Surgery, Gastroenterology and Oncology

|
|
Background: Liver incidentalomas are frequently encountered in gastroenterology practice due to enhanced imaging technology capabilities. Benign focal liver lesions are commonly detected in hospital patients undergoing ultrasound (US) examinations, with simple hepatic cysts being the most frequent finding. This study aimed to assess the prevalence, management, and outcomes of liver incidentalomas in gastroenterology practice and determine alignment with current standards of care.
Methods: A retrospective study was conducted on 591 individuals aged 18 years or older who visited the gastroenterology clinic at Alhabib Medical Group, Qassim, from January 2020 to June 2023. Participants were divided into an incidentaloma group (n=62) and control group (n=529). Electronic medical records were systematically reviewed for hepatic incidentalomas, lesion characteristics, and follow-up management.
Results: Alkaline phosphatase (ALP) levels were significantly elevated in the incidentaloma group (102.26 ± 89.45 U/L) compared to controls (77.13 ± 46.48 U/L, p=0.033). CT utilization was higher in the incidentaloma group (56.45% vs 22.12%, p<0.001). Fatty liver disease prevalence was lower in the incidentaloma group (22.58% vs 50.09%, p<0.001).
Conclusion: Liver incidentalomas demonstrate distinct clinical and biochemical characteristics, with ALP serving as a potential biomarker for further investigation.
INTRODUCTION
Incidentalomas, which are described as unexpected or unrelated radiographic findings, have become more common because to the extensive use of abdominal imaging. These results were not originally intended to be part of the research (1).
Globally, the prevalence of liver incidentalomas varies depending on patient population, imaging modality, and underlying disease burden (2). In regions with high rates of chronic liver disease and viral hepatitis, such as the Middle East, the likelihood that an incidental lesion may represent significant pathology is heightened (3). The Saudi Arabia, in particular, has witnessed evolving epidemiological patterns of liver disease, shaped by the interplay of hepatitis B virus (HBV), hepatitis C virus (HCV), metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD), and the rising burden of obesity and diabetes. Within this context, incidental hepatic findings carry profound clinical implications: distinguishing benign lesions from those requiring urgent intervention can influence survival, health resource utilization, and healthcare policy (4).
Imaging studies may discover incidentalomas at varying frequencies; the greatest rates are shown in chest computed tomography (45%), computed tomography (CT) (38%), and cardiac magnetic resonance imaging (MRI) (34%) (5).
Incidentalomas most often occur in the following areas: pituitary (1 in 10 cases), thyroid (up to 50% of cases), lungs (8 to 51%), liver (15%), pancreas (2% of cases), adrenal glands (3 to 4%) and kidneys (up to 33% in older persons) (6). The recommended imaging modality for screening hepatocellular carcinoma (HCC) in cirrhotic patients is Ntransabdominal ultrasound (TUS). Technical limitations, lack of expertise among technologists, irregular liver texture, steatosis, and obesity all work against TUS's ability to identify HCC (7). With TUS, the sensitivity for early lesion detection of HCC is 63%. For lesions less than 2 cm in diameter, MRI is more sensitive than TUS (84.8% vs. 27.3%) (8). The American Association for the Study of Liver Diseases (AASLD) now recommends TUS for HCC monitoring, even though MRI offers superior sensitivity. The shortcomings of TUS have led many liver transplant facilities to switch to MRI as their screening tool of choice (9-11).
This study aimed to describe the prevalence and spectrum of liver incidentalomas encountered in a real-world cohort and to examine the diagnostic strategies employed, including imaging modalities and laboratory investigations.
PATIENTS AND METHODS
A retrospective study design was conducted on 591 individuals aged 18 years or older who had visited the gastroenterology clinic during the specified study period who had undergone imaging studies including US, CT or MRI for reasons unrelated to liver conditions and who subsequently demonstrated incidental findings of liver lesions at gastroenterology practice setting at Alhabib Medical Group at Qassim from January 2020 to June 2023 after approval from Ethical Committee (Approval No: HAP-01-R-082).
Participants were divided into an incidentaloma group (n=62), and control group (n=529).
Exclusion Criteria
Patients were applied to eliminate patients with known liver conditions at the time of imaging, as well as those with a documented history of cancer, to ensure the identification of truly incidental findings rather than expected pathology.
Electronic medical records from the Cloud Solutions system were utilized as the primary data source for this investigation.
Patient records were systematically reviewed to identify the presence of hepatic incidentalomas, with detailed documentation of lesion size and anatomical location. Follow-up management strategies were recorded, including subsequent imaging studies and surgical referrals when indicated. Demographic variables were extracted including patient age, sex, body mass index (BMI), and relevant comorbidities to ensure comprehensive characterization of the study population.
Clinical presentation data were collected to document the symptoms that prompted the initial imaging workup, specifically focusing on gastro-intestinal complaints including nausea, vomiting, abdominal pain, and changes in bowel habits.
Statistical Analysis
Statistical analysis was done by SPSS v27 (IBM©, Armonk, NY, USA). Shapiro-Wilks test and histograms were used to evaluate the normality of the distribution of data. Quantitative parametric data were presented as mean and standard deviation (SD) and were analyzed by unpaired student t-test. Qualitative variables were presented as frequency and percentage and analyzed using the Chi-square test or Fisher's exact test when appropriate. A two-tailed p value ?0.05 was considered statistically significant.
Results
The prevalence of hepatic incidentalomas was recorded in 62 (10.5 %) patients.
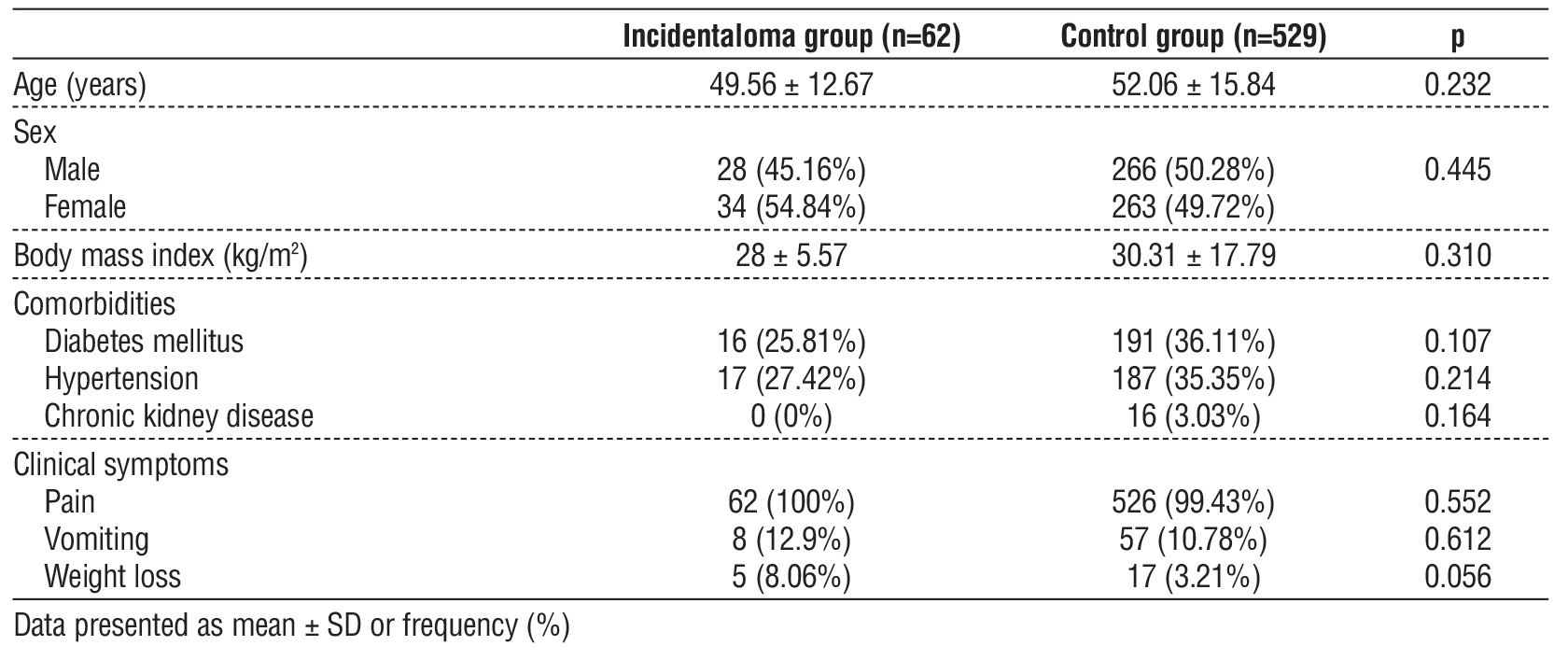
Age, sex, BMI, comorbidities and clinical symptoms were insignificantly different between both groups (table 1).
