Surgery, Gastroenterology and Oncology

|
|
Background: The purpose of this study is to determine if post-operative administration of dexamethasone reduces the risk of postoperative hypocalcemia and low parathyroid hormone levels.
Methods: We compared 2 groups of patients (group A and group B). Group A received post operative dexamethasone post operatively and group B didn’t receive any glucocorticoids post operatively. Calcium and parathyroid hormone levels were measured pre and post
operatively, patients were followed up for 30 days post operatively. Symptomatic hypo-calcemia was the primary outcome.
Results: 50 patients were included, 25 patients in each group. 4% of group A patients developed symptomatic hypocalcemia while 28% in group B patients developed post- operative symptomatic hypocalcemia which was statistically significant at P value of 0.021. Each group had one patient whom had developed persistent hypocalcemia with low para-thyroid hormone levels. There was no statistical significance regarding other complications between the 2 groups.
Conclusions: This trial demonstrated that the use of low dose dexamethasone post operatively following total thyroidectomy reduced the incidence of post operative symptomatic hypocalcemia with no effect on other complications.
Introduction
Thyroidectomy is performed for various thyroid diseases whether benign or malignant; this could be in the form of total or hemithyroidectomy. Despite of its importance, it holds a risk for serious complications, especial total thyroidectomy. These complications include Hypocalcemia (HC) and recurrent laryngeal nerve (RLN) palsy and voice dysfunction (1).
Hypocalcemia is a common complication in the immediate postoperative period, According to British Association of Endocrine and Thyroid Surgeons report, incidence of transient and permanent hypocalcemia after thyroidectomy is 27.4% and 12.1%, respectively (2). Hypocalcemia can lead to prolongation of the recovery period and hence hospital costs (3). Therefore, preventing these complications is a crucial issue during and after surgery.
Hypocalcemia could be due to surgical trauma whether it’s caused by parathyroid gland devascularization, congestion from venous drainage obstruction or excision of the gland.
Voice dysfunction may occur due to injury of the recurrent laryngeal nerve which could cause temporary or permanent vocal cord paralysis. Direct nerve injury is thought to be less common than indirect injury (4).
Other Risk factors that could aid in the occurrence of these complications are thyroid gland size, retrosternal extension, and recurrence (5).
Glucocorticoids are well known as effective anti-inflammatory agents and may be important biologic modifiers of perioperative inflammatory responses, leading to improvement of surgical outcomes and reduction of complications. Regarding the use of steroids in thyroid surgery, there is little and conflicting information in the literature (6,7).
Material and Method
Type of the study: Randomized Prospective study.
Required sample: 50 patients divided randomly into two groups equally. Simple random sampling technique was used (the lottery method). The sample size was decided upon by the community department at Ain Shams university
Study settings: The study took place at Ain Shams University hospital from October 2021 till October 2022, after approval of the ethical committee and obtaining an informed consent from all participants. We compared 2 groups of patients, one group recieved Dexamethasone (Group A) postoperatively following total thyroidectomy to a group without any perioperative glucocorticoid administration (Group B) following total thyroidectomy.
Dexamethasone was given in three doses. 1st dose was given 1 hour postoperatively (8 mg), then the following two days patients were given 4 mg of dexamethasone daily in the morning. Plasma levels of parathyroid hormone, total calcium, were measured pre- and postoperatively. Complications were recorded within a 30-day follow-up. Postoperative symptomatic hypocalcemia was the primary outcome.
Inclusion criteria:
1. Patients undergoing total thyroidectomy
2. Patients having benign lesion.
3. Patients with normal levels of parathyroid and calcium preoperatively.
Exclusion criteria:
1. Patients having recurrent thyroid enlargement.
2. Patients undergoing Hemithyroidectomy.
3. Patients with endocrinological diseases and chronic illnesses such as diabetes.
4. Retrosternal extension of the thyroid gland.
5. Malignant thyroid.
6. Patients with abnormal levels of calcium or parathyroid hormone pre-operatively.
7. Cases found in the final pathology to have the number of parathyroid glands remaining in situ (PGRIS) score zero as all parathyroid gland is in the final specimen.
All the patients in this study were under the care of one surgical team under supervision of consultant surgeon.
All patients were subjected to the following:
Preoperative:
- Clinical history:
- Personal history: including age, weight, occupation, and special habits of medical importance particularly smoking.
- History of present illness: mode of onset, duration of illness, any previous treatment for endocrinological abnormalities, hypocalcemia or history of previous surgeries in the neck.
- Past history of medical diseases: such as diabetes, drug allergy, previousblood transfusion, and previous operations.
- Clinical examination:
Clinical examination of the neck regarding the thyroid, trachea and draining lymph nodes.
3- Investigations:
- Routine preoperative investigations were done for all patients, including complete blood picture, coagulation profile, liver and kidney function tests, fasting blood sugar, chest x-ray. Special investigations were requested for patients with specific complaints as pulmonary function tests for patients with manifestations of chronic obstructive airway disease; ECG for patients above the age of 40.
- Specific preoperative investigations:
1. Thyroid ultrasound.
2. Thyroid Profile (free t3, free t4, TSH).
3. Fine Needle Biopsy.
4. Plasma levels of parathyroid hormone (PTH) (reference range, 15–65 pg/ml).
5. Plasma calcium level (reference range, 8.4–10.4 mg/dL).
6. Indirect laryngoscope for proper assessment of any vocal cord abnormalities.
Surgical intervention:
All operations were performed under general anesthesia with orotracheal intubation. Total thyroidectomy is performed in a standardized manner.
A transverse incision was made through the skin and underlying layers. Skin flaps were raised deep to the platysma and superficial to the sternohyoid muscle, at the level of the thyroid cartilage superiorly and sternal notches inferiorly.
The strap muscles (sternohyoid and sternothyroid) were lateralized by incising the median raphe until the thyroid capsule was identified. In certain cases where exposure needed to be improved such as in huge or retrosternal goiