Surgery, Gastroenterology and Oncology

|
|
Purpose: Patients with Cowden syndrome (CS) have an increased lifetime risk of developing cancers, particularly breast, uterus, thyroid, colon and renal cell cancer. CS is associated with a germline mutation of PTEN, a gene that plays an important role in carcinogenesis. This review hypothesized that inactivation of PTEN could have dramatic consequences on response of treatments in patients with Cowden Syndrome.
Methods: This systematic review has been reported in line with PRISMA and AMSTAR, we investigated to deficit of PTEN and the response to current available treatments for renal cell cancer (RCC).
Results: Preclinical studies showed that PTEN loss determinate a growth level of AKT and mTORC1. For this reason, many studies focused on inhibition of mTOR for treatment of patient with Cowden Syndrome’s. In addition, preclinical data demonstrated that the loss of PTEN is responsible for the increase in vascular endothelial growth factor (VEGF), to suggest that the VEGF antibody bevacizumab in patients with renal cell carcinoma and CS should be indicated.
Conclusion: Cowden syndrome associated renal cell carcinoma patients could benefit from mTOR and anti VEGF therapy, and potentially also by tyrosine kinase inhibitors. Otherwise, immunotherapy the use of would not be recommended. However, confirmatory studies are needed in order to define the role of PTEN as a biomarker of response to treatment.
Introduction
The study of the genetic basis of RCC has led to the identification of at least twelve genes involved in the development of this cancer. Therefore, a single germline alteration may be the cause of the development of RCC in 4-6% of patients. Several of these conditions including VHL, HPRC, BHD, and HLRCC, CS (1).
CS is a rare hereditary syndrome with an estimated incidence of 1 in 200,000 individuals (2). CS patients have an increased lifetime risk of developing cancers, particularly breast, uterus, thyroid and colon cancers (3, 4). The diagnosis is essentially clinical and is based on a combination of pathognomonic, minor and major criteria (5). Genitourinary tumors such as kidney and prostate cancer are associated with CS, in particular RCC considered one of the diagnostic criteria. Skin manifestations are present in almost all patients. The characteristic skin findings of CS are: trichilemmomas, acral keratosis and plantar cavities of the palm. Papillomas of the oral cavity are frequent and generally coalesce giving a “cobblestone appearance”. Macular pigmentation of the glans is also a major diagnostic criterion and may present in almost half of the male patients (6). Gastrointestinal polyps are very common in patients with CS, with a lifetime risk of developing colon cancer of 16%. Histologic types include hamartomatous, hyperplastic, inflammatory, lipomatous, ganglioneuromatous, and adenomatous polyps (2). Patients with CS may experience thyroid disorders with benign and malignant features. In particular, benign pathology occurs in 50-70% of cases and malignant in 14%. The most common histologic subtype of thyroid carcinoma is papillary carcinoma, followed by follicular and anaplastic carcinomas (7). One of the pathognomonic signs of people with CS is macrocephaly. Another cerebral manifestation is the LDD, a dysplastic gangliocytoma of the cerebellum that typically occurs in adulthood. Moreover, some studies suggest that individuals with CS may have varying degrees of cognitive impairment (3,8).
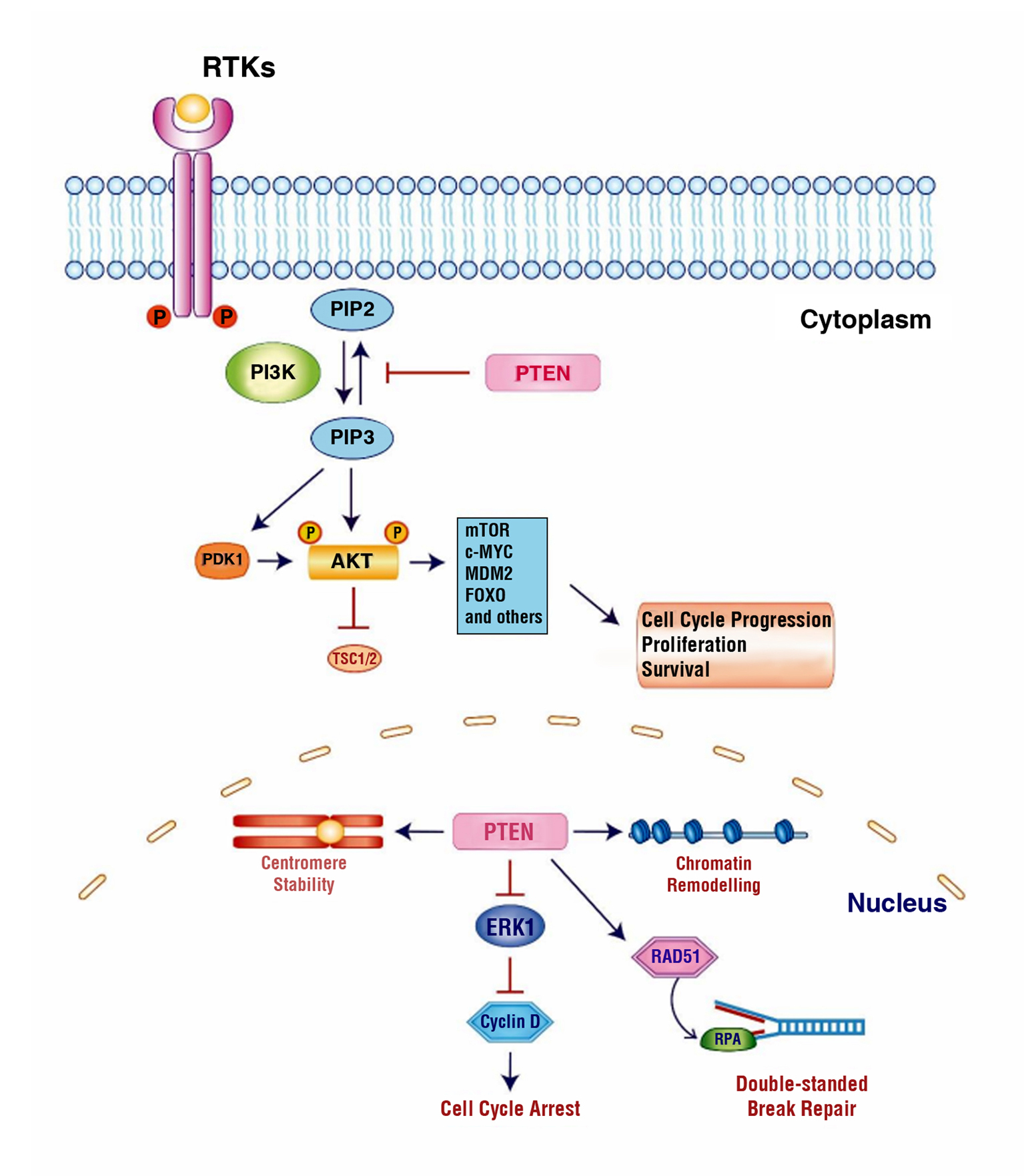
CS is associated with a germline mutation of phosphatase and TENsin homolog deleted on chromosome 10 (PTEN). The gene encodes for a multifunction protein of 403 aminoacidic with lipid and protein phosphatase activities. PTEN plays an important role in numerous cellular processes such as control of cell survivor and proliferation, angiogenesis, cellular motility and regulation of glucoside metabolism (9). All these processes depend of PI3K/AKT/mTOR pathway (fig. 1). In particularly the PI3K is a lipid kinase activated by receptor tyrosine kinases; this converts the PIP2 to PIP3 that recruits PDK1, mTORC2 and finally AKT. PTEN is the most important negative regulator of PI3K signalling. By dephosphorylating PIP3 to PIP2, PTEN reverses the action of PI3K, thereby hampering all downstream functions controlled by the AKT/mTOR axis, such as cycle progression, induction of cell death, regulation of transcription, translation, angiogenesis, and stem cell self-renewal (10). However, PI3K signalling downregulation is a part of a complex system in which PTEN is involved. PTEN can also function as a tumour suppressor in a PI3K independent manner. PTEN protein exists in nuclear form (11), which is able to reduce the activity of Cyclin D1, involved in DNA double-strand damage repair (by interaction with RAD51 protein), delaying the progression of the cell cycle. Furthermore, at the nuclear level it plays an unclear role in the regulation of centrosome stability, mediated by interaction with CENP-C (12).
Figure 1 - Schematic representation of cytoplasmic and nuclear PTEN signaling. In the cytoplasm, PTEN is able to regulate the PI3K/AKT/mTOR signaling pathway by dephosphorylation of PIP3 to PIP2, thus negatively regulating PI3K and leading to inactivation of AKT and hampering AKT-related downstream functions such as cell cycle progression, proliferation and survival. In nucleus, PTEN plays a role in maintaining centromere stability, chromatin remodeling by binding to histone H1, repairing DNA double-strand break by RAD51 protein, and cell cycle control by modulating ERK1 and Cyclin D1 levels.
PTEN has such important role in biology of cancer. This review shows some data known about correlation between deficit of PTEN and the response to current available treatments for RCC.
METHOD
This review has been reported in line with PRISMA (Preferred Reporting Items for Systematic Reviews and MetaAnalyses) and AMSTAR (Assessing the methodological quality of systematic reviews) Guidelines. This systematic review included all clinical and preclinical studies that evaluated the correlation between deficit of PTEN and the response to current available treatments for RCC. A search was performed through MEDLINE and Cochrane Database using a combination of key terms: “Renal cell cancer”, “Cowden syndrome”, “Loss PTEN”, “TKI”, “VEGF”, “PD1/ PDL1”, “mTOR”, “PI3KCA”. Studies were considered eligible in our systematic reviews if they met the following criteria: (1) clinical and preclinical studies evaluating loss PTEN and the response to treatments; (2) retrospective and prospective studies; (3) studies published in English only. The exclusion criteria were: (1) inappropriate study design (conference abstracts, letters to editor and ongoing randomized trial), (2) studies evaluating loss PTEN in the absence of therapeutic correlations, and (3) duplicate publication or provision of insufficient data. The authors reviewed all the eligible studies, according to the inclusion and exclusion criteria. The search strategy was illustrated in the PRISMA flow chart (fig. 2). The Newcastle–Ottawa Scale criterion was used to evaluate the quality of the studies included.
Figure 2 - PRISMA flow chart.

RESULTS
Tyrosine kinase inhibitors and PTEN
In recent studies, it has been evaluated how PTEN mutation can be involved in resistance mechanism induced by targeted receptor tyrosine kinase inhibitor (TKI), the standard treatment in advanced RCC (13,14). Although approximately 70% of patients show an initial response to Sunitinib, later Sunitinib resistance and disease progression occur (15). The Cancer Genome Atlas data showed a correlation between bi-allelic loss of PTEN and poor overall survival in RCC (16,17).
In a study of Hiroshima University, Sekino et al. have studied the association between PTEN expression and therapeutic outcomes in 74 metastatic RCCs treated with Sunitinib and Sorafenib as first-line treatment. They have found negative PTEN expression in 17 of 74 (23%) metastatic RCC patients. Kaplan-Meier analysis revealed a significant association between negative PTEN expression and poor progression-free survival (PFS) in these patients. In particular in the Sunitinib group, negative PTEN expression was significantly associated with poor PFS (p=0.009), whereas in the sorafenib group, there was no association between negative PTEN expression and poor PFS (p=0.744). Sekino et al. also aimed to analyze the effect of PTEN knockout on Sunitinib and Sorafenib resistance in RCC cell lines. They showed that knockout of PTEN induced spheroid formation and promoted Sunitinib and sorafenib resistance in RCC cell lines. Immunohisto-chemistry revealed that negative PTEN expression was correlated with a poor survival outcome of Sunitinib treatment (15).
In another study, Sekino et al. analyzed the involvement of miR-130b in Sunitinib resistance. The authors demonstrated that the over-expression of miR-130b decreased Sunitinib sensitivity in Caki-1 cells whereas the down regulation of miR-130b improved Sunitinib sensitivity in 786-O cells. So, they observed that the expression of miR-130b was inversely correlated with the expression of PTEN inducing Sunitinib resistance in RCC through downregulation of PTEN (18).
Conversely, the RECORD-3 trial has shown that negative PTEN expression was not associated with therapeutic outcomes Sunitinib treatment (19). The primary objective of this study was to assess PFS non-inferiority of first-line Everolimus compared with first-line Sunitinib and to determine the role of first-line mTOR inhibitors in metastatic RCC. The median PFS after first-line Sunitinib was 10.1 months compared with 7.9 months for Everolimus. The median PFS for patients treated with Everolimus followed by Sunitinib was 21.1 months compared with 25.8 months for those treated with Sunitinib followed by Everolimus (HR, 1.4; 95% CI, 1.2–1.8). The median OS for first-line Everolimus followed by Sunitinib was 22.4 months compared with 32.03 months for first-line Sunitinib followed by Everolimus (HR, 1.2; 95% CI, 0.9–1.6). The final OS analysis of RECORD-3 continues to support first-line Sunitinib followed by Everolimus (median OS was 29.5 months compared to 22.4 months for Everolimus followed by Sunitinib). These findings help to explain why the predictive value of PTEN in Sunitinib treatment is controversial. In fact, further studies are necessary to identify the predictive value of PTEN.
Vascular endothelial growth factor inhibitors and PTEN
Many studies have shown that the loss of PTEN is responsible for the increase in VEGF. One of the most potent stimuli for increased VEGF production by tumor cells is hypoxia, because it leads to the induction of HIF-1, leading to the transcription of dozens of target genes, including VEGF (20). Another mechanism is activation of the EGFR/PI3K/AKT/mTOR pathway, that could increase VEGF expression by up regulating HIF-1 (21). For example, PI3K is activated through loss of PTEN, which in glioblastomas results in increased VEGF expression mediated by HIF-1 stabilization (22).
Tian and colleagues exploring the role of PTEN in hepatocellular carcinoma, found similar inhibition of angiogenesis. Using a nude mouse model, was demonstrated that PTEN decreased expression of HIF-1 and VEGF and suppressed angiogenesis induced by human HCC cells with low expression of PTEN. Interestingly, this study also suggested that PTEN regulates angiogenesis through both phosphatase-dependent and independent mechanisms (23).
There are some studies about loss of PTEN and VEGF-Inhibitors also about metastatic colon cancer. Loss of PTEN in these patients was reported in 13-55% of cases (24,25), and it is related to worse prognosis in patients K-RAS wide type (26). These studies demonstrated that in patients with low levels of PTEN, the levels of circulating VEGF increased. In a study conducted on 471 patients, Price et al. (27), aimed to analyse the role of PTEN as a biomarker of therapy in advanced colon cancer. The authors evaluated the prognostic impact of PTEN loss based on copy number alterations, as well as determining the potential for predictive outcomes in patients receiving Bevacizumab treatment. They found that PTEN wasn’t a predictive factor to anti-VEGF therapy and it wasn’t related to progression free survival, overall survival and prognosis. It wasn’t also related to resistance to anti-EGFR therapy. However, the limit of the study was the presence of 94% of primary tumor, which may have reduced the impact of tissue source variation and did not allow them to assess the effect of PTEN loss in metastases on prognosis.
In another study, Sclafani et al. (28) have demonstrated that the lack of PTEN expression in the metastases was an independent predictor of response to treatment with chemotherapy plus bevacizumab. PTEN has been reported to act as a potential biomarker. In particular, PTEN loss has been suggested to be a negative predictive factor for benefit from other targeted agents such as cetuximab in metastatic colon cancer and trastuzumab in metastatic breast cancer. They have not found a significant difference in survival outcomes in their population according to the expression of PTEN.
Koichi Hamada et Coll. had demonstrated that the loss of PTEN specifically in mouse endothelial cells is responsible for enhanced angiogenesis leading accelerated tumour growth (29).
An identical mechanism may be operating in humans with CS. A patient who inherits a mutated PTEN allele is not only at risk for additional tumorigenic mutations due to the loss of PTEN function but may also experience accelerated growth of any incipient tumors due to enhanced angiogenesis.
These preclinical data seem to suggest that the VEGF antibody bevacizumab in patients with renal cell carcinoma and CS should be more indicated than other treatments.
Programmed death-1 receptor and ligands inhibitors and PTEN
Peng et. Coll. have described the role of PTEN loss as a mechanism responsible for resistance to anti PD-1 and PD-L1 treatment (30), which represent an important therapeutic opportunity for patients with metastatic RCC (31). The loss of PTEN modifies the cytokine secretion pattern responsible for the creation of an immune-suppressive microenvironment that promotes tumour progression (32).
Many data have described the ability of PTEN to modulate the level of PD-L1 (33), so the role of PTEN does not seem to be limited only to changes in the tumour microenvironment. The loss of PTEN or constitutive expression of the PI3K/AKT pathway can regulate PD-L1 expression in some tumour types.
The loss of PTEN is responsible for the release from the tumor of anti-inflammatory cytokines which determines a significant reduction of T-cell activity. The presence of infiltrated T-cells in the tumour micro-environment is associated with high percentage of immunotherapy efficacy, including targeting of the immune checkpoint PD1/PD-L1 (34).
The constitutive activation of the PI3K/AKT/mTOR signaling axis, as a consequence of the activation of upstream oncogenic drivers such as NRAS, KRAS, and RET, appear the main mechanism responsible for resistance to immune checkpoint inhibition. Moreover, loss of PTEN function is an alteration responsible for constitutive activation of this signalling, as a consequence of point mutation, gene deletion, or hyper-methylation events (30). This pathway is both active in tumour cells and in the microenvironment, regulating not only cancer growth and dissemination, but also the activity of immune cells inside the tumor and other processes as neovascularization and reorganization of tumour matrix (35).
Trujillo et Coll. (36) described two cases of secondary resistance to immunotherapy with associated acquisition either active β-catenin signaling or PTEN gene deletion in patients with metastatic melanoma. Initially, the patients showed a durable partial response to either a melanoma-peptide/interleukin-12 vaccine or combined anti-CTLA-4 + anti-PD-1 therapy, but sub-sequently developed treatment-resistant metastases. In the first case, the recurrent tumor showed new robust tumour expression of β-catenin, whereas in the second case genomic sequencing revealed acquired PTEN loss.
Mammalian target of rapamycin inhibitors and PTEN
Several studies have hypothesized that the presence of PIK3/PTEN genomic aberrations represents a potential indicator of response to therapy with selective mTOR inhibitors (37). Preclinical studies showed that PTEN loss is responsible for PI3K-AKT signaling activation with increased sensitivity to Everolimus. These findings have enabled researchers to apply mTOR inhibitors in many tumor-types with specific genomic aberrations irrespective of tumor histology and location. It’s known that inactivation of PTEN determinate a growth level of AKT and mTORC1 (mTOR complex 1). For this reason, many studies focused on inhibition of mTOR for chemo-prevention and treatment of patient with Cowden Syndrome’s.
In an interesting study Squarize CH et all. (38) described the effect of rapamycin (mTOR specific inhibitor) in PTEN null murine model (K14Cre PTENF/F mice). These mice, like patients affected by CS, show several cutaneous lesions, alteration in thyroid gland (including thyroid tumors whit follicular aspect) and multiple mammary gland tumor. Mice treated with rapamycin showed regression of muco-cutaneous lesions. Moreover, mice treated before the lesions developed showed reduction of heterologous lesions and reduction of mortality.
Preclinical data (39), in particular studies on mouse models, describe how PTEN loss was associated with behavioral disorders, neuronal function and autism. These data seem to promise a possible therapeutic efficacy of mTOR inhibitors in the neuropsychiatric context.
Komiya et coll. (40) have evaluated if Sirolimus could modulate mTOR signaling and clinical symptoms in CS patients. Fifty-six days treatment with Sirolimus was well tolerated and was associated with some evidence of improvement in symptoms, skin and gastro-intestinal lesions, cerebellar function. Moreover, tissues showed decreased mTOR signaling. These data suggest that Sirolimus may have a role in the prevention of malignancy in patients with CS. Instead, no strong data support the efficacy of mTOR inhibitors in cancer treatment of PTEN loss patient. Kim et coll. investigated the anti-tumour activity of Everolimus in solid tumors but the study did not meet its primary objective of demonstrating the anti-tumour activity in these patients maybe for heterogeneous patient population such as different types of cancer, age and race.
PI3KCA inhibitor in PTEN loss cancer
In the last few years different trials focus on specific catalytic domains of PI3K, in particular sub-unit alpha (codified by PI3KCA gene). PI3K was deregulated in many types of cancer, such as in hormone sensitive breast cancer (HER2 not amplified) in which almost 40% of cases show a gain of function mediated by PI3KCA mutation (41). For this reason, different types of PI3KCA inhibitors were tested but at the moment only one (Alpelisib) shown a good tolerability profile. In the SOLAR1 study a cohort of 63 patients with breast cancer PI3KCA mut (HR+, HER2-) was treated with Alpelisib plus Fulvestrant. These patients shown a significant best PFS respect population treated with Fulvestrant alone (11 moth vs 5.7 moths; HR 0.65; 95% CI, 0.50 to 0.85; P<0.001) (PI3K1). PI3K partway play a central role in kidney cancer to so different inhibitor of PI3KCA was tested.
Likely in the future PI3K inhibitors will use for treat some patients affected by renal cell carcinoma, however in PTEN loss population, specific PI3KCAinhibition could be useful. In their elegant work, Juric and colleagues compared the results of whole genome sequencing (WGS) performed in primary tumor (excised at diagnosis) and several metastatic sites from a patient with a PIK3CA-mutated breast cancer who received Alpelisib. Molecular analysis revealed PTEN loss in all progressing sites (42). Hosford et al. demonstrated in xenografts model of endocrine-resistant breast cancer that PTEN-deficient cancer is strongly dependent on a different sub-unit of PI3K, (sub-unit Beta p110β) (43). This data supports the hypothesis that PTEN deficient cancer need a specific therapeutically approach.
DISCUSSION
Clinicians managing patients with kidney cancer should be familiar with the hereditary RCC syndromes, as the role of inherited predisposition to kidney cancer is most likely underestimated. The diagnosis of an inherited form of RCC is important in the management for the patient, but also to define the correct treatment. CS may be a challenging diagnosis due to the complexity of a clinical diagnosis that requires a combination of pathognomonic, major and minor criteria. Family history of RCC may not provide an indication of a hereditary component for CS. Therefore, clinicians should be aware that family history of RCC or other cancers does not exclude individuals from CS. Those patients with a personal history or clinical manifestations should be considered for genetic counselling.
The prognostic role of PTEN loss in metastatic RCC patients treated with TKI is controversial. Many studies consider the loss of PTEN a cause of resistance to TKI therapy, underlining the better prognosis of PTEN positive patients (17-18). Controversially, RECORD 3 study showed a first-line advantage in OS with Sunitinib followed by Everolimus (19).
Several studies have described that the loss of PTEN results in an increase in VEGF. We showed the benefits in the context of various tumour types (glioblastoma, hepatocarcinoma, colon cancer) and the potential use of PTEN as a biomarker of response.
Clear and unclear renal tumors often present with activation of the PI3K/AKT pathway. Deregulated expression of the PTEN gene is associated with resistance to immune checkpoint inhibition. Moreover, the loss of PTEN expression is associated with alterations of the tumour microenvironment with an increase in the non-inflamed tumor as a consequence of the release of anti-inflammatory cytokines and a significant reduction in the activity of T lymphocytes. In this context, the activity of immune checkpoint inhibitors is ineffective (30,32).
In 2009 Everolimus and Temsirolimus are approved for clinical use in RCC by FDA. Efficacy of MTOR inhibitors is given by the inhibition of the PI3K/AKT pathway as well as by the inhibitory effect on HIF translation. pS6 and pAKT are potential biomarkers of response in Temsirolimus-treated patients with metastatic sporadic RCC. As pS6 and pAKT are dysregulated by the loss of PTEN, those with CS-RCC in whom advanced disease develops may also benefit from mTOR inhibition. Preclinical data demonstrated the benefit that MTOR inhibitors have in terms of chemoprevention in this population. The path of MTOR targeting can potentially be followed in the adjuvant setting (44).
PIK3CA genomic aberrations in patients affected by HR+/HER2 negative Breast Cancer led to the approval of specific inhibitors of sub-unit alpha catalytic domain of PI3K. Similar treatments was tested in patient affected by Renal cell carcinoma. However not significant efficacy was noted. Moreover, pre-clinical data suggest that PTEN null cancer tumor are resistance at these drugs because a different catalytic domain (the sub-unit beta) is involved in hyperactivation of PI3K/PTEN pathway. Recently was tested BKM120 (a PI3K beta inhibitor) in combination with bevacizumab in patient affected by glyoblastoma (45). This combination could be very efficacy in patient with PTEN null mutation, however a great toxicity was observed so introduction in clinical practice seems very far.
CONCLUSION
In the present study, we explored the potential role of PTEN in patients with CS-RCC. Data showed potentially benefit of use of mTOR and VEGF inhibitors in these patients, and potentially also by TKIs (table 1). However, further confirmatory studies are needed to identify the mTOR inhibitors as the treatment of choice for RCC-CS patients. Moreover, the role of PTEN loss as a potential response biomarker and a predictor of response appears to be proposed only by pre-clinical data (46). Therefore, there is an emergent need to identify predictive markers of response that may be useful to prospectively select patients bearing tumours which may respond and benefit from mTOR inhibition therapies.
Table 1 - Loss PTEN and the response to treatments.

Author’s Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Lanzafame Katia, Inzerilli Nicola and Rosaria Carciotto. The first draft of the manuscript was written by Claudio Longhitano, Lorenzo Rossi and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest and Source of Funding
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval
The approval of a research ethic committee is not required, since this review was conducted without any direct or indirect intervention on patients.
REFERENCES
1.Shuch B, Ricketts CJ, Vocke CD, Komiya T, Middelton LA, Kauffman EC, et al. Germline PTEN mutation Cowden syndrome: an under-appreciated form of hereditary kidney cancer. J Urol. 2013;190(6): 1990-8.
2.Cauchin E, Touchefeu Y, Matysiak-Budnik T. Hamartomatous Tumors in the Gastrointestinal Tract. Gastrointest Tumors. 2015; 2(2):65-74.
3.Gammon A, Jasperson K, Champine M. Genetic basis of Cowden syndrome and its implications for clinical practice and risk management. Appl Clin Genet. 2016;9:83-92.
4.Pilarski R, Burt R, Kohlman W, Pho L, Shannon KM, Swisher E. Cowden syndrome and the PTEN hamartoma tumor syndrome: systematic review and revised diagnostic criteria. J Natl Cancer Inst. 2013;105(21):1607-16.
5.Ngeow J, Eng C. Germline PTEN Mutation Analysis for PTEN Hamartoma Tumor Syndrome. Methods Mol Biol. 2016;1388:63-73.
6.Lopes S, Vide J, Moreira E, Azevedo F. Cowden syndrome: clinical case and a brief review. Dermatol Online J. 2017;23(8):13030/ qt0023k3x0.
7.Cameselle-Teijeiro J, Fachal C, Cabezas-Agrícola JM, Alfonsín-Barreiro N, Abdulkader I, Vega-Gliemmo A, et al. Thyroid Pathology Findings in Cowden Syndrome: A Clue for the Diagnosis of the PTEN Hamartoma Tumor Syndrome. Am J Clin Pathol. 2015;144(2):322-8.
8.Seol JE, Park IH, Lee W, Kim H, Seo JK, Oh SH. Cowden Syndrome with a Novel Germline PTEN Mutation and an Unusual Clinical Course. Ann Dermatol. 2015;27(3):306-9.
9.Pilarski R. PTEN Hamartoma Tumor Syndrome: A Clinical Overview. Cancers (Basel). 2019;11(6):844.
10.Milella M, Falcone I, Conciatori F, Cesta Incani U, Del Curatolo A, Inzerilli N, et al. PTEN: Multiple Functions in Human Malignant Tumors. Front Oncol. 2015;5:24.
