer surgery, studies comparing the results of the ERAS protocol only in laparoscopically operated patients have begun to emerge (12-18). Results from these publications confirm the benefits of the ERAS protocol combined with laparoscopy. However, some authors question the generalisation of these results (21). These studies have almost exclusively been performed in Asiatic countries where patients are younger, in better general shape, often include only early gastric cancer and have lower BMI compared to their Western counterparts (12-18). Additionally, most studies excluded patients with perioperative chemotherapy (12-18), whereas, according to ESMO guidelines, most Western patients are candidates for perioperative treatment (19). Consequently, the results from the current studies cannot be generally applied to Western patients. The aim of the present study was to determine the value of the ERAS protocol in patients with early and advanced gastric cancer operated with laparoscopic gastrectomy at a Western medical centre.
METHODS
Patients and ethical consideration
Before operation, a written informed consent was obtained from the patients. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University Medical Centre Maribor, Slovenia. The study was registered under the code UKC-MB-KME-74/20. Patients with histologically confirmed gastric cancer were included in the study. The inclusion criteria were as follows: i) a preoperative gastric cancer stage of any T, any N, M0; ii) no previous upper abdominal surgery; iii) laparoscopic surgery; iv) normal haematological, renal, hepatic, and cardiac parameters; v) ASA ? 3. Exclusion criteria were as follows: i) history of cancer; ii) presence of acute infection; iii) gastric cancer infiltrating other organs or causing obstruction. Patients were diagnosed between May 2015 and October 2020. Before operation, each patient was discussed at the local tumour board. Patients with preoperative stage Ib or higher were scheduled for perioperative chemotherapy. In the final group, 57 patients were included. While 39 patients received conventional perioperative care and laparoscopic surgery (CC), 11 received the ERAS rehabilitation program and laparoscopic surgery (ERAS).
Operation and treatment
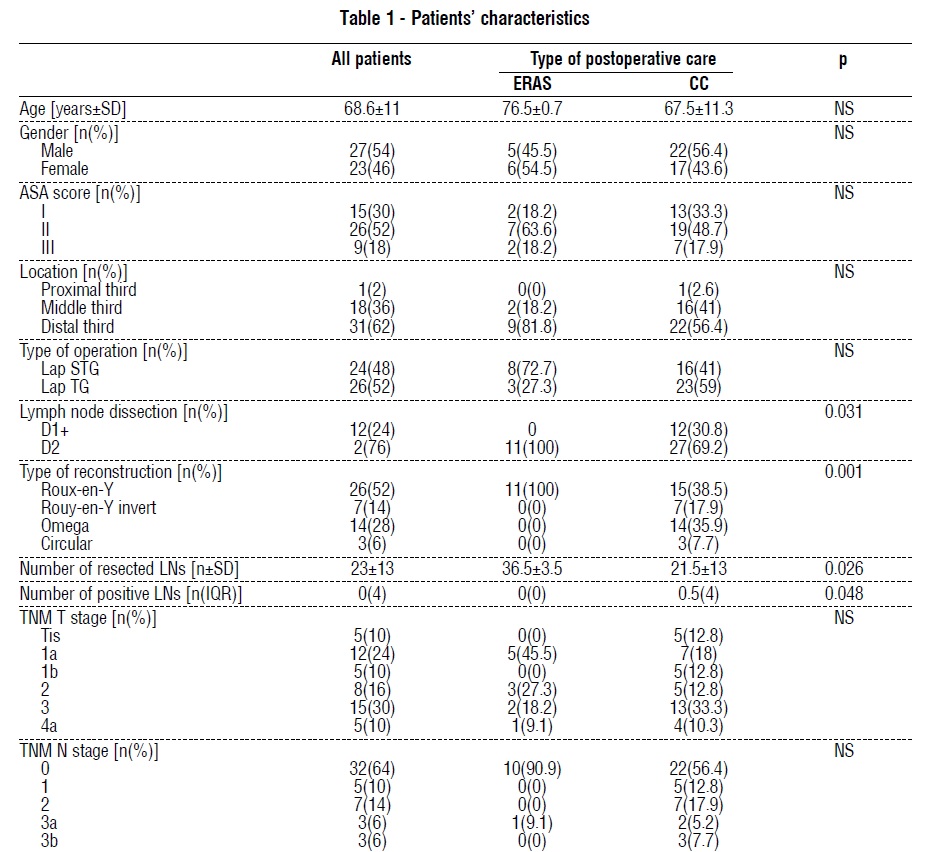
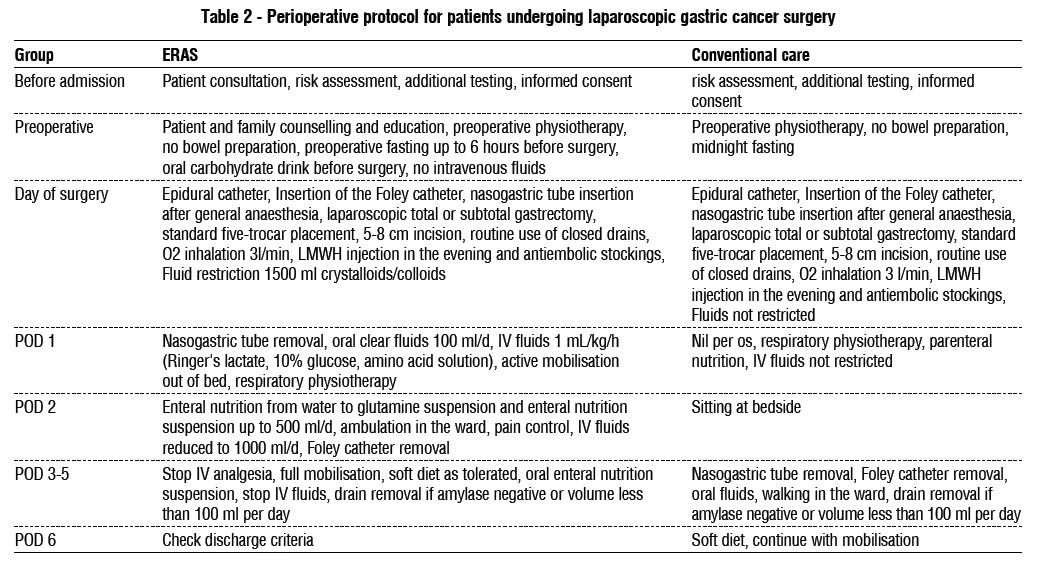
All patients were operated by the same team of surgeons experienced in laparoscopic gastric cancer surgery. A totally laparoscopic total or subtotal gastrectomy was performed in all the included patients. The proportion of laparoscopic operations and types of reconstruction is presented in table 1. The elements of the ERAS protocol were developed according to ERAS consensus guidelines for gastric cancer (2). Details of the ERAS and conventional care protocols are listed in table 2. Patients in the ERAS group were educated before the surgery at the outpatient clinic. Patients were admitted 2 days before surgery. They were allowed to consume a normal diet up to 6 hours before operation. A carbohydrate-rich drink was allowed until 2 hours before surgery. Patients received no preoperative bowel preparation. Before operation, no nasogastric tube was inserted. On the day of the surgery, an epidural catheter was inserted. Patients in the ERAS group received additional postoperative anti-inflammatory drugs twice a day. Nasogastric tubes were removed on POD1 (post-operative day one), and they were allowed to sip clear fluid and a glutamine-rich drink. They began with early mobilisation. On POD1, they were encouraged to sit and perform respiratory rehabilitation; on POD2, they were encouraged to stand with help; on POD3, they began to walk. The postoperative intravenous fluids were gradually tapered off until POD3 or 4 when they received a soft diet. Patients were discharged when fully ambulatory, when they required no intravenous analgesia, or when with afebrile status. After discharge, they were regularly followed-up on outpatient clinic. All surgery was performed by the same experienced laparoscopic team. Depending on the location of the tumour, either a total or a subtotal laparoscopic gastrectomy was performed. The laparoscopic technique was described elsewhere (28, 29). The intestinal continuity was reconstructed with either Billroth II or Rouxen- Y anastomoses. The lymphadenectomy was performed in accordance with the Guidelines of Japanese Gastric Cancer Association (27). For early gastric cancer, a D1+ lymphadenectomy was sufficient; for all other stages, a D2 lymph node dissection was performed. The extraction of the specimen and the intestinal reconstruction were performed through a 5 to 8 cm supraumbilical midline incision. Drains were routinely placed in the right subhepatic and left subdiaphragmal space.
Study endpoints
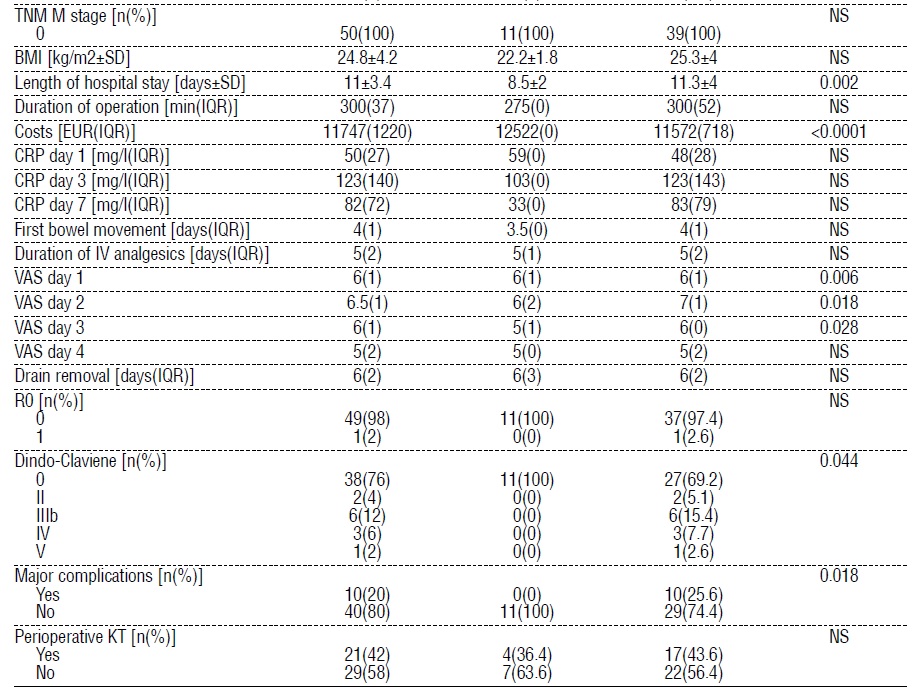
Primary study endpoints were the length of the postoperative hospital stay, postoperative pain measured by the visual analogue scale (VAS) on days one to four, time to first defecation, duration of intravenous analgesics and the complication rate. Secondary endpoints were the costs of hospitalisation, postoperative systemic inflammatory response measured with serum CRP levels on days one, three and seven and the 30-day readmission rate.
Statistical analysis
Continuous variables were presented as mean ± SD for normally distributed variables and as median (IQR) for continuous variables without normal distribution. Discrete variables were presented as absolute number (percentage). Depending on the distribution, continuous variables were compared with Student’s t-test and Mann-Whitney’s U-test. Normality was tested with the Kolmogorow’s and Smirnoff’s test for normality. The discrete variables were compared with the 2 test of the Fisher’s exact test. The level of significance was the p value of 0.05 or less. All analyses were performed with the SPSS v. 22.0 (IBM, Chicago, IL, USA).
RESULTS
A total of 58 consecutive patients who underwent laparoscopic gastrectomy from January 2015 to October 2020 were included in the study. The baseline characteristics of the included patients are summarized in table 1. There was no significant difference in the distribution of patients’ characteristics between the ERAS and CC groups. Tumours in both groups were mostly located in the distal third of the stomach. In both groups, the same proportion of patients received perioperative chemotherapy (47.4% in the ERAS group vs. 43.6% in the CC group; p = 0.741).
Most of the patients in the ERAS group received a laparoscopic distal subtotal gastrectomy [16(84.2)]. In the CC group, significantly more patients received a laparoscopic total gastrectomy [23 (59); p = 0.002]. All patients in the ERAS group received a D2 lymphadenectomy compared to 69.2% of patients in the CC group (p = 0.012). The average number of dissected lymph nodes was significantly higher in the ERAS group (28±9 LNs in the ERAS vs. 19.9±13 LNs in the CC; p = 0.026). there was no significant difference in the number of positive LNs between groups. In all patients in the ERAS group, a Roux-en-Y reconstruction was used. In most cases in the CC group, Roux-en-Y reconstruction was used followed by Omega loop. A circular stapler was used in the CC group only in three cases. Operation time ways significantly shorter in the ERAS group [260 (112) min in ERAS vs. 300(40) min in CC; p = 0.025]. In both groups, we observed no 30-day mortality. The ERAS group had no morbidity and no mortality. Patients in the CC group had significantly more complications. In the CC group, major complications needing any form of intervention were observed in 25.6%. Between the ERAS and CC groups, there was no significant difference in the TNM distribution. However, in 12.8% of the included patients in the CC group the histology revealed a carcinoma in situ, while there was none in the ERAS group. Slightly less cases of early carcinoma was observed in the CC group compared to the ERAS group (42.1% in the ERAS vs. 30.8% in the CC; p = 0.862). There was no significant difference in the rate of R0 resection between groups. Patients in the ERAS group had a significant shorter hospital stay compared to the CC group (7.5(4) days in the ERAS vs. 11(6) days in the CC; p = 0.003). For patients in both groups, the time to first bowel movement was similar and needed IV analgesic treatment was similar. However, patients in the ERAS group had significantly smaller pain scores derived from VAS on days one to three. Total medical costs were significantly higher in the ERAS group (p < 0.0001). There were no significant differences in the 30-day readmission rate between groups (15.8% in both groups). The readmission rate in the patient group less than 65 years was 0% in the ERAS and 5.3% in the CC group. this difference was not significant. In both groups, differences in the postoperative stress responses measured with the serum levels of CRP on day one, three and seven were not significantly different. Even so, a faster return to baseline levels was observed in the ERAS group compared to the CC group. This difference did not reach the level of significance.
Subgroup analysis
In the subgroup analysis, only patients with no morbidity were compared for postoperative recovery results. Eleven patients from the ERAS group were compared to 27 patients in the CC group. After we excluded patients with postoperative morbidity, the length of hospital stay was only insignificantly longer in the CC group (p = 0.078). Patients in the ERAS group had a mean of 2-day shorter hospital stay. Total medical costs were higher in the ERAS group (p < 0.0001). The time to first bowel movement and duration of IV analgesia was similar, while the pain scores derived from VAS on days 1 to 3 were significantly less in the ERAS group. Values of postoperative stress indicators were similar in both groups. In the ERAS group, we again noticed an insignificantly faster recovery of postoperative serum CRP levels to baseline. Because of the small number of laparoscopic total gastrectomies in the ERAS group only a meaningful analysis of the subgroup with laparoscopic subtotal gastrectomy could be performed. In the subgroup of patients with laparoscopic subtotal gastrectomy patients in the ERAS group had more extracted lymph nodes per operation (27.7±9 LNs in ERAS vs. 16±13 LNs in CC; p = 0.009), shorter operation times (220(90) min in ERAS vs. 320(103) min in CC; p = 0.012), higher hospital costs (12479(69) EUR in ERAS vs. 11287(364) EUR in CC; p <0.0001), lower values of CRP on day seven (53(0) mg/ml in ERAS vs. 107(71) mg/ml in CC; p = 0.002), lower pain scores on days one to three compared to patients in the CC group (5(1), 5(2) and 5(6) in ERAS vs. 6.5(1), 7(2) and 6(1)in CC; p = 0.009, 0.011 and 0.024). In the ERAS group significantly more D2 lymphadenectomies were performed (16(100) in ERAS vs. 8(50) in CC; p = 0.003) and patients received exclusively a Roux-en-Y reconstruction (p < 0.0001). No significant differences were noted in the rate of conversions between groups. There were no complications in the ERAS group and significantly more proximal tumour location compared to patients in the CC group (p = 0.009). There were no significant differences in the duration of the hospital stay or the readmission rates between groups (table 3).


Multivarinate analysis
A forward stepwise conditional regression model was used to identify predictors significantly associated with the ERAS protocol. The multivariate logistic regression model identified hospital stay (HR: 0.567; 95%CI: 0.326-0.985; p = 0.044), and the pain scores on day 1 (HR: 0.12; 95%CI: 0.022-0.662; p = 0.015) and 2 (HR: 0.134; 95%CI: 0.026-0.693; p = 0.017) as significantly related to ERAS protocol.
DISCUSSION
Most of the present studies that evaluate the feasibility of the ERAS protocol after laparoscopic gastric cancer surgery were published in specialised Eastern centres, with fit patients capable to endure the strenuous ERAS protocol (17,25,26). Since there is avoid in studies evaluating the feasibility of the ERAS protocol after laparoscopic gastrectomy in the West, we performed a retrospective analysis comparing the results of laparoscopic gastrectomy of early and advanced gastric cancer patients combined with ERAS and conventional postoperative care at a Western centre.
Patients included in our study were older and had more accompanying diseases compared to studies published in the East (21-24). The age of patients included in RCTs by Sugisawa et al., Kang et al. and Mingjie et al. ranged from 56 to 64 years (17, 25, 26). The mean age of included patients in our study was 68 years. The majority of included patients had an ASA score of II or III. In addition, two thirds of patients in our study had advanced gastric cancer necessitating a more demanding laparoscopic total gastrectomy. This reflects the usual patient population seen in the West. Our results confirmed that even older patients satisfactorily complied with the ERAS protocol. Bu et al. reported that implementation of ERAS in older patients significantly increased the incidence of nausea, vomiting, gastric retention, and ileus (20). We did not observe such complications despite the older age of patients and the fact that nearly half of the patients received a total gastrectomy.
In the present study the multivariate logistic regression model related the ERAS protocol with shorter hospitalisation and smaller pain scores on days 1 and 2. Patients in the ERAS group had a significantly shorter hospital stay compared to the CC group. Similar results were reported from other RCTs (2-18, 25, 26) and meta-analyses (21-24). Contrary to the results from studies that included only the laparoscopic approach (2-18, 25, 26), we did not observe a faster recovery of bowel function nor did we observe a significant reduction of duration of IV analgesic use. The shorter hospital stay in our study thus could not be directly attributed to faster gut function recovery as reported elsewhere (21). On the other hand, we observed that pain scores derived from VAS on days 1 to 3 were significantly less in the ERAS group compared to the CC group in the univariate analysis.
Based on this finding, we propose that the ERAS protocol combined with minimally invasive surgery reduces the pain on first postoperative days which in turn allows faster mobilisation, especially on days 1 and 2. The mobilisation of patients on the first two days is critical, since it reduces the likelihood of respiratory complications that prolong the hospital stay (21). In order to achieve shorter hospitalisation, it is therefore prudent to strive for early full mobilisation. This is especially the case in elderly and frail patients who are more prone to secondary infections.
Moreover, elderly less ambulant patients feel reluctant to discharge from the hospital even if the pain score on days four and more might be low.
There are conflicting results regarding the readmission rates between the ERAS protocol and conventional care in the literature (20-25). Most of the initial papers reported higher readmission rates in patients after laparoscopic gastrectomy with ERAS protocol (20-24). Only recently papers have begun to emerge reporting exceedingly low readmission rates (25). This suggests that sufficient experience was necessary to reduce readmissions. The readmission rate in the present study was 15.8% and no statistical difference was found between the ERAS protocol and conventional care. Readmission rates presented in the present study might be higher than reported by Sugisawa et al. (0% readmission rate in both groups) (25). However, in their study only patients with an ECOG performance status of 0 were included (25). As shown by Bu et al. age and general performance are significant factors that predispose patients to readmission (20). When we excluded patients older than 65 years, we also did not observe any readmissions, which is in agreement with the observations made by Bu et al and results published by other Eastern studies (20-25).
No morbidity and mortality was observed in the ERAS group. Significantly more patients had complications in the CC group. In the CC group we observed minor complications (Dindo-Claviene
Complications prolong hospitalisation even if only
conservative treatment is necessary. To exclude the
confounding effect of complications on the length of
postoperative stay, we compared a subgroup of
patients with an uneventful postoperative course.
Surprisingly in the subgroup analysis of patients with no complications, patients in the ERAS group had significantly less pain on days one to three. While the hospital stay in the EARS group was shorter compared to the CC group, this difference did not reach the level of significance. In the subgroup analysis of patients who received laparoscopic subtotal gastrectomy we observed significantly higher lymph node yield per operation and shorter operating times in the ERAS group. The CRP levels on day seven and the pain scores on days one to three were significantly smaller in ERAS group. In spite of this no difference in the length of hospital stay was observed. This finding is in contrast to current published studies (21-24). Since laparoscopy itself reduces hospital stay compared to open surgery, we agree with Liu et al. that the statistical insignificance in such cases may be attributed to benefits of laparoscopic gastrectomy, leaving little room for improvement via the implementation of the ERAS protocol (23).
Total medical costs were significantly higher in the ERAS group. This finding stands in contrast to most other studies reporting that shorter hospital stays bring down cost (21-24). In our country, medical costs of hospital stay are cheap. The main bulk of costs are produced by the multimodal approach necessary for the ERAS protocol. The difference of hospital stay of two days is not enough to reduce costs of the multimodal approach. This highlights the importance of conducting ERAS studies in different countries. Medical systems differ from region to region and results cannot be extrapolated globally.
The inflammatory response after the ERAS protocol combined with laparoscopy was found by many authors to be reduced (16). The association of inflammatory response and the ERAS protocol is still not understood (21). Some evidence points that early postoperative nutrition strengthens the gut barrier (21). Nonetheless, we could not confirm lower CRP levels in the ERAS group in our study. The rise of serum CRP was smaller in the ERAS group and the levels fell faster compared to the CC group at discharge, but this did not reach the level of significance. We attributed this to the small sample size of the study.
Many critics are concerned with the oncological sufficiency of ERAS and laparoscopic treatment (18). In our study, all patents in the ERAS group had a R0 resection. In each case, a D2 lymph node dissection was performed, and the average number of extracted lymph nodes is comparable to other RCT that reported the lymph node yield (12-18). We could also show that perioperative treatment did not have any impact on the compliance of patients with the ERAS protocol or produce additional morbidity. Patients after preoperative course of chemotherapy are in worse general condition and have a poorer nutritional status. Our results prove that, despite chemotherapy, even elderly patients with early and advanced gastric cancer could be included in the ERAS protocol. In addition, the ERAS protocol involves key elements aimed at improving the nutritional status of patients. Patients after neoadjuvant treatment should benefit the most from this protocol. This was supported by our results.
Our study has some limitations. Since a small number in the ERAS group received a laparoscopic total gastrectomy, meaningful subgroup analysis to evaluate the feasibility of the ERAS protocol in laparoscopic total gastrectomy could not be performed in the present study. Further trials with more included patients will be necessary. Meanwhile, there was a significant difference in the type of intestinal continuity reconstruction between patients in the ERAS and CC group. It is therefore questionable whether ERAS patients fared better because of the reconstruction and to what extent the ERAS protocol was responsible. Secondly, it was a retrospective study; hence some bias in inclusion of patients might be present. Finally, the ERAS protocol advocates against the use of drains. Nevertheless, gastric cancer surgery is associated with a morbidity of up to 45%, therefore most authors report the use of abdominal drains, and only one study on ERAS in gastric cancer reported no use of drains (18).
CONCLUSION
In conclusion our results confirm that the ERAS protocol can be safely used in elderly patients with early and advanced gastric cancer. It reduces the hospital stay and pain scores on days one and two. The perioperative treatment did not influence the compliance of patients in the ERAS group. Patients benefit from laparoscopic surgery combined with the ERAS protocol and can tolerate the intense postoperative treatment even after adjuvant chemotherapy. The protocol reduces postoperative pain on days one and two which allows faster mobilization and shorter hospital stays. Although the results support the use of ERAS combined with laparoscopic subtotal gastrectomy in elderly patients with early and advanced gastric cancer, additional RCT conducted in specialised Western centres are needed to determine the value of the ERAS protocol in laparoscopic total gastrectomy in the West.
Authorship confirmation statement
All authors confirm that the results presented in this article is their own original work and that the information they provided on these pages are true.
Conflict of interest
All author declare that they have no conflict of interest.
Fundind statement
None declared.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University Medical Centre Maribor, Slovenia. The study was registered under the code UKCMB- KME-74/20.
REFERENCES
1. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J Surg. 2019;43(3):659-695.
2. Mortensen K, Nilsson M, Slim K, Schäfer M, Mariette C, Braga M, et al. Consensus guidelines for enhanced recovery after gastrectomy: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Br J Surg. 2014;101(10):1209-29.
3. Yamada T, Hayashi T, Aoyama T, Shirai J, Fujikawa H, Cho H et al. Feasibility of enhanced recovery after surgery in gastric surgery: a retrospective study. BMC Surg, 2014;14:41.
4. Liu XX, Jiang ZW, Wang ZM, Li JS. Multimodal optimization of surgical care shows beneficial outcome in gastrectomy surgery. JPEN J Parenter Enteral Nutr. 2010;34(3):313-21.
5. Wang D, Kong Y, Zhong B, Zhou X, Zhou Y. Fast-track surgery improves postoperative recovery in patients with gastric cancer: a randomized comparison with conventional postoperative care. J Gastrointest Surg, 2010; 14(4):620-7.
6. Park YK, Yoon HM, Kim YW, Park JY, Ryu KW, Lee WJ, et al. Laparoscopy-assisted versus open D2 distal gastrectomy for advanced gastric cancer. Ann Surg. 2018;267(4):638-645.
7. Son T, Hyung WJ. Laparoscopic gastric cancer surgery: Current evidence and future perspectives. World J Gastroenterol. 2016; 22(2):727-35.
8. Son T, Kwon IG, Hyung WJ. Minimally invasive surgery for gastric cancer treatment: Current status and future perspectives. Gut Liver. 2014;8(3):229-36.
9. Shi Y, Xu X, Zhao Y, Qian F, Tang B, Hao Y, et al. Long-term oncologic outcome of a randomized controlled trial comparing laparoscopic versus open gastrectomy with D2 lymph node dissection for advanced gastric cancer. Surgery. 2019;165(6): 1211-1216.
10. Best LMJ, Mughal M, Gurusamy KS. Laparoscopic versus open gastrectomy for gastric cancer (Review). Cochrane Database Syst Rev. 2016;3(3):CD011389.
11. Ding J, Liao GQ, Liu HL, Liu S, Tang J. meta-analysis of laparoscopyassisted distal gastrectomy with D2 lamph node dissection for gastric cancer. J Surg Oncol. 2012;105(3):297-303.
12. Hu JC, Jiang LX, Cai L, Zheng HT, Hu SY, Chen HB, et al. Preliminary Experience of Fast-Track Surgery Combined with Laparoscopy- Assisted Radical Distal Gastrectomy for Gastric Cancer. J Gastrointest Surg, 2012;16(10):1830-9.
13. Kim JW, Kim WS, Cheong JH, Hyung WJ, Choi SH, Noh SH. Safety and efficacy of fast-track surgery in laparoscopic distal gastrectomy for gastric cancer: a randomized clinical trial. World J Surg, 2012; 36(12):2879-87.
14. Sahoo MR, Gowda MS, Kumar AT. Early rehabilitation after surgery program versus conventional care during perioperative period in patients undergoing laparoscopic assisted total gastrectomy. J Minim Access Surg, 2014;10(3):132-8.
15. Abdikarim I, Cao XZ, Li SZ, Zhao XQ, Taupyk Y, Wang Q. Enhanced recovery after surgery with laparoscopic radical gastrectomy for stomach carcinomas. World J Gastroenterol, 2015; 21(47): 13339-44.
16. Liu G, Jian F, Wang X, Chen L. Fast-track surgery protocol in elderly patients undergoing laparoscopic radical gastrectomy for gastric cancer: a randomized controlled trial. Onco Targets Ther, 2016; 9:3345-51.
17. Kang SH, Lee Y, Min SH, Park YS, Ahn SH, Park DJ, et al. Multimodal Enhanced Recovery After Surgery (ERAS) Program is the Optimal Perioperative Care in Patients Undergoing Totally Laparoscopic Distal Gastrectomy for Gastric Cancer: A Prospective, Randomized, Clinical Trial. Ann Surg Oncol. 2018;25(11):3231-3238.
18. Li Y, Qiu J, Cao H. Application of enhanced recovery after surgery for patients with laparoscopic radical gastrectomy. Zhonghua Wei Chang Wai Ke Za Zhi. 2016;19(3):269-73.
19. Smyth EC, Verheij M, Allum W, Cunningham D, Cervantes A, Arnold D, ESMO Guidelines Committee. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27(suppl 5):v38-v49.
20. Bu J, Li N, Huang X, He S, Wen J, Wu X. Feasibility of fast-track surgery in elderly patients with gastric cancer. J Gastrointest Surg, 2015;19(8):1391-8.
21. Wee IJY, Syn NLX, Shabbir A, Kim G, So JBY. Enhanced recovery versus conventional care in gastric cancer surgery: a meta-analysis of randomized and non-randomized controlled trials. Gastric Cancer, 2019;22(3):423-434.
22. Li MZ, Wu WH, Li L, Zhou XF, Zhu HL, Li JF, et al. Is ERAS effective and safe in laparoscopic gastrectomy for gastric carcinoma? A meta-analysis. World J Surg Oncol, 2018;16(1):17.
23. Li Z, Wang Q, Li B, Bai B, Zhao Q. Influence of enhanced recovery after surgery programs on laparoscopy-assisted gastrectomy for gastric cancer: a systematic review and meta-analysis of randomized control trials. World J Surg Oncol. 2017;15(1):207.
24. Wang LH, Zhu RF, Gao C, Wang SL, Shen LZ. Application of enhanced recovery after gastric cancer surgery: An updated metaanalysis. World J Gastroenterol. 2018;24(14):1562-1578.
25. Sugisawa N, Tokunaga M, Makuuchi R, Miki Y, Tanizawa Y, Bando E et al. A phase II study of an enhanced recovery after surgery protocol in gastric cancer surgery. Gastric Cancer. 2016;19(3):961-7.
26. Xia Mingjie, Zhang Luyao, Tang Ze, Zhao Yin Quan, Wang Quan. Laparoscopic Radical Gastrectomy for Resectable Advanced Gastric Cancer Within Enhanced Recovery Programs: A Prospective Randomized Controlled Trial. J Laparoendosc Adv Surg Tech A, 2017;27(9):959-964.
27. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer, 2017; 20(1):1-19. 28. Jagric T. The impact of modifying the laparoscopic lymphadenectomy technique on the extent of lymphadenectomy in laparos-copically operated gastric cancer patients. A single-center study. Surgery and Surgical Endoscopy, 2019; 1(1): 19-25.
29. Jagric T. East meets West: the initial results of laparoscopic gastric cancer resections with Eastern principles in a single Western centre - a propensity score-matched study. Langenbecks Arch Surg. 2021; 406(8):2699-2708.
Full Text Sources:
Abstract:
Views: 3578

Background: We determined the feasibility of the ERAS protocol in laparoscopically operated patients for early and advanced gastric cancer.
Methods: Fifty-eight patients were included in the study (19 in the ERAS and 39 in the CC group). In both groups, only laparoscopic technique was used. Postoperative recovery parameters and serum CRP levels were compared.
Results: The CC group had significantly more complications (0% in the ERAS vs. 25.6% in the CC group; p=0.018). Patients in the ERAS group had a significantly shorter hospital stay (8.5±2 days in the ERAS vs. 11.3±4 days in the CC; p=0.002) and significantly lower pain scores on days one to three compared to the CC. The total medical cost was higher in the ERAS group (p<0.0001). The multivariate logistic regression model identified shorter hospital stay (HR: 0.567; 95% CI: 0.326-0.985; p=0.044), and lower pain scores on day one (HR: 0.12; 95% CI: 0.022-0.662; p=0.015) and two (HR: 0.134; 95% CI: 0.026-0.693; p=0.017), as significantly related to the ERAS protocol.
Conclusion: ERAS protocol is feasible for laparoscopic gastrectomy. It reduces postoperative pain on days one and two which allows faster mobilization and earlier discharge.
Key words: ERAS protocol, laparoscopy, gastric cancer
INTRODUCTION
The success of the enhanced recovery after surgery (ERAS) protocol in major abdominal operations has been widely acknowledged (1). Reports from ERAS implementation in colorectal surgery reported favourable results in terms of faster recovery of the bowel function, less postoperative pain, reduced postoperative morbidity and mortality, shorter hospital length as well as lower costs and postoperative inflammatory response (1). These results have sparked the desire to achieve the same goals in gastric cancer surgery. Indeed, the first studies confirmed many benefits compared to the conventional care surgery (2-5). However, only open approach was used in the first reports. Meanwhile, laparoscopic surgery has become an established part of gastric cancer treatment with proven benefits for patients (6-11). Laparoscopy reduces the tissue trauma and postoperative pain as well as speeds up recovery (6-11). Studies have only recently begun to take laparoscopic gastrectomy combined with the ERAS protocol into account, albeit they did not exclude open surgery (2-5). This makes an assessment of the impact of the ERAS protocol difficult. As the experience has grown in the field of laparoscopic gastric cancer surgery, studies comparing the results of the ERAS protocol only in laparoscopically operated patients have begun to emerge (12-18). Results from these publications confirm the benefits of the ERAS protocol combined with laparoscopy. However, some authors question the generalisation of these results (21). These studies have almost exclusively been performed in Asiatic countries where patients are younger, in better general shape, often include only early gastric cancer and have lower BMI compared to their Western counterparts (12-18). Additionally, most studies excluded patients with perioperative chemotherapy (12-18), whereas, according to ESMO guidelines, most Western patients are candidates for perioperative treatment (19). Consequently, the results from the current studies cannot be generally applied to Western patients. The aim of the present study was to determine the value of the ERAS protocol in patients with early and advanced gastric cancer operated with laparoscopic gastrectomy at a Western medical centre.
METHODS
Patients and ethical consideration
Before operation, a written informed consent was obtained from the patients. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University Medical Centre Maribor, Slovenia. The study was registered under the code UKC-MB-KME-74/20. Patients with histologically confirmed gastric cancer were included in the study. The inclusion criteria were as follows: i) a preoperative gastric cancer stage of any T, any N, M0; ii) no previous upper abdominal surgery; iii) laparoscopic surgery; iv) normal haematological, renal, hepatic, and cardiac parameters; v) ASA ? 3. Exclusion criteria were as follows: i) history of cancer; ii) presence of acute infection; iii) gastric cancer infiltrating other organs or causing obstruction. Patients were diagnosed between May 2015 and October 2020. Before operation, each patient was discussed at the local tumour board. Patients with preoperative stage Ib or higher were scheduled for perioperative chemotherapy. In the final group, 57 patients were included. While 39 patients received conventional perioperative care and laparoscopic surgery (CC), 11 received the ERAS rehabilitation program and laparoscopic surgery (ERAS).
Operation and treatment
All patients were operated by the same team of surgeons experienced in laparoscopic gastric cancer surgery. A totally laparoscopic total or subtotal gastrectomy was performed in all the included patients. The proportion of laparoscopic operations and types of reconstruction is presented in table 1. The elements of the ERAS protocol were developed according to ERAS consensus guidelines for gastric cancer (2). Details of the ERAS and conventional care protocols are listed in table 2. Patients in the ERAS group were educated before the surgery at the outpatient clinic. Patients were admitted 2 days before surgery. They were allowed to consume a normal diet up to 6 hours before operation. A carbohydrate-rich drink was allowed until 2 hours before surgery. Patients received no preoperative bowel preparation. Before operation, no nasogastric tube was inserted. On the day of the surgery, an epidural catheter was inserted. Patients in the ERAS group received additional postoperative anti-inflammatory drugs twice a day. Nasogastric tubes were removed on POD1 (post-operative day one), and they were allowed to sip clear fluid and a glutamine-rich drink. They began with early mobilisation. On POD1, they were encouraged to sit and perform respiratory rehabilitation; on POD2, they were encouraged to stand with help; on POD3, they began to walk. The postoperative intravenous fluids were gradually tapered off until POD3 or 4 when they received a soft diet. Patients were discharged when fully ambulatory, when they required no intravenous analgesia, or when with afebrile status. After discharge, they were regularly followed-up on outpatient clinic. All surgery was performed by the same experienced laparoscopic team. Depending on the location of the tumour, either a total or a subtotal laparoscopic gastrectomy was performed. The laparoscopic technique was described elsewhere (28, 29). The intestinal continuity was reconstructed with either Billroth II or Rouxen- Y anastomoses. The lymphadenectomy was performed in accordance with the Guidelines of Japanese Gastric Cancer Association (27). For early gastric cancer, a D1+ lymphadenectomy was sufficient; for all other stages, a D2 lymph node dissection was performed. The extraction of the specimen and the intestinal reconstruction were performed through a 5 to 8 cm supraumbilical midline incision. Drains were routinely placed in the right subhepatic and left subdiaphragmal space.
