Surgery, Gastroenterology and Oncology
|
Introduction: Laparoscopy can diagnose and treat the etiologies of acute upper abdominal pain. This study aimed to assess the effectiveness of laparoscopy in upper gastrointestinal (G.I.T) emergencies regarding intraoperative and postoperative outcomes.
Method: A retrospective observational study was conducted in the emergency departments of Zagazig University on 215 patients who had upper abdominal emergency surgeries between June 2017 and June 2020.
Results: The majority of patients (68%) were £ 40 years old, with a male predominance (67%). Acute cholecystitis (54%), perforated peptic ulcer (PU) (18%), splenic injuries (26%), and acute pancreatitis with necrosis (2%) were the most common reasons for surgical upper G.I.T. emergencies. Intraoperative complications occurred in 10 cases(5%) in the form of omental bleeding (2%), cystic artery bleeding(1%), liver injuries (0.5%), injury to the duodenum (0.5%), injury to the colon (0.5%), and bile duct injury (0.5%). Intraoperative conversion occurred in 10 patients (5%), with the most common reasons being uncontrolled bleeding (2%), obstructed anatomy or difficult dissection (1%), difficult closure of perforated peptic ulcer (0.5%), duodenal injury (0.5%), colonic injury (0.5%), and bile duct injury (0.2%). Postoperative complications occurred in 41 patients(20%) in the form of wound infection (5%), hematoma (3%), ileus (2.5%), seroma (2%), pneumonia (1.5%), and intra-abdominal abscess formation (1%), omental bleeding (1%), adhesive IO (1%), cystic duct stump leakage (1%), biliary stricture (0.5%), port site hernia (0.5%), port site bleeding (0.5%), and cystic artery stump bleeding(0.5%). Re-intervention occurred in 9 patients (4.5%), with a mortality rate of 1.5%.
Conclusion: In upper G.I.T. emergencies, the laparoscopic approach is safe and feasible, with good intraoperative and postoperative outcomes.
Introduction
When surgical procedures are standardized, the benefits of laparoscopy in a range of emergency scenarios are acknowledged without question. When only a basic strategy is set for the surgery, and the surgical approach entirely depends on intra-abdominal findings, the benefits are diminished or unknown. The evidence unequivocally supports the superiority of a laparoscopic approach in numerous emergency cases, such as acute cholecystitis, gastroduodenal perforated ulcers, infected pancreatic necrosis, and splenic injuries (1-4).
Laparoscopy gives the primary advantages of a shorter hospital stay, a quicker procedure, and faster recovery without complications. Rapid recovery is connected with early enteral feeding. Adequate nutritional support aids in maintaining homeostasis and, as a result, enhances immunity, thereby decreasing the incidence of wound infection. Laparoscopy should be considered with caution whenever abdominal access is considered difficult, as in cases of organ enlargement, adhesion, and bowel distension. In actuality, creating the pneumoperitoneum is an essential step in the procedure. Increased intraperitoneal pressure produces cardio-respiratory and neurological effects (5-9). In this study, we designed a retrospective observational study to present our experience in assessing the outcomes of a laparoscopic approach in emergent upper abdominal surgery in terms of intraoperative and postoperative complications.
Patients and methods
Design of the study and participants
Between June 2017 and June 2020, 215 patients were admitted to Zagazig University Hospital emergency surgical unit with clinical diagnoses of upper G.I.T. emergencies, namely acute cholecystitis, perforated P.U., acute necrotizing pancreatitis, and splenic trauma. The work has been reported following STROBE guidelines. To be included in the study, patients must meet the following criteria: >18 years of both sexes complaining of acute upper G.I.T. emergencies and undergoing laparos-copic surgeries, namely acute cholecystitis, perforated peptic ulcer, pancreatic necrosis, and splenic injuries.
< 18 years of age and open surgeries for upper G.I.T. emergency surgeries were excluded.
Types of outcomes (clinical endpoints)
The primary outcome was the occurrence of intraoperative complications. The secondary outcome was postoperative complications.
Method
Perioperative assessment and approach
The diagnosis was based on plain x-rays, abdominal ultrasonography, and computed tomography (C.T.). General anesthesia with cuffed endotracheal intubation to prevent vomiting aspiration. For three years, all procedures were performed in a single facility. The operative steps were carried out exactly as described before (4,10-12).
Drains were placed, one in the pelvis and the other at the subphrenic site, and were left in place as long as discharge came out. Daily outputs from all operatively positioned drains were recorded. CT-guided percutaneous drainage may be employed in cases of intra-abdominal abscess. Patients were given clear fluid as soon as they could tolerate it. Antibiotic prophylaxis was continued for 24 hours after the procedure. The drainage tube was withdrawn when the patient had defecated, and the drain was normal.
Following hospital discharge, all patients were followed for 24 months. Patients were reached by phone, outpatient clinic visits, or e-mail messages. After 12 months, a full history and clinical examination were completed, as well as U.S.S. and C.T. (to detect late complications). During the follow-up period, no patients were lost to follow-up.
Statistical analysis
The mean S.D. was used for normally distributed continuous variables; the median was used for non-normally distributed continuous variables. Percentages represented categorical variables. The laboratory findings were evaluated to see if they were within the usual range. All statistical analyses were performed using S.P.S.S. version 20 (S.P.S.S., Chicago, IL).
Results
Table 1 displays demographic and preoperative data. The majority of patients (68%) were ≤ 40 years old, with a male predominance (67%). The most prevalent causes of surgical upper G.I.T. emergencies were acute cholecystitis (54%), perforated PU (18%), splenic injuries (26%), and acute pancreatitis with necrosis (2%). Diabetes mellitus was the most common related co-morbidity (31%), followed by hypertension (24%). The majority of cases (92%) had ≤ ASA III. The initial B.M.I. was 35.5±2.35, and 18% had previous abdominal operations.