Table 1 - Demographic data and comorbidities of the studied groups
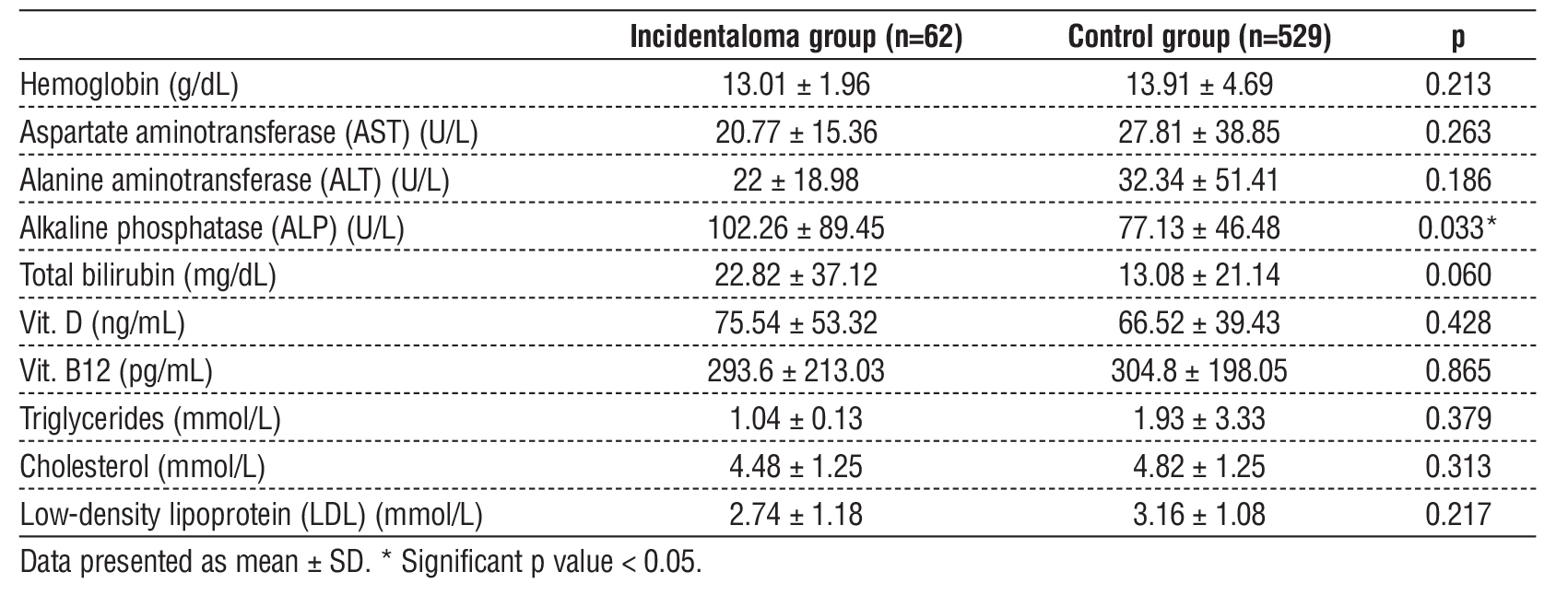
Hb, AST, ALT, total bilirubin, vitamin D, vitamin B12, TG, cholesterol and LDL were insignificantly different between both groups. ALP was significantly higher in the incidentaloma group than control group (P value=0.033) (table 2).
Table 2 - Laboratory investigation of the studied groups
Performing of US and CT were significantly lower in the incidentaloma group than control group (p value < 0.001). Liver lesions by US and CT were significantly higher in the incidentaloma group than control group (p value < 0.001). Liver size by US was (3.4 ± 7.69 x 1.7 ± 1.52) cm while liver size by CT was (3.4 ± 3.35 x 2.9 ± 2.75) cm. MRI was significantly higher in the incidentaloma group than control group (p value < 0.001). Liver lesion by MRI were insignificantly different between both groups (table 3).
Table 3 - Imaging findings of the studied groups
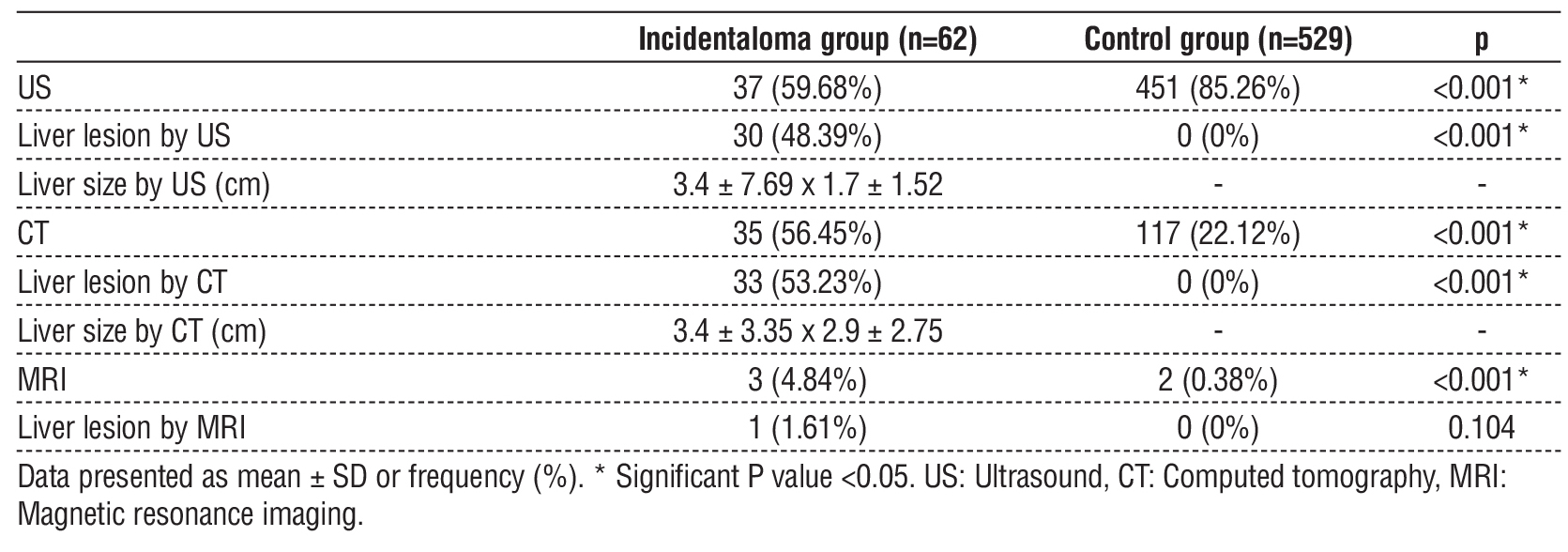
Table 4 - Radiological characteristics of incidental liver lesions in the incidentaloma group
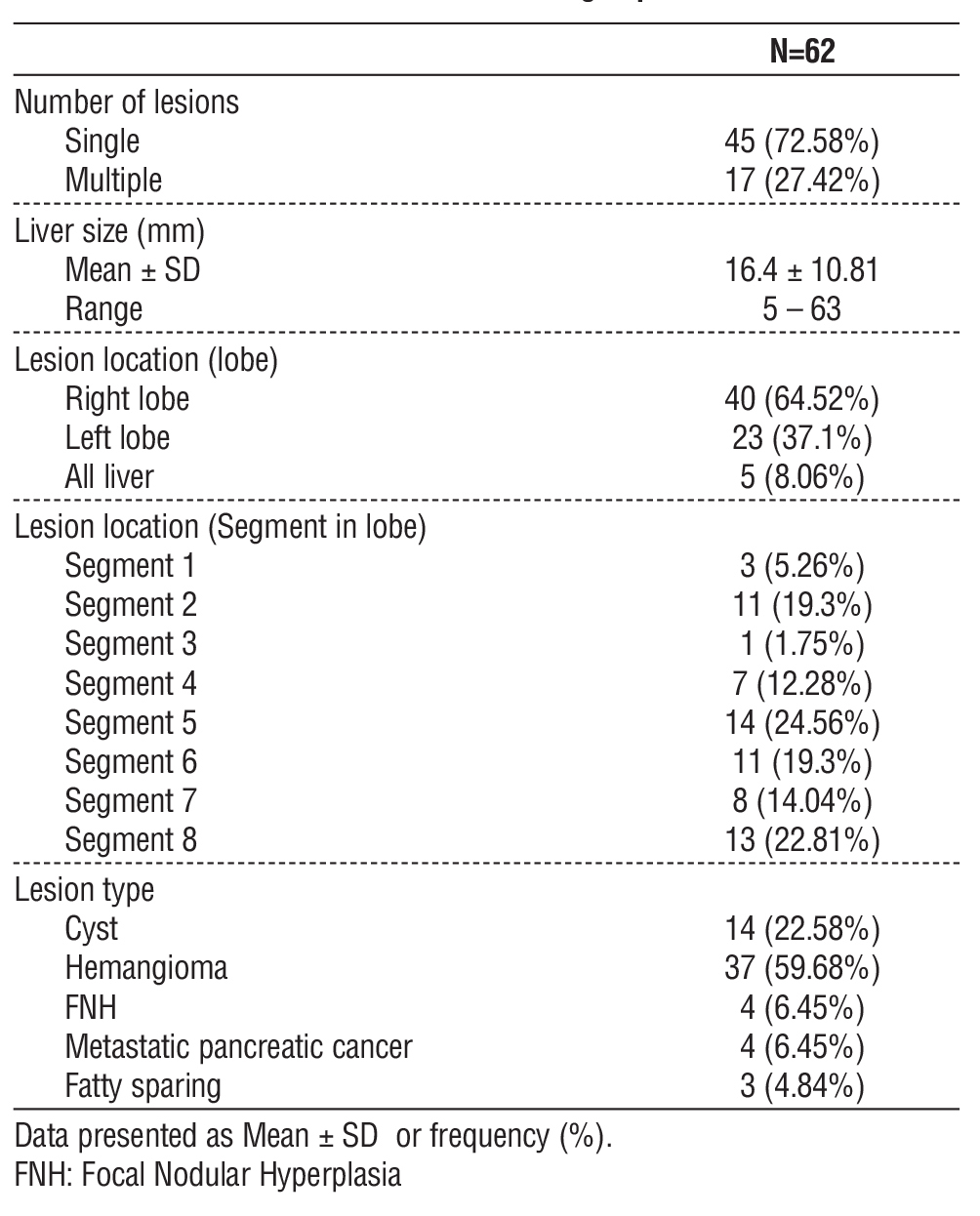
Number of lesions were single in 45 (72.58%) patients and multiple in 17 patients (27.42%). Liver size ranged from 5 to 63 mm with mean value was 16.4 ± 10.81) mm. Lesion location was in the right lobe in 40 patients (64.52%), left lobe in 23 patients (37.1%),
and involving the whole liver in 5 patients (8.06%). Segmental distribution was in segment 1 in 3 (5.26%) patients, segment 2 in 11 (19.3%) patients, segment 3 in 1 (1.75%) patient, segment 4 in 7 (12.28%) patients, segment 5 in 14 (24.56%) patients, segment 6 in 11 (19.3%) patients, segment 7 in 8 (14.04%) patients, and segment 8 in 13 (22.81%) patients. Lesion types were hemangioma in 37 patients (59.68%), cyst in 14 (22.58%), focal nodular hyperplasia (FNH) in 4 (6.45%), metastatic pancreatic cancer in 4 (6.45%), and fatty sparing in 3 (4.84%) (table 4).
Fatty liver was significantly lower in the incidentaloma group than control group (p value < 0.001). Follow up was significantly higher in the incidentaloma group than control group (p < 0.05) (table 5).
Table 5 - Fatty liver and follow up of the studied groups

DISCUSSION
The widespread implementation of advanced imaging technologies in contemporary clinical practice has resulted in a substantial increase in the detection of incidental liver lesions, fundamentally altering the landscape of hepatic pathology diagnosis and management (12,13).
The present study demonstrates a significant elevation in ALP levels among patients with liver incidentalomas (102.26 ± 89.45 U/L) compared to controls (77.13 ± 46.48 U/L, p=0.033), while other liver enzymes including AST, ALT, and total bilirubin remained comparable between groups. This finding aligns with the broader understanding that liver incidentalomas may represent subclinical pathological processes that manifest through subtle biochemical alterations rather than overt clinical symptoms (14). The selective elevation of ALP, in the absence of significant changes in hepatocellular enzymes, suggests that incidental liver lesions may be associated with biliary tract involvement or space-occupying effects that preferentially affect this enzyme system. This biochemical pattern is particularly relevant given that ALP elevation can indicate various hepatic conditions including mass lesions that may not immediately manifest through conventional liver function para-meters (13).
The imaging utilization patterns revealed significant differences between study groups, with US examination performed in 59.68% of incidentaloma patients versus 85.26% of controls (p<0.001). This inverse relationship suggests that US may serve as an initial screening tool that, when negative, reduces the likelihood of detecting incidental findings, consistent with the observations by Sluijter et al. (15) who reported that 49.2% of abdominal US examinations during on-call hours were negative. The exclusive detection of liver lesions by US in the incidentaloma group (48.39% versus 0% in controls) underscores the diagnostic value of this modality in identifying hepatic abnormalities, particularly when clinical suspicion is low. The mean lesion dimensions detected by US (3.4 ± 7.69 cm in length and 1.7 ± 1.52 cm in width) fall within the range where diagnostic uncertainty often necessitates further evaluation, as suggested by the management thresholds proposed by Berland et al. (16) for various hepatic lesions.
CT utilization showed a contrasting pattern, with higher usage in the incidentaloma group (56.45%) compared to controls (22.12%, p<0.001). This trend likely reflects the need for advanced imaging characteri-zation when initial studies suggest abnormalities or when clinical presentation warrants cross-sectional imaging. The CT-detected lesions measured 3.4 ± 3.35 cm in length and 2.9 ± 2.75 cm in width, dimensions that correspond to the size thresholds where malignancy risk increases and surgical intervention may be considered, as demonstrated by Liu et al. (17) who found that tumor size greater than 4 cm was an independent predictive factor for malignant disease in hepatic incidentalomas. The limited utilization of MRI in both groups (4.84% in incidentaloma group versus 0.38% in controls) reflects its specialized role in hepatic lesion characterization, typically reserved for cases where CT findings remain indeterminate or when specific tissue characterization is required (18).
Our findings demonstrate that hepatic incidentalomas constitute a substantial proportion of imaging findings
in gastroenterology practice, with hemangiomas representing the predominant benign lesion type at 59.68%, followed by cysts at 22.58%. This distribution aligns with established literature showing hemangiomas as the most common benign hepatic lesion detected incidentally (17,19). The observed mean lesion size of 16.4 mm corresponds with previous studies indicating that most incidental hepatic lesions fall within the small-to-moderate size range requiring careful diagnostic consideration (16). The predominance of right lobe involvement (64.52%) mirrors anatomical expectations given the larger volume of hepatic parenchyma in this location. Our malignancy rate of 6.45% falls within the range reported by Koea, (19) who documented 10% malignancy rates for both hypervascular and hypovascular incidental lesions. The detection of focal nodular hyperplasia in 6.45% of cases supports previous observations by Liu et al. (17) regarding the spectrum of benign pathologies encountered in hepatic incidentalomas, emphasizing the critical importance of appropriate imaging characterization and multidisciplinary management approaches.
A significant lower fatty liver disease prevalence in the incidentaloma group (22.58%) compared to controls (50.09%, p<0.001) represents a notable departure from expected patterns and warrants careful interpretation. The lower prevalence of fatty liver disease in the incidentaloma group may reflect the fact that these lesions represent focal pathological processes rather than diffuse metabolic liver disease, consistent with the observations by Koea (19) who noted that hepatic incidentalomas constitute a distinct clinical entity with specific diagnostic and management considerations.
This finding also aligns with the concept that incidental liver lesions may represent a different spectrum of hepatic pathology, potentially including focal nodular hyperplasia, hemangiomas, or other benign lesions that do not typically coexist with fatty liver disease (20).
The minimal follow-up requirements observed in the incidentaloma group (1.61% versus 0% in controls, p=0.003) suggest that the majority of detected lesions were likely characterized as benign or low-risk based on initial imaging findings. This pattern is consistent with the natural history of most hepatic incidentalomas, which are predominantly benign and require only observation or limited follow-up (21). The low follow-up rate may reflect the effectiveness of current imaging protocols in distinguishing between benign and potentially malignant lesions, reducing the need for extensive surveillance in most cases.
However, this trend also highlights the importance of appropriate risk stratification and the application of evidence-based management guidelines for hepatic incidentalomas. The work by Berland et al. (16) emphasized the need for systematic approaches to incidental findings, with specific management algorithms based on lesion characteristics, patient risk factors, and imaging features. The low follow-up rate may reflect challenges in managing incidental findings, requiring careful balance between necessary surveillance and avoiding overtreatment, based on individual patient context and lesion features.
Limitations
The small incidentaloma cohort in this retrospective single-center study limits its generalizability and introduces inherent selection bias. Reliance on electronic records risks documentation inaccuracies and incomplete follow-up data. Variability in imaging protocols and indications may affect lesion characterization. Exclusion of cancer history patients might overlook relevant associations.
CONCLUSIONS
The study identified significantly elevated ALP in incidentalomas, suggesting subclinical biliary involvement. Incidentaloma patients underwent fewer US but more CT/MRI, with lesions averaging 3-4 cm. Unexpectedly, fatty liver prevalence was lower in incidentalomas. Minimal follow-up implies most lesions were initially deemed benign.
Authors’ Contribution
I contributed to the study conception and design. Material preparation, data collection and analysis were performed by me. The first draft of the manuscript was written by me and I commented on previous versions of the manuscript. I read and approved the final manuscript.
Conflicts of Interest: Not applicable
Source of Funding: Not applicable
REFERENCES
1. Brady A. Incidentalomas, SPEW, and VOMIT-radiological dyspepsia? Eur Radiol. 2020;30(9):4968-73.
2. ?irli R, Popescu A, Jenssen C, Möller K, Lim A, Dong Y, et al. WFUMB Review Paper. Incidental Findings in Otherwise Healthy Subjects, How to Manage: Liver. Cancers (Basel). 2024;16(16):651-84.
3. Al Ta’ani O, Aleyadeh W, Al-Ajlouni Y, Alnimer L, Ismail A, Natour B, et al. The burden of cirrhosis and other chronic liver disease in the middle east and North Africa (MENA) region over three decades. BMC Public Health. 2024;24(1):2979-84.
4. Alqahtani SA, Abaalkhail F, Alghamdi S, Bzeizi K, Al-Hamoudi WK, Paik JM, et al. The burden of metabolic dysfunction-associated steatotic liver disease and viral hepatitis in Saudi Arabia. Saudi J Gastroenterol. 2024;30(5):310-8.
5. O'Sullivan JW, Muntinga T, Grigg S, Ioannidis JPA. Prevalence and outcomes of incidental imaging findings: umbrella review. BMJ. 2018;361(8):2387-92.
6. Hitzeman N, Cotton E. Incidentalomas: initial management. Am Fam Physician. 2014;90(11):784-9.
7. Esfeh JM, Hajifathalian K, Ansari-Gilani K. Sensitivity of ultrasound in detecting hepatocellular carcinoma in obese patients compared to explant pathology as the gold standard. Clin Mol Hepatol. 2020; 26(1):54-9.
8. Kim SY, An J, Lim YS, Han S, Lee JY, Byun JH, et al. MRI with liver-specific contrast for surveillance of patients with cirrhosis at high risk of hepatocellular carcinoma. JAMA Oncol. 2017;3(4):456-63.
9. Kim HL, An J, Park JA, Park SH, Lim YS, Lee EK. Magnetic resonance imaging is cost-effective for hepatocellular carcinoma surveillance in high-risk patients with cirrhosis. Hepatology. 2019; 69(4):1599-613.
10. An JY, Peña MA, Cunha GM, Booker MT, Taouli B, Yokoo T, et al. Abbreviated MRI for Hepatocellular Carcinoma Screening and Surveillance. Radiographics. 2020;40(7):1916-31.
11. Ganne-Carrié N, Piscaglia F. Non-enhanced MRI surveillance for HCC: A new tool for all, none or selected patients at risk? J Hepatol. 2020;72(4):607-9.
12. Costanzo R, Scalia G, Strigari L, Ippolito M, Paolini F, Brunasso L, et al. Nuclear medicine imaging modalities to detect incidentalomas and their impact on patient management: A systematic review. J Cancer Res Clin Oncol. 2024;150(7):368.
13. Pickhardt PJ. Incidentalomas at abdominal imaging. Br J Radiol. 2023;96(1142):20211167.
14. Fergusson J. Investigation and management of hepatic incidentalomas. J Gastroenterol Hepatol. 2012;27(12):1772-82.
15. Sluijter TE, Yakar D, Kwee TC. On-call abdominal ultrasonography: The rate of negative examinations and incidentalomas in a European tertiary care center. Abdom Radiol. 2022;47(7):2520-6.
16. Berland LL, Silverman SG, Gore RM, Mayo-Smith WW, Megibow AJ, Yee J, et al. Managing incidental findings on abdominal CT: White paper of the ACR incidental findings committee. J Am Coll Radiol. 2010;7(10):754-73.
17. Liu CL, Fan ST, Lo CM, Chan SC, Tso WK, Ng IO, et al. Hepatic resection for incidentaloma. J Gastrointest Surg. 2004;8(7):785-93.
18. Haring MP, Cuperus FJ, Duiker EW, de Haas RJ, de Meijer VE. Scoping review of clinical practice guidelines on the management of benign liver tumours. BMJ Open Gastro. 2021;8(1):e000592.
19. Koea JB. Hepatic incidentaloma: The rule of tens. HPB. 2013;15(5): 379-83.
20. Ehrl D, Rothaug K, Herzog P, Hofer B, Rau H-G. “Incidentaloma” of the liver: Management of a diagnostic and therapeutic dilemma. HPB Surg. 2012;2012(1):891787.
21. Zülke C, Schlitt H. Incidentalomas of the liver and gallbladder. Der Chirurg. 2007;78(8):698-712.
Full Text Sources:
Abstract:
Views: 1204

For Authors
Journal Subscriptions

Dec 2025
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.