11.Sun Z, Huang C, He J, Lamb KL, Kang X, Gu T, et al. PTEN C-terminal deletion causes genomic instability and tumor development. Cell Rep. 2014;6(5):844-54.
12.Shen WH, Balajee AS, Wang J, Wu H, Eng C, Pandolfi PP, et al. Essential role for nuclear PTEN in maintaining chromosomal integrity. Cell. 2007;128(1):157-70.
13.Atkins MB, Tannir NM. Current and emerging therapies for first-line treatment of metastatic clear cell renal cell carcinoma. Cancer Treat Rev. 2018;70:127-137.
14.Vuorinen RL, Paunu N, Turpeenniemi-Hujanen T, Reunamo T, Jekunen A, Kataja V, et al. Sunitinib first-line treatment in metastatic renal cell carcinoma: costs and effects. Anticancer Res. 2019; 39(10):5559-5564.
15.Sekino Y, Hagura T, Han X, Babasaki T, Goto K, Inoue S, et al (2020). PTEN Is Involved in Sunitinib and Sorafenib Resistance in Renal Cell Carcinoma. Anticancer Res. 2020;40(4):1943-1951.
16.Lee HJ, Lee HY, Lee JH, Lee H, Kang G, Song JS, et al. Prognostic significance of biallelic loss of pten in clear cell renal cell carcinoma. J Urol. 2014;192(3):940-6.
17.Ricketts CJ, De Cubas AA, Fan H, Smith CC, Lang M, Reznik E, et al (2018). The cancer genome atlas comprehensive molecular characterization of renal cell carcinoma. Cell Rep. 2018;23(1):313-326.e5.
18.Sekino Y, Sakamoto N, Sentani K, Oue N, Teishima J, Matsubara A, et al. miR-130b Promotes Sunitinib Resistance through Regulation of PTEN in Renal Cell Carcinoma. Oncology. 2019;97(3):164-172.
19.Motzer RJ, Barrios CH, Kim TM, Falcon S, Cosgriff T, Harker WG, et al. (2014). Phase II randomized trial comparing sequential first-line everolimus and second-line sunitinib versus first-line sunitinib
and second-line everolimus in patients with metastatic renal cell carcinoma. J Clin Oncol. 2014;32(25):2765-72.
20.Blancher C, Harris AL. The molecular basis of the hypoxia response pathway: tumour hypoxia as a therapy target. Cancer Metastasis Rev. 1998;17(2):187-94.
21.Blancher C, Moore JW, Robertson N, Harris AL. Effects of ras and von Hippel-Lindau (VHL) gene mutations on hypoxia-inducible factor (HIF)-1alpha, HIF-2alpha, and vascular endothelial growth factor expression and their regulation by the phosphatidylinositol 3'-kinase/Akt signaling pathway. Cancer Res. 2001;61(19):7349-55.
22.Zundel W, Schindler C, Haas-Kogan D, Koong A, Kaper F, Chen E, et al (2000). Loss of PTEN facilitates HIF-1-mediated gene expression. Genes Dev. 2000;14(4):391-6.
23.Tian T, Nan KJ, Wang SH, Xuan Liang, Chuang-Xin Lu, Hui Guo, et al. PTEN regulates angiogenesis and VEGF expression through phosphatase-dependent and -independent mechanisms in HepG2 cells. Carcinogenesis. 2010;31(7):1211-9.
24.Wang ZH, Gao QY, Fang JY. Loss of PTEN expression as a predictor of resistance to antiEGFR monoclonal therapy in metastatic colo-rectal cancer: evidence from retrospective studies. Cancer Chemother Pharmacol. 2012;69(6):1647-55.
25.Naguib A, Cooke JC, Happerfield L, Kerr L, Gay LJ, Luben RN, et al. Alterations in PTEN and PIK3CA in colorectal cancers in the EPIC Norfolk study: associations with clinicopathological and dietary factors. BMC Cancer. 2011;11:123.
26.Laurent-Puig P, Cayre A, Manceau G, Buc E, Bachet JB, Lecomte T, et al. Analysis of PTEN, BRAF, and EGFR status in determining benefit from cetuximab therapy in wild-type KRAS metastatic colon cancer. J Clin Oncol. 2009;27(35):5924-30.
27.Price TJ, Hardingham JE, Lee CK, Townsend AR, Wrin JW, Wilson K, et al. Prognostic impact and the relevance of PTEN copy number alterations in patients with advanced colorectal cancer (CRC)
receiving bevacizumab. Cancer Med. 2013;2(3):277-85.
28.Sclafani F, Rimassa L, Colombo P, Destro A, Stinco S, Lutman FR, et al. An exploratory biomarker study in metastatic tumors from colorectal cancer patients treated with bevacizumab. Int J Biol Markers. 2015;30(1):e73-80.