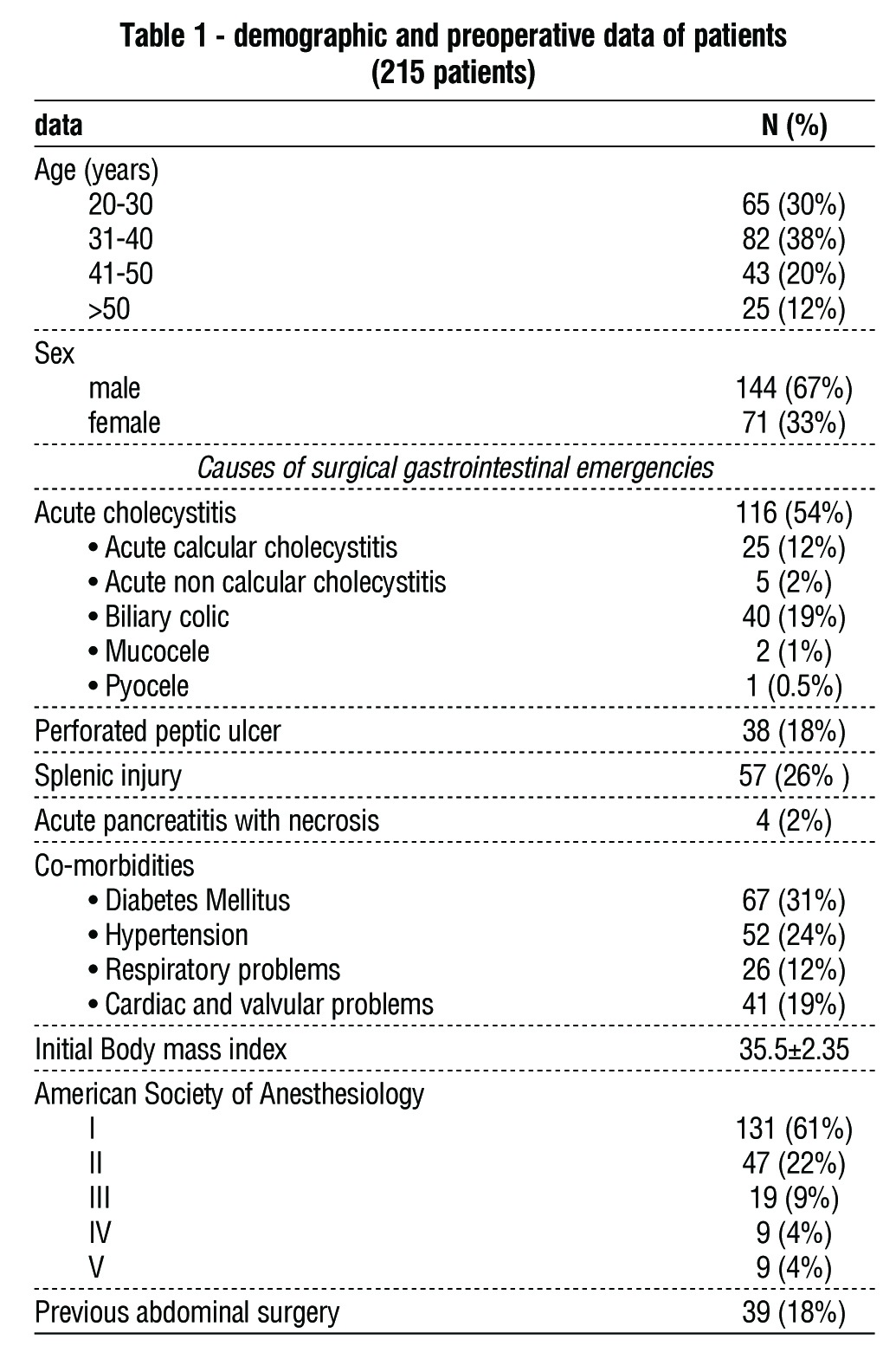
Table 2 displays the intraoperative data. Most cases (55%) required more than 60 minutes of surgery. The most common intraoperative consequences were omental bleeding (2%), cystic artery bleeding (1%), liver injuries (0.5%), duodenal injury (0.5%), and bile duct injury (0.5%). Conversion occurred in 10 patients (5%); the most common reasons for conversion were uncontrolled bleeding (2%), clogged anatomy or difficult dissection (1%), difficult closure of a perforated duodenum (0.5%), injury to the duodenum (0.5%), injury to the colon (0.5%), and injury to the bile duct (0.5%).