Study endpoints
Primary study endpoints were the length of the postoperative hospital stay, postoperative pain measured by the visual analogue scale (VAS) on days one to four, time to first defecation, duration of intravenous analgesics and the complication rate. Secondary endpoints were the costs of hospitalisation, postoperative systemic inflammatory response measured with serum CRP levels on days one, three and seven and the 30-day readmission rate.
Statistical analysis
Continuous variables were presented as mean ± SD for normally distributed variables and as median (IQR) for continuous variables without normal distribution. Discrete variables were presented as absolute number (percentage). Depending on the distribution, continuous variables were compared with Student’s t-test and Mann-Whitney’s U-test. Normality was tested with the Kolmogorow’s and Smirnoff’s test for normality. The discrete variables were compared with the 2 test of the Fisher’s exact test. The level of significance was the p value of 0.05 or less. All analyses were performed with the SPSS v. 22.0 (IBM, Chicago, IL, USA).
RESULTS
A total of 58 consecutive patients who underwent laparoscopic gastrectomy from January 2015 to October 2020 were included in the study. The baseline characteristics of the included patients are summarized in table 1. There was no significant difference in the distribution of patients’ characteristics between the ERAS and CC groups. Tumours in both groups were mostly located in the distal third of the stomach. In both groups, the same proportion of patients received perioperative chemotherapy (47.4% in the ERAS group vs. 43.6% in the CC group; p = 0.741).
Most of the patients in the ERAS group received a laparoscopic distal subtotal gastrectomy [16(84.2)]. In the CC group, significantly more patients received a laparoscopic total gastrectomy [23 (59); p = 0.002]. All patients in the ERAS group received a D2 lymphadenectomy compared to 69.2% of patients in the CC group (p = 0.012). The average number of dissected lymph nodes was significantly higher in the ERAS group (28±9 LNs in the ERAS vs. 19.9±13 LNs in the CC; p = 0.026). there was no significant difference in the number of positive LNs between groups. In all patients in the ERAS group, a Roux-en-Y reconstruction was used. In most cases in the CC group, Roux-en-Y reconstruction was used followed by Omega loop. A circular stapler was used in the CC group only in three cases. Operation time ways significantly shorter in the ERAS group [260 (112) min in ERAS vs. 300(40) min in CC; p = 0.025]. In both groups, we observed no 30-day mortality. The ERAS group had no morbidity and no mortality. Patients in the CC group had significantly more complications. In the CC group, major complications needing any form of intervention were observed in 25.6%. Between the ERAS and CC groups, there was no significant difference in the TNM distribution. However, in 12.8% of the included patients in the CC group the histology revealed a carcinoma in situ, while there was none in the ERAS group. Slightly less cases of early carcinoma was observed in the CC group compared to the ERAS group (42.1% in the ERAS vs. 30.8% in the CC; p = 0.862). There was no significant difference in the rate of R0 resection between groups. Patients in the ERAS group had a significant shorter hospital stay compared to the CC group (7.5(4) days in the ERAS vs. 11(6) days in the CC; p = 0.003). For patients in both groups, the time to first bowel movement was similar and needed IV analgesic treatment was similar. However, patients in the ERAS group had significantly smaller pain scores derived from VAS on days one to three. Total medical costs were significantly higher in the ERAS group (p < 0.0001). There were no significant differences in the 30-day readmission rate between groups (15.8% in both groups). The readmission rate in the patient group less than 65 years was 0% in the ERAS and 5.3% in the CC group. this difference was not significant. In both groups, differences in the postoperative stress responses measured with the serum levels of CRP on day one, three and seven were not significantly different. Even so, a faster return to baseline levels was observed in the ERAS group compared to the CC group. This difference did not reach the level of significance.
Subgroup analysis
In the subgroup analysis, only patients with no morbidity were compared for postoperative recovery results. Eleven patients from the ERAS group were compared to 27 patients in the CC group. After we excluded patients with postoperative morbidity, the length of hospital stay was only insignificantly longer in the CC group (p = 0.078). Patients in the ERAS group had a mean of 2-day shorter hospital stay. Total medical costs were higher in the ERAS group (p < 0.0001). The time to first bowel movement and duration of IV analgesia was similar, while the pain scores derived from VAS on days 1 to 3 were significantly less in the ERAS group. Values of postoperative stress indicators were similar in both groups. In the ERAS group, we again noticed an insignificantly faster recovery of postoperative serum CRP levels to baseline. Because of the small number of laparoscopic total gastrectomies in the ERAS group only a meaningful analysis of the subgroup with laparoscopic subtotal gastrectomy could be performed. In the subgroup of patients with laparoscopic subtotal gastrectomy patients in the ERAS group had more extracted lymph nodes per operation (27.7±9 LNs in ERAS vs. 16±13 LNs in CC; p = 0.009), shorter operation times (220(90) min in ERAS vs. 320(103) min in CC; p = 0.012), higher hospital costs (12479(69) EUR in ERAS vs. 11287(364) EUR in CC; p <0.0001), lower values of CRP on day seven (53(0) mg/ml in ERAS vs. 107(71) mg/ml in CC; p = 0.002), lower pain scores on days one to three compared to patients in the CC group (5(1), 5(2) and 5(6) in ERAS vs. 6.5(1), 7(2) and 6(1)in CC; p = 0.009, 0.011 and 0.024). In the ERAS group significantly more D2 lymphadenectomies were performed (16(100) in ERAS vs. 8(50) in CC; p = 0.003) and patients received exclusively a Roux-en-Y reconstruction (p < 0.0001). No significant differences were noted in the rate of conversions between groups. There were no complications in the ERAS group and significantly more proximal tumour location compared to patients in the CC group (p = 0.009). There were no significant differences in the duration of the hospital stay or the readmission rates between groups (table 3).
Multivarinate analysis
A forward stepwise conditional regression model was used to identify predictors significantly associated with the ERAS protocol. The multivariate logistic regression model identified hospital stay (HR: 0.567; 95%CI: 0.326-0.985; p = 0.044), and the pain scores on day 1 (HR: 0.12; 95%CI: 0.022-0.662; p = 0.015) and 2 (HR: 0.134; 95%CI: 0.026-0.693; p = 0.017) as significantly related to ERAS protocol.