29.Hamada K, Sasaki T, Koni PA, Natsui M, Kishimoto H, Sasaki J, et al (2005). The PTEN/PI3K pathway governs normal vascular development and tumor angiogenesis. Genes Dev. 2005;19(17):2054-65.
30.Peng W, Chen JQ, Liu C, Malu S, Creasy C, Tetzlaff MT, et al. Loss of PTEN Promotes Resistance to T CellMediated Immunotherapy. Cancer Discov. 2016;6(2):202-16.
31.Motzer RJ, Escudier B, McDermott DF, George S, Hammers HJ, Srinivas S, et al. CheckMate 025 Investigators (2015). Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1803-13.
32.Roh W, Chen PL, Reuben A, Spencer CN, Prieto PA, Miller JP, et al. Integrated molecular analysis of tumor biopsies on sequential CTLA-4 and PD-1 blockade reveals markers of response and resistance. Sci Transl Med. 2017;9(379):eaah3560.
33.Song M, Chen D, Lu B, Wang C, Zhang J, Huang L, et al. PTEN loss increases PD-L1 protein expression and affects the correlation between PD-L1 expression and clinical parameters in colorectal cancer. PLoS One. 2013;8(6):e65821.
34.Cretella D, Digiacomo G, Giovannetti E, Cavazzoni A. PTEN Alterations as a Potential Mechanism for Tumor Cell Escape from PD-1/PD-L1 Inhibition. Cancers (Basel). 2019;11(9):1318.
35.Sun C, Mezzadra R, Schumacher TN. Regulation and Function of the PD-L1 Checkpoint. Immunity. 2018;48(3):434-452.
36.Trujillo JA, Luke JJ, Zha Y, Segal JP, Ritterhouse LL, Spranger S, et al. Secondary resistance to immunotherapy associated with b-catenin pathway activation or PTEN loss in metastatic melanoma. J Immunother Cancer. 2019;7(1):295.
37.Rodrigues HV, Ke D, Lim J, Stephen B, Bellido J, Janku F, et al (2015). Phase I combination of pazopanib and everolimus in PIK3CA mutation positive/PTEN loss patients with advanced solid tumors refractory to standard therapy. Invest New Drugs. 2015;33(3):700-9.
38.Squarize CH, Castilho RM, Gutkind JS. Chemoprevention and treatment of experimental Cowden's disease by mTOR inhibition with rapamycin. Cancer Res. 2008;68(17):7066-72.
39.Tilot AK, Frazier TW 2nd, Eng C. Balancing Proliferation and Connectivity in PTEN-associated Autism Spectrum Disorder. Neurotherapeutics. 2015;12(3):609-19.
40. Komiya T, Blumenthal GM, De Chowdhury R, Fioravanti S, Ballas MS, Morris J, et al (2019). A Pilot Study of Sirolimus in Subjects with Cowden Syndrome or Other Syndromes Characterized by Germline Mutations in PTEN. Oncologist. 2019;24(12):1510-e1265.
41.André F, Ciruelos E, Rubovszky G, Campone M, Loibl S, Rugo HS, et al (2019); SOLAR-1 Study Group. Alpelisib for PIK3CAMutated, Hormone Receptor-Positive Advanced Breast Cancer. N Engl J Med. 2019;380(20):1929-1940.
42.Juric D, Castel P, Griffith M, Griffith OL, Won HH, Ellis H, et al. Convergent loss of PTEN leads to clinical resistance to a PI(3)Ka inhibitor. Nature. 2015;518(7538):240-4.
43.Hosford SR, Dillon LM, Bouley SJ, Rosati R, Yang W, Chen VS, et al. Combined Inhibition of Both p110a and p110b Isoforms of Phosphatidylinositol 3-Kinase Is Required for Sustained Therapeutic Effect in PTENDeficient, ER+ Breast Cancer. Clin Cancer Res. 2017;23(11):2795-2805.
44.Shuch B, Ricketts CJ, Vocke CD, Komiya T, Middelton LA, Kauffman EC, et al. Germline PTEN mutation Cowden syndrome: an underappreciated form of hereditary kidney cancer. J Urol. 2013;190(6):1990-8.
45.Hainsworth JD, Becker KP, Mekhail T, Chowdhary SA, Faulkner Eakle J, Wright D, et al. Phase I/II study of bevacizumab with BKM120, an oral PI3K inhibitor, in patients with refractory solid tumors (phase I) and relapsed/refractory glioblastoma (phase II). J Neurooncol. 2019;144(2):303-311.
46.Pópulo H, Lopes JM, Soares P. The mTOR signalling pathway in human cancer. Int J Mol Sci. 2012;13(2):1886-1918.
Full Text Sources:
Abstract:
Views: 2479

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.