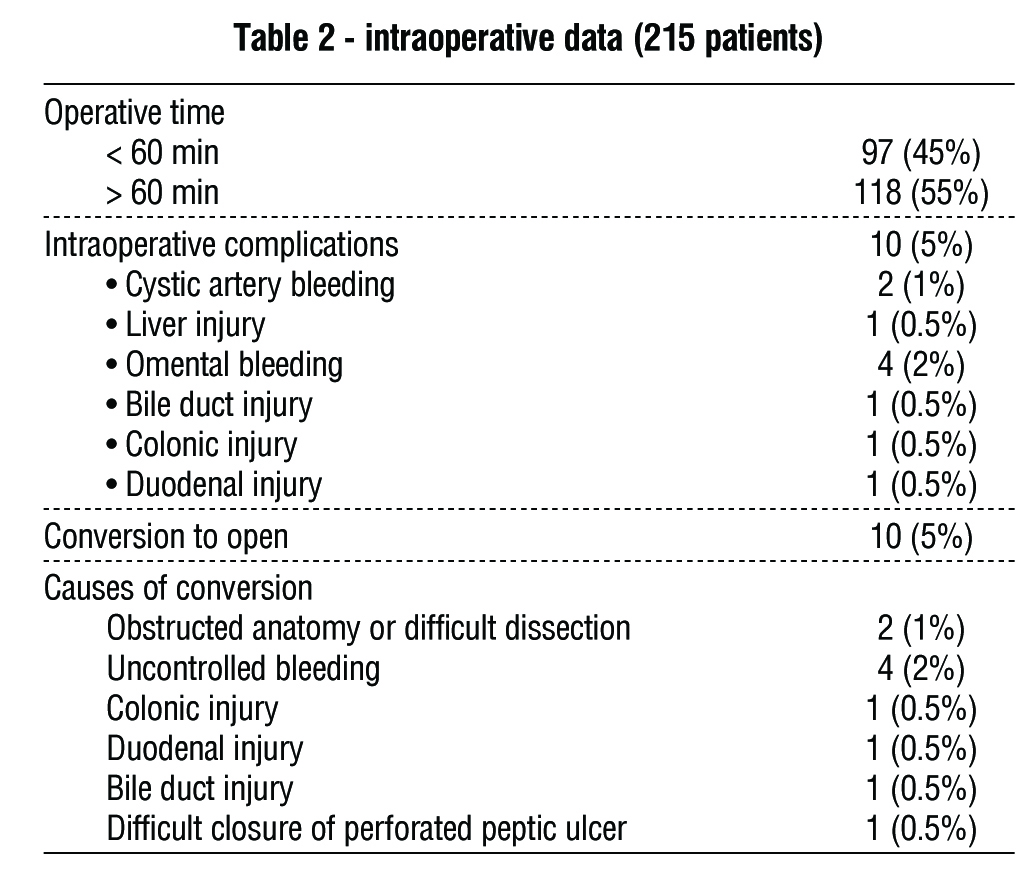
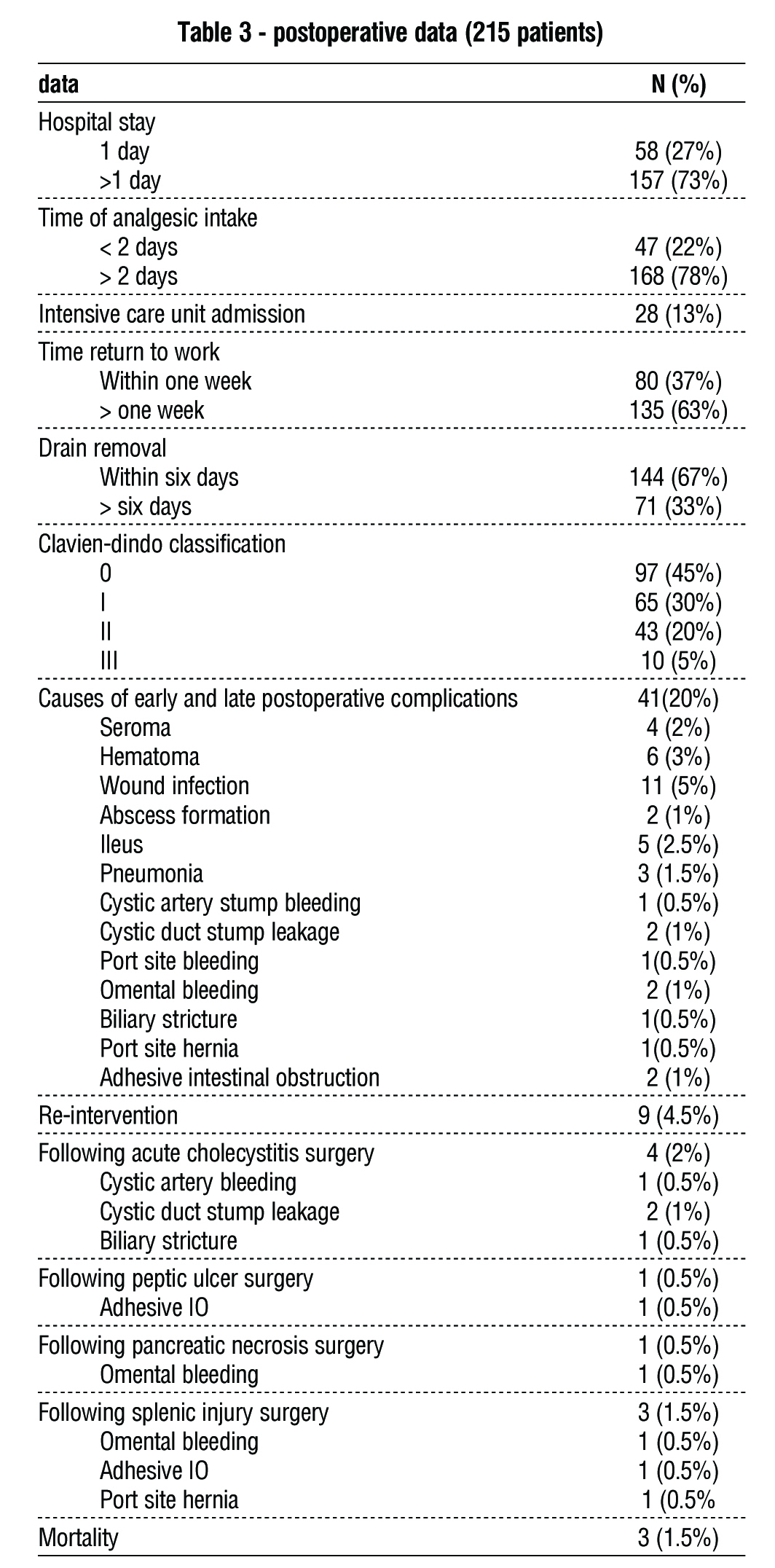
Table 3 displays the postoperative data for the patients investigated. The majority of cases (73%) were hospitalized for more than one day; the majority (78%) received analgesics for more than two days, with 13% admitted to the I.C.U. In the postoperative period, the majority of cases (63%) took more than one week to return to work, and 67% of patients had drain removal within six days. The most common causes of postoperative early and delayed problems were wound infection (5%), hematoma (3%), ileus (2.5%), seroma (2%), pneumonia (1.5%), and intra-abdominal abscess formation (1%), omental bleeding (1%), adhesive IO (1%), cystic duct stump leakage (1%), biliary stricture (0.5%), port site hernia (0.5%), port site bleeding (0.5%), and cystic artery stump bleeding (0.5%). Re-exploration happened in 9 patients (4.5%), with a mortality rate of 1.5%.
Discussion
The role of laparoscopy in upper G.I.T. emergencies, such as acute cholecystitis, perforated P.U., pancreatic necrosis, and splenic trauma, is debatable. Our study aimed to evaluate the role of laparoscopy in these situations. We found that the most prevalent causes of surgical upper G.I.T. emergencies were acute cholecystitis (54%), perforated PU (18%), splenic injuries (26%), and acute pancreatitis with necrosis (2%). The most common intraoperative consequences were omental bleeding (2%) and cystic artery bleeding (1%). Conversion to open surgery occurred in 10 patients (5%), with the most prevalent reasons being uncontrolled bleeding (2%), clogged anatomy, or difficult dissection (1%). The most common causes of postoperative early and delayed problems were wound infection (5%), hematoma (3%), ileus (2.5%), seroma (2%), pneumonia (1.5%), and intra-abdominal abscess formation (1%), omental bleeding (1%), adhesive IO (1%), cystic duct stump leakage (1%), biliary stricture (0.5%), port site hernia (0.5%), port site bleeding (0.5%), and cystic artery stump bleeding (0.5%). Re-exploration happened in 9 patients (4.5%), with a mortality rate of 1.5%.
Acute gallbladder diseases
Acute cholecystitis affects 20% to 30% of the population, making it the third most common cause of acute abdomen treated in emergency rooms (13). Conversion, re-exploration, and biliary damage were among the postoperative problems feared to arise from laparoscopy procedures performed in emergency conditions. Predictive indicators for difficult cholecystectomy with a high conversion rate have been studied previously (14). Other research has shown that performing a cholecystectomy as soon as possible (within the first 72 hours) is preferable since it shortens the operative time and time patients need to stay in the hospital (1). However, a different study examined how severity levels affected patients' treatment preferences (15).
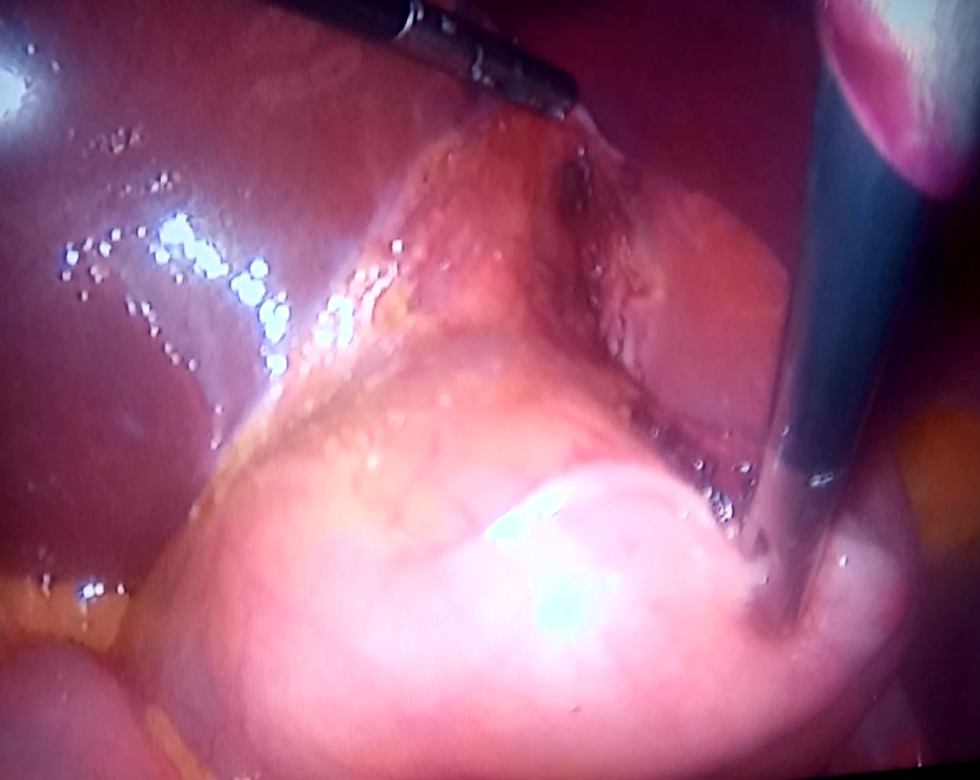
In our center, acute cholecystitis is the most common emergency upper G.I.T. procedure (54%). It is most likely linked to high-fat dietary variables. The most prevalent reason for surgery was persistent biliary colic, followed by acute calcular cholecystitis. We operate within three days of the onset of symptoms and begin with identifying the Calot triangle. If the Calot triangle cannot be identified, we proceed with the fundus first approach (fig. 1). The incidence of intraoperative and postoperative complications was low in our study, with excellent outcomes due to the panoramic view of the laparoscope, high experience, and finally, thanks to the recent technology expressed by the use of harmonic scalpel with minimal bleeding. The most prevalent intraoperative consequences were cystic artery hemorrhage (1%) and bile duct damage (0.5%). One case of cystic artery bleeding was managed intraoperatively by clipping, whereas the other required open conversion for bleeding control. One case of intraoperative bile duct injuries that could not be detected by laparoscopy was handled by open conversion and satisfactory tear detection with suture repair by Vicryl 5/0 interrupted suture. The most common postoperative complications were seroma (n=4), hematoma (n=6), wound infection (n=11), ileus (n=5), gallbladder bed abscess (n=2), cystic artery bleeding (n=1),cystic duct stump leakage(n=2) and biliary stricture(n=1). Re-intervention occurred in 9 patients (4.5%).
A previous study identified conversion risk variables as male, old, very overweight, having cirrhosis, previous upper abdominal surgery, severe acute cholecystitis, and emergency laparoscopic cholecystectomy (16). While several studies have confirmed that upper G.I.T. surgery is not a contraindication for laparoscopic cholecystectomy (17) and that cholecystectomy after the sleeve is safe (18).
Another study stated that the main reasons for the conversion to open surgery are the lack of a critical view of safety, a fully buried gallbladder, a stone stuck in the gallbladder, and the inability to hold the gallbladder. (19). We faced the problem of difficulty handling the fundus of the gallbladder in acute cholecystitis, especially if mucocele or pyocele, and we solved this problem by needle evacuation of gallbladder content. That helped us immensely to hold the fundus and push the gallbladder over the liver to identify the Calot triangle, which was challenging in circumstances of acute inflammation. In this case, if the Calot triangle could not be defined well, we used a fundus first approach, which greatly aided us in elevating the Calot triangle and facilitating dissection (20). The important thing in our approach was not to injure the biliary tract in any way, so if there was difficulty identifying the Calot triangle safely, we performed a subtotal cholecystectomy. However, we faced gallbladder remnant and cystic duct stump stone formation, which necessitated further operation by laparoscopic completion cholecystectomy, which has proven superior to open completion cholecystectomy (21).
In our study, the most common reasons for reintervention were cystic artery stump bleeding (one case), which was controlled by suture ligation; cystic duct stump leakage (two cases), which was controlled by endoscopic stenting using ERCP; and biliary stricture (one case), which was controlled by endoscopic dilatation and stent insertion via ERCP.
Another challenging factor is elderly people who may complain of acute cholecystitis and have an inadequate cardiopulmonary reserve, particularly during the COVID-19 era, with consequent post- COVID-19 pulmonary fibrosis and therefore, pneumo-peritoneum emerging as a hazard during laparoscopic cholecystectomy. We solved this problem by creating a low-pressure pneumoperitoneum (10 mmHg) and starting with a fundus-first cholecystectomy. This helped move the gallbladder higher over the liver during the dissection of the Calot triangle, which led to a lower rate of complications (22). A comparablestudy demonstrated the efficiency of low-pressure pneumoperitoneum in laparoscopic cholecystectomy for acute cholecystitis with a fundus-first approach over open cholecystectomy with a superior outcome (23-24).
Perforated gastro-duodenal ulcer
A perforated peptic ulcer is an acute gastrointestinal condition most commonly caused by peptic ulcers, with an incidence of 2-10% (25). A study found that the laparoscopic approach is an essential diagnostic tool for the ulcer site, size, and etiology (26). All cases in our study underwent simple closure with an omental patch by laparoscope and had excellent intraoperative and postoperative outcomes, which was agreed upon by other studies (2, 27-28).
Conversion is an essential item during laparoscopic P.U. repair, with an incidence of 5.3%-8%, and they attributed the causes of conversion to the size of the perforation, the friable edges of the lesion, the degree of peritonitis, shock at the time of hospitalization, and more than a day delay in diagnosis (29-30).
The conversion happened in four patients in our investigation due to obstructed anatomy (1 patient), uncontrolled bleeding (2 patients), and difficult closure of the ulcer (1 patient). This incidence was lower than in the previous studies, presumably due to sampling size variance, and most cases were smaller perforated ulcers < 2 cm in size. In the current series, postoperative complications included wound infection (4 cases), hematoma (2 cases), seroma (1 patient), ileus (1 patient), pneumonia (1 patient), and adhesive IO (one patient). Re-intervention occurred in one case of adhesive I.O. and needed adhesiolysis.
Pancreatic emergencies
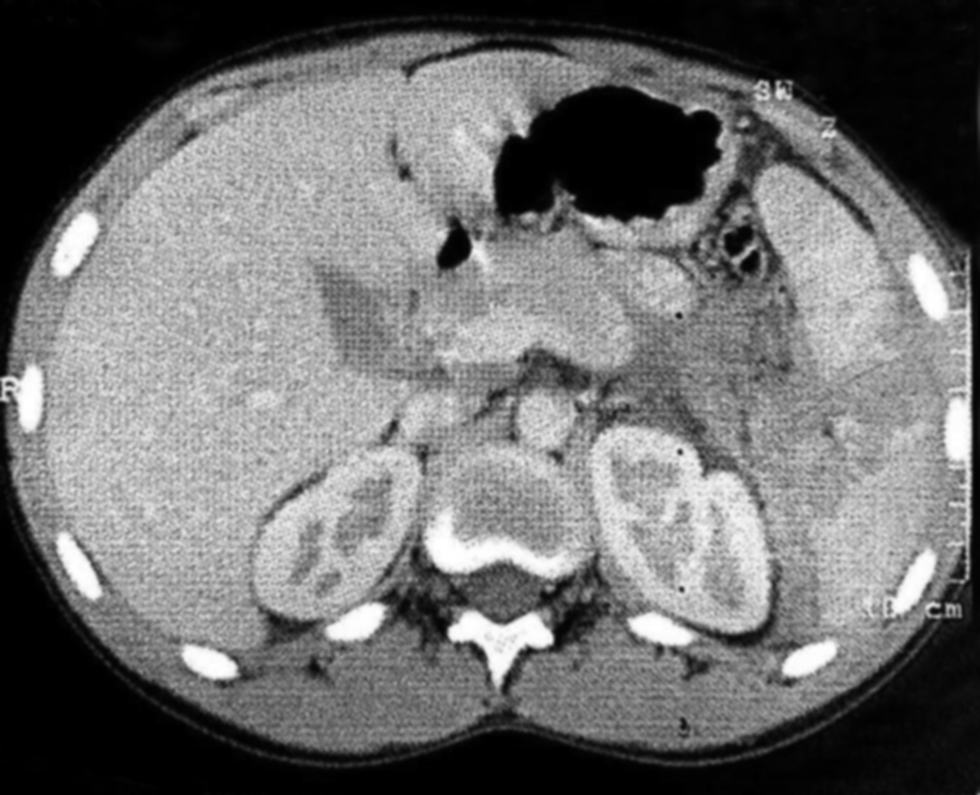
Approximately 20% of acute pancreatitis patients develop pancreatic necrosis, and 30% are infected, with a 30%-39% mortality rate (31-32). Surgical intervention is indispensable in treating infected pancreatic necrosis (31,33) but with significant complications such as new organ failure, sepsis, abdominal hemorrhage, and gastrointestinal fistula (34-35).
In our analysis, four patients (2%) had laparoscopic transperitoneal necrosectomy. Intraoperative omental hemorrhage occurred in three patients, two of whom were treated intraoperatively, while the third was controlled after conversion. Another intraoperative complication was a duodenal injury during pancreatic necrosis debridement, which needed conversion and closure of the tear with a gastro-jejunostomy.
Splenic trauma
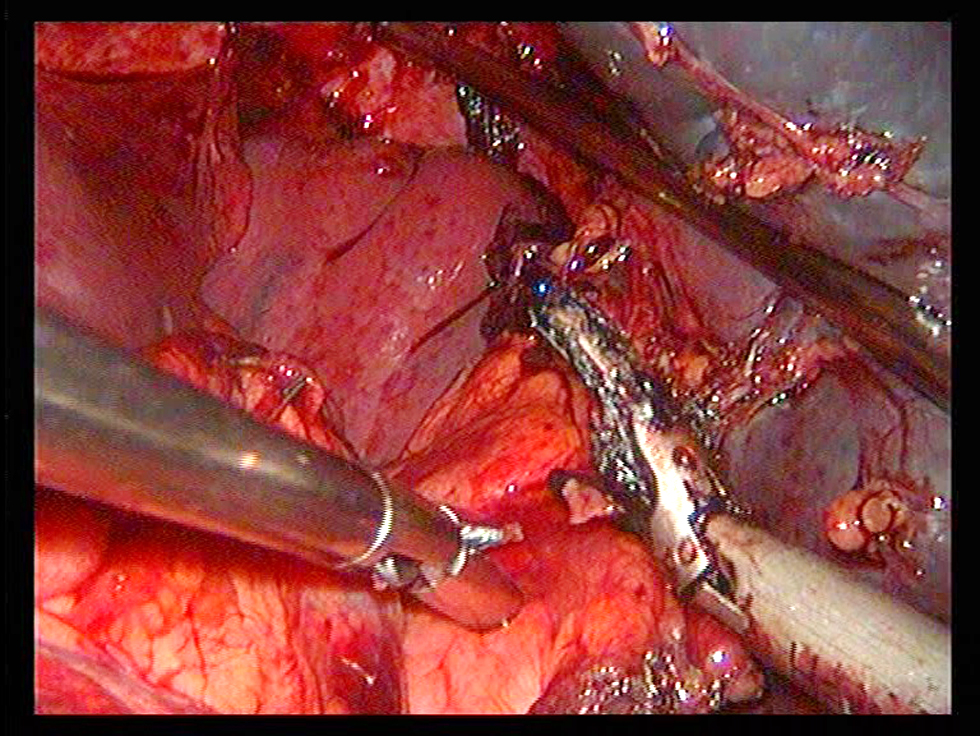
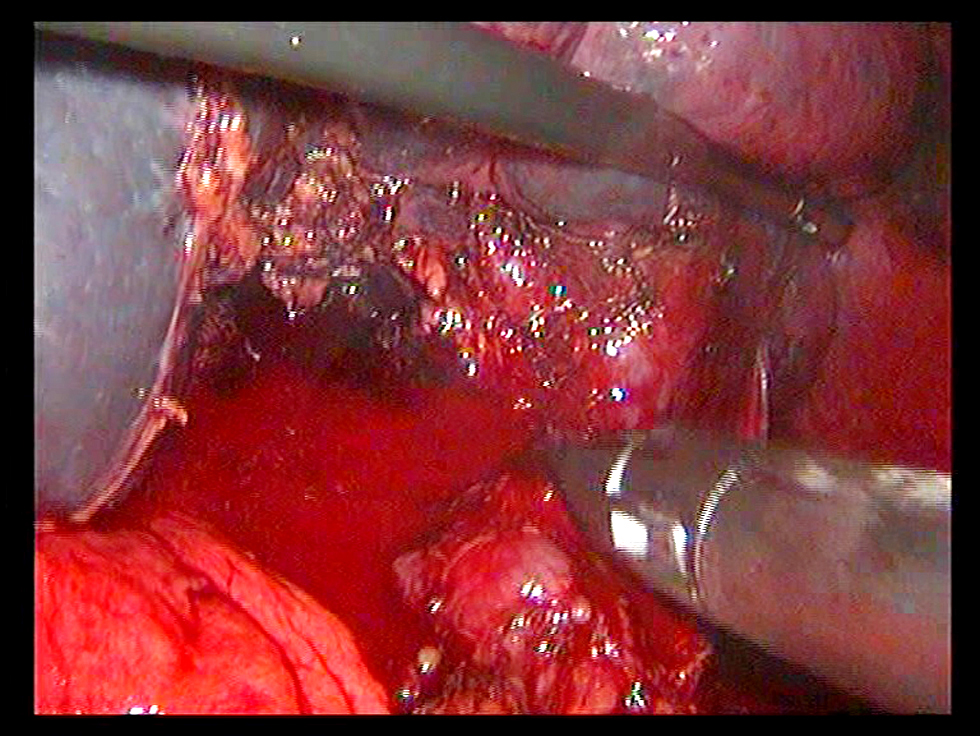
Laparoscopy is a reliable and safe treatment in low-grade hemodynamically stable splenic injuries (fig. 2) with a shorter hospital stay and a lower morbidity and mortality rate (36-38). In our study, 57 patients with splenic injuries (26%) were treated with a laparoscopic method (fig. 3), with two cases experiencing intraoperative difficulties (one of omental bleeding and one of colonic injury). The omental bleeding was successfully controlled with a laparoscope, whereas the colonic damage case required open conversion with tear repair and a right transverse colostomy. Another incidence of conversion happened as a result of difficult dissection (fig. 4). The commonest postoperative complications were seroma (n=2), hematoma (n=2), abscess formation (n=1), ileus (n=1), pneumonia (n=2), omental bleeding (n=1), port site hernia (n=1), and adhesive IO (n=1).
Conclusion
The laparoscopic approach is safe and feasible in upper abdominal emergency surgeries with low
morbidity and mortality.
Registration
Criteria for registering on the quality control review protocol on clinical trials.
Ethical approval, consent to participate
The faculty of the Medical Ethical Committee at Zagazig University granted us all the ethical agreements.The described work has been carried out for human experiments following the World Medical Association's Code of Ethics (Helsinki Declaration).The work followed STROBE guidelines.
Authors’ contributions
All Authors contributed equally to the study as regards the conception and design of the study, acquisition of data, analysis and interpretation of data, drafting the article or revising it critically for important intellectual content, and final approval of the version to be submitted.
Competing interests
The authors declare that they have no competing financial or non-financial interests.
Acknowledgement
We would like to thank all members of the laparos-copic unit in the faculty of medicine at Zagazig University for their great help and recommendations.
Funding
This research did not receive any specific grant from public, commercial, or not-for-profit funding agencies.
References
1. Pisano M, Allievi N, Gurusamy K, Borzellino G, Cimbanassi S, Boerna D, Coccolini F, et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J Emerg Surg. 2020;15(1):61.
2. Cirocchi R, Søreide K, Di Saverio S, Rossi E, Arezzo A, Zago M, et al. Meta-analysis of perioperative outcomes of acute laparoscopic
versus open repair of perforated gastroduodenal ulcers. J Trauma Acute Care Surg. 2018;85(2):417-425.
3. Tarasconi A, Coccolini F, Biffl WL, Tomasoni M, Ansaloni L, Picetti E, et al. Perforated and bleeding peptic ulcer: WSES. guidelines. World J Emerg Surg. 2020;15:3.
4. Tamer A.A.M. Habeeb, Emad Salah, Ahmed S. Mohamed, Said M. Negm. Role of Laparoscopic Splenectomy in Isolated
High-Grades Splenic Injuries: A Randomized Controlled Trial. Surg. Gastroenterol. Oncol. 2021 eCollection September 30
DOI: 10.21614/sgo-eC-369.
5. Esposito S. Immune system and surgical site infection. J Chemother. 2001;13Supplement-2.12:6.
6. Bajwa SJS, Kulshrestha A. Anaesthesia for laparoscopic surgery: General vs regional anaesthesia. J Minim Access Surg. 2016; 12(1):4-9.
7. Gutt C, Oniu T, Mehrabi A, Schemmer P, Kashfi A, Kraus T, et al. Circulatory and respiratory complications of carbon dioxide
insufflation. Dig Surg. 2004;21(2):95-105.
8. Böttger TC, Hermeneit S, Muller M, Terzic A, Rodehorst A, Elad L, et al. Modifiable surgical and anesthesiologic risk factors for the
development of cardiac and pulmonary complications after laparos-copic colorectal surgery. Surg Endosc. 2009;23(9):2016-25.
9. Agresta F, Ciardo LF, Mazzarolo G, Michelet I, Orsi G, Trentin G, et al. Peritonitis: laparoscopic approach. World J Emerg Surg. 2006;1:9.
10. Litwin DEM, Cahan MA. Laparoscopic cholecystectomy. Surg Clin North Am. 2008;88(6):1295-313, ix.
11. Sanabria A, Villegas MI, Morales Uribe CH. Laparoscopic repair for perforated peptic ulcer disease. Cochrane Database Syst Rev. 2013; (2):CD004778.
12. Wang C-y, Chen D, Zhao G, Zheng H, Chen J-h, Xu P, et al. One-step laparoscopic pancreatic necrosectomy verse surgical step-up approach for infected pancreatic necrosis: a case-control study. World J Emerg Med. 2022;13(4):274-282.
13. Knab LM, Boller AM, Mahvi DM. Cholecystitis. Surg Clin North Am. 2014;94(2):455-70.
14. AL-Naimy TA, Baiomy TA, Oraby EM. How to predict a difficult laparoscopic cholecystectomy? Med. J. Cairo Univ. 2017;85(5):1-6.
15. Yokoe M, Takada T, Strasberg SM, Solomkin JS, Mayumi T, Gomi H, et al. TG13 diagnostic criteria and severity grading of acute
cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2013; 20(1):35-46.
16. Verma S, Agarwal PN, Bali RS, Singh R, Talwar, N. Early versus Delayed Laparoscopic Cholecystectomy for Acute Cholecystitis: A Prospective Randomized Trial. I.S.R.N. Minim. Invasive Surg. 2013, 2013, 1–3.
17. Metwalli AEM, Elaidy MM, Habeeb TAAM. Safety of laparoscopic cholecystectomy among patients with previous upper abdominal surgery. Surg Chron. 2020:25(3):187-191.
18. Habeeb TAAM, Kermansaravi M, Giménez ME, Manangi MN, Elghadban H, Abdelsalam SA, et al. Sleeve Gastrectomy and Cholecystectomy are Safe in Obese Patients with Asymptomatic Cholelithiasis. A Multicenter Randomized Trial. World J Surg. 2022; 46(7):1721-1733.
19. Mannino M, Toro A, Teodoro M, Coccolini F, Sartelli M, Ansaloni L, et al. Open conversion for laparoscopically difficult cholecystectomy is still a valid solution with unsolved aspects. World J Emerg Surg. 2019;14:7.
20. Kelly MD. Laparoscopic retrograde (fundus first) cholecystectomy. BMC Surg. 2009;9:19.
21. Habeeb TAAM, Mohammad H, Mansour MI, Farouk M. Post-
cholecystectomy gallbladder remnant and cystic duct stump stone: surgical pitfalls, causes of occurrence and completion cholecystectomy (open versus laparoscopic) as a safe surgical option of
treatment: short and long term outcome. Randomized Controlled Clinical Trial. Surg. Gastroenterol. Oncol. 2021 eCollection November 03 DOI: 10.21614/sgo-eC-368.
22. Habeeb TAAM, Abdouyassin M, Mehaney Habib F, Baghdadi MA. Emergency laparoscopic cholecystectomy with low-pressure
pneumo-peritoneum in cardiopulmonary risk patients: Fundus-Calot cholecystectomy versus Calot first cholecystectomy. Randomized Controlled Trial. Surg. Gastroenterol. Oncol. 2021 eCollection September 30 DOI:10.21614/sgo-eC-370.
23. Yassin MA, Habeeb TAAM, AShafik mohamed, Said mohamed negm. Laparoscopic cholecystectomy is no more risky in emergent cases with in cardiopulmonary risk: Fundus-Callot cholecystectomy with low pressure pneumo-peritoneum VS open cholecystectomy. Randomized controlled trial. Surg Chron. 2021;26(1):63-68.
24. Coccolini F, Catena F, Pisano M, Gheza F, Fagiuoli S, Di Saverio S, et al. Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. Int J Surg. 2015;18:196-204.
25. Lagoo S, McMahon RL, Kakihara M, Pappas TN, Eubanks S. The sixth decision regarding perforated duodenal ulcer. JSLS. 2002;6(4): 359-68.
26. Kim HC, Yang DM, Kim SW, Park SJ. Gastrointestinal tract perforation: evaluation of M.D.C.T. according to perforation site and elapsed time. Eur Radiol. 2014;24(6):1386-93.
27. Alnaimy TA, Elalfy TR, Elkilany MA. A comparison of laparoscopic and open repair of perforated duodenal ulcer using omental patch: a prospective randomized controlled trial. Kasr El Aini Journal of Surgery. 2018.
28. Matsuda M, Nishiyama M, Hanai T, Saeki S, Watanabe T. Laparoscopic omental patch repair for perforated peptic ulcer. Ann Surg. 1995;221(3):236-40.
29. Lunevicius R, Morkevicius, M. Systematic review comparing
laparoscopic and open repair for perforated peptic ulcer. Br J Surg. 2005;92(10):1195-207.
30. Kim JH, Chin HM, Bae YJ, Jun KH. Risk factors associated with
conversion of laparoscopic simple closure in perforated duodenal ulcer. Int J Surg. 2015;15:40-4.
31. Boxhoorn L, Voermans RP, Bouwense SA, Bruno MJ, Verdonk RC, Boermeester MA, et al. Acute pancreatitis. Lancet. 2020; 396(10252):726-734.
32. Bugiantella W, Rondelli F, Boni M, Stella P, Polistena A, Sanguinetti A, et al. Necrotizing pancreatitis: a review of the interventions. Int J Surg. 2016;28 Suppl 1:S163-71.
33. Gurusamy KS, Belgaumkar AP, Haswell A, Pereira SP, Davidson BR. Interventions for necrotising pancreatitis. Cochrane Database Syst Rev. 2016;4:CD011383.
34. van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Boermeester MA, Dejong CH, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med. 2010; 362(16):1491-502.
35. Tu YL, Jiao HB, Tan XL, Sun LY, Zhang WZ. Laparotomy versus retroperitoneal laparoscopy in debridement and drainage of retroperitoneal infected necrosis in severe acute pancreatitis. Surg Endosc. 2013;27(11):4217-23.
36. Abdelshafy AA, Nagy ME, Elshinawi ME, Ouf TI. Role of laparoscopy in blunt abdominal trauma: A comparative prospective cohort study between laparoscopy and laparotomy in patients with blunt
abdominal trauma. Egypt. J. Surg. 2020;4:926-931.
37. Hassanen A, Abou-Bieh H, Nagib Y. Laparoscopy for the evaluation of anterior abdominal stab wounds in hemodynamically stable patients. EJS. 2009;28:58–61.
38. Leppäniemi A, Salo J, Haapiainen R. Complications of negative laparotomy for truncal stab wounds. J Trauma. 1995;38(1):54-8.
Full Text Sources:
Abstract:
Views: 3644

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.