DISCUSSION
Most of the present studies that evaluate the feasibility of the ERAS protocol after laparoscopic gastric cancer surgery were published in specialised Eastern centres, with fit patients capable to endure the strenuous ERAS protocol (17,25,26). Since there is avoid in studies evaluating the feasibility of the ERAS protocol after laparoscopic gastrectomy in the West, we performed a retrospective analysis comparing the results of laparoscopic gastrectomy of early and advanced gastric cancer patients combined with ERAS and conventional postoperative care at a Western centre.
Patients included in our study were older and had more accompanying diseases compared to studies published in the East (21-24). The age of patients included in RCTs by Sugisawa et al., Kang et al. and Mingjie et al. ranged from 56 to 64 years (17, 25, 26). The mean age of included patients in our study was 68 years. The majority of included patients had an ASA score of II or III. In addition, two thirds of patients in our study had advanced gastric cancer necessitating a more demanding laparoscopic total gastrectomy. This reflects the usual patient population seen in the West. Our results confirmed that even older patients satisfactorily complied with the ERAS protocol. Bu et al. reported that implementation of ERAS in older patients significantly increased the incidence of nausea, vomiting, gastric retention, and ileus (20). We did not observe such complications despite the older age of patients and the fact that nearly half of the patients received a total gastrectomy.
In the present study the multivariate logistic regression model related the ERAS protocol with shorter hospitalisation and smaller pain scores on days 1 and 2. Patients in the ERAS group had a significantly shorter hospital stay compared to the CC group. Similar results were reported from other RCTs (2-18, 25, 26) and meta-analyses (21-24). Contrary to the results from studies that included only the laparoscopic approach (2-18, 25, 26), we did not observe a faster recovery of bowel function nor did we observe a significant reduction of duration of IV analgesic use. The shorter hospital stay in our study thus could not be directly attributed to faster gut function recovery as reported elsewhere (21). On the other hand, we observed that pain scores derived from VAS on days 1 to 3 were significantly less in the ERAS group compared to the CC group in the univariate analysis.
Based on this finding, we propose that the ERAS protocol combined with minimally invasive surgery reduces the pain on first postoperative days which in turn allows faster mobilisation, especially on days 1 and 2. The mobilisation of patients on the first two days is critical, since it reduces the likelihood of respiratory complications that prolong the hospital stay (21). In order to achieve shorter hospitalisation, it is therefore prudent to strive for early full mobilisation. This is especially the case in elderly and frail patients who are more prone to secondary infections.
Moreover, elderly less ambulant patients feel reluctant to discharge from the hospital even if the pain score on days four and more might be low.
There are conflicting results regarding the readmission rates between the ERAS protocol and conventional care in the literature (20-25). Most of the initial papers reported higher readmission rates in patients after laparoscopic gastrectomy with ERAS protocol (20-24). Only recently papers have begun to emerge reporting exceedingly low readmission rates (25). This suggests that sufficient experience was necessary to reduce readmissions. The readmission rate in the present study was 15.8% and no statistical difference was found between the ERAS protocol and conventional care. Readmission rates presented in the present study might be higher than reported by Sugisawa et al. (0% readmission rate in both groups) (25). However, in their study only patients with an ECOG performance status of 0 were included (25). As shown by Bu et al. age and general performance are significant factors that predispose patients to readmission (20). When we excluded patients older than 65 years, we also did not observe any readmissions, which is in agreement with the observations made by Bu et al and results published by other Eastern studies (20-25).
No morbidity and mortality was observed in the ERAS group. Significantly more patients had complications in the CC group. In the CC group we observed minor complications (Dindo-Claviene
Surprisingly in the subgroup analysis of patients with no complications, patients in the ERAS group had significantly less pain on days one to three. While the hospital stay in the EARS group was shorter compared to the CC group, this difference did not reach the level of significance. In the subgroup analysis of patients who received laparoscopic subtotal gastrectomy we observed significantly higher lymph node yield per operation and shorter operating times in the ERAS group. The CRP levels on day seven and the pain scores on days one to three were significantly smaller in ERAS group. In spite of this no difference in the length of hospital stay was observed. This finding is in contrast to current published studies (21-24). Since laparoscopy itself reduces hospital stay compared to open surgery, we agree with Liu et al. that the statistical insignificance in such cases may be attributed to benefits of laparoscopic gastrectomy, leaving little room for improvement via the implementation of the ERAS protocol (23).
Total medical costs were significantly higher in the ERAS group. This finding stands in contrast to most other studies reporting that shorter hospital stays bring down cost (21-24). In our country, medical costs of hospital stay are cheap. The main bulk of costs are produced by the multimodal approach necessary for the ERAS protocol. The difference of hospital stay of two days is not enough to reduce costs of the multimodal approach. This highlights the importance of conducting ERAS studies in different countries. Medical systems differ from region to region and results cannot be extrapolated globally.
The inflammatory response after the ERAS protocol combined with laparoscopy was found by many authors to be reduced (16). The association of inflammatory response and the ERAS protocol is still not understood (21). Some evidence points that early postoperative nutrition strengthens the gut barrier (21). Nonetheless, we could not confirm lower CRP levels in the ERAS group in our study. The rise of serum CRP was smaller in the ERAS group and the levels fell faster compared to the CC group at discharge, but this did not reach the level of significance. We attributed this to the small sample size of the study.
Many critics are concerned with the oncological sufficiency of ERAS and laparoscopic treatment (18). In our study, all patents in the ERAS group had a R0 resection. In each case, a D2 lymph node dissection was performed, and the average number of extracted lymph nodes is comparable to other RCT that reported the lymph node yield (12-18). We could also show that perioperative treatment did not have any impact on the compliance of patients with the ERAS protocol or produce additional morbidity. Patients after preoperative course of chemotherapy are in worse general condition and have a poorer nutritional status. Our results prove that, despite chemotherapy, even elderly patients with early and advanced gastric cancer could be included in the ERAS protocol. In addition, the ERAS protocol involves key elements aimed at improving the nutritional status of patients. Patients after neoadjuvant treatment should benefit the most from this protocol. This was supported by our results.
Our study has some limitations. Since a small number in the ERAS group received a laparoscopic total gastrectomy, meaningful subgroup analysis to evaluate the feasibility of the ERAS protocol in laparoscopic total gastrectomy could not be performed in the present study. Further trials with more included patients will be necessary. Meanwhile, there was a significant difference in the type of intestinal continuity reconstruction between patients in the ERAS and CC group. It is therefore questionable whether ERAS patients fared better because of the reconstruction and to what extent the ERAS protocol was responsible. Secondly, it was a retrospective study; hence some bias in inclusion of patients might be present. Finally, the ERAS protocol advocates against the use of drains. Nevertheless, gastric cancer surgery is associated with a morbidity of up to 45%, therefore most authors report the use of abdominal drains, and only one study on ERAS in gastric cancer reported no use of drains (18).
CONCLUSION
In conclusion our results confirm that the ERAS protocol can be safely used in elderly patients with early and advanced gastric cancer. It reduces the hospital stay and pain scores on days one and two. The perioperative treatment did not influence the compliance of patients in the ERAS group. Patients benefit from laparoscopic surgery combined with the ERAS protocol and can tolerate the intense postoperative treatment even after adjuvant chemotherapy. The protocol reduces postoperative pain on days one and two which allows faster mobilization and shorter hospital stays. Although the results support the use of ERAS combined with laparoscopic subtotal gastrectomy in elderly patients with early and advanced gastric cancer, additional RCT conducted in specialised Western centres are needed to determine the value of the ERAS protocol in laparoscopic total gastrectomy in the West.
Authorship confirmation statement
All authors confirm that the results presented in this article is their own original work and that the information they provided on these pages are true.
Conflict of interest
All author declare that they have no conflict of interest.
Fundind statement
None declared.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University Medical Centre Maribor, Slovenia. The study was registered under the code UKCMB- KME-74/20.
REFERENCES
1. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J Surg. 2019;43(3):659-695.
2. Mortensen K, Nilsson M, Slim K, Schäfer M, Mariette C, Braga M, et al. Consensus guidelines for enhanced recovery after gastrectomy: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Br J Surg. 2014;101(10):1209-29.
3. Yamada T, Hayashi T, Aoyama T, Shirai J, Fujikawa H, Cho H et al. Feasibility of enhanced recovery after surgery in gastric surgery: a retrospective study. BMC Surg, 2014;14:41.
4. Liu XX, Jiang ZW, Wang ZM, Li JS. Multimodal optimization of surgical care shows beneficial outcome in gastrectomy surgery. JPEN J Parenter Enteral Nutr. 2010;34(3):313-21.
5. Wang D, Kong Y, Zhong B, Zhou X, Zhou Y. Fast-track surgery improves postoperative recovery in patients with gastric cancer: a randomized comparison with conventional postoperative care. J Gastrointest Surg, 2010; 14(4):620-7.
6. Park YK, Yoon HM, Kim YW, Park JY, Ryu KW, Lee WJ, et al. Laparoscopy-assisted versus open D2 distal gastrectomy for advanced gastric cancer. Ann Surg. 2018;267(4):638-645.
7. Son T, Hyung WJ. Laparoscopic gastric cancer surgery: Current evidence and future perspectives. World J Gastroenterol. 2016; 22(2):727-35.
8. Son T, Kwon IG, Hyung WJ. Minimally invasive surgery for gastric cancer treatment: Current status and future perspectives. Gut Liver. 2014;8(3):229-36.
9. Shi Y, Xu X, Zhao Y, Qian F, Tang B, Hao Y, et al. Long-term oncologic outcome of a randomized controlled trial comparing laparoscopic versus open gastrectomy with D2 lymph node dissection for advanced gastric cancer. Surgery. 2019;165(6): 1211-1216.
10. Best LMJ, Mughal M, Gurusamy KS. Laparoscopic versus open gastrectomy for gastric cancer (Review). Cochrane Database Syst Rev. 2016;3(3):CD011389.
11. Ding J, Liao GQ, Liu HL, Liu S, Tang J. meta-analysis of laparoscopyassisted distal gastrectomy with D2 lamph node dissection for gastric cancer. J Surg Oncol. 2012;105(3):297-303.
12. Hu JC, Jiang LX, Cai L, Zheng HT, Hu SY, Chen HB, et al. Preliminary Experience of Fast-Track Surgery Combined with Laparoscopy- Assisted Radical Distal Gastrectomy for Gastric Cancer. J Gastrointest Surg, 2012;16(10):1830-9.
13. Kim JW, Kim WS, Cheong JH, Hyung WJ, Choi SH, Noh SH. Safety and efficacy of fast-track surgery in laparoscopic distal gastrectomy for gastric cancer: a randomized clinical trial. World J Surg, 2012; 36(12):2879-87.
14. Sahoo MR, Gowda MS, Kumar AT. Early rehabilitation after surgery program versus conventional care during perioperative period in patients undergoing laparoscopic assisted total gastrectomy. J Minim Access Surg, 2014;10(3):132-8.
15. Abdikarim I, Cao XZ, Li SZ, Zhao XQ, Taupyk Y, Wang Q. Enhanced recovery after surgery with laparoscopic radical gastrectomy for stomach carcinomas. World J Gastroenterol, 2015; 21(47): 13339-44.
16. Liu G, Jian F, Wang X, Chen L. Fast-track surgery protocol in elderly patients undergoing laparoscopic radical gastrectomy for gastric cancer: a randomized controlled trial. Onco Targets Ther, 2016; 9:3345-51.
17. Kang SH, Lee Y, Min SH, Park YS, Ahn SH, Park DJ, et al. Multimodal Enhanced Recovery After Surgery (ERAS) Program is the Optimal Perioperative Care in Patients Undergoing Totally Laparoscopic Distal Gastrectomy for Gastric Cancer: A Prospective, Randomized, Clinical Trial. Ann Surg Oncol. 2018;25(11):3231-3238.
18. Li Y, Qiu J, Cao H. Application of enhanced recovery after surgery for patients with laparoscopic radical gastrectomy. Zhonghua Wei Chang Wai Ke Za Zhi. 2016;19(3):269-73.
19. Smyth EC, Verheij M, Allum W, Cunningham D, Cervantes A, Arnold D, ESMO Guidelines Committee. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27(suppl 5):v38-v49.
20. Bu J, Li N, Huang X, He S, Wen J, Wu X. Feasibility of fast-track surgery in elderly patients with gastric cancer. J Gastrointest Surg, 2015;19(8):1391-8.
21. Wee IJY, Syn NLX, Shabbir A, Kim G, So JBY. Enhanced recovery versus conventional care in gastric cancer surgery: a meta-analysis of randomized and non-randomized controlled trials. Gastric Cancer, 2019;22(3):423-434.
22. Li MZ, Wu WH, Li L, Zhou XF, Zhu HL, Li JF, et al. Is ERAS effective and safe in laparoscopic gastrectomy for gastric carcinoma? A meta-analysis. World J Surg Oncol, 2018;16(1):17.
23. Li Z, Wang Q, Li B, Bai B, Zhao Q. Influence of enhanced recovery after surgery programs on laparoscopy-assisted gastrectomy for gastric cancer: a systematic review and meta-analysis of randomized control trials. World J Surg Oncol. 2017;15(1):207.
24. Wang LH, Zhu RF, Gao C, Wang SL, Shen LZ. Application of enhanced recovery after gastric cancer surgery: An updated metaanalysis. World J Gastroenterol. 2018;24(14):1562-1578.
25. Sugisawa N, Tokunaga M, Makuuchi R, Miki Y, Tanizawa Y, Bando E et al. A phase II study of an enhanced recovery after surgery protocol in gastric cancer surgery. Gastric Cancer. 2016;19(3):961-7.
26. Xia Mingjie, Zhang Luyao, Tang Ze, Zhao Yin Quan, Wang Quan. Laparoscopic Radical Gastrectomy for Resectable Advanced Gastric Cancer Within Enhanced Recovery Programs: A Prospective Randomized Controlled Trial. J Laparoendosc Adv Surg Tech A, 2017;27(9):959-964.
27. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer, 2017; 20(1):1-19. 28. Jagric T. The impact of modifying the laparoscopic lymphadenectomy technique on the extent of lymphadenectomy in laparos-copically operated gastric cancer patients. A single-center study. Surgery and Surgical Endoscopy, 2019; 1(1): 19-25.
29. Jagric T. East meets West: the initial results of laparoscopic gastric cancer resections with Eastern principles in a single Western centre - a propensity score-matched study. Langenbecks Arch Surg. 2021; 406(8):2699-2708.
Full Text Sources:
Abstract:
Views: 3578
Watch Video Articles
For Authors
Journal Subscriptions

Current Issue
Dec 2025
Supplements
Instructions for authors
Online submission
Contact
ISSN: 2559 - 723X (print)
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Open Access Statement
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Journal Metrics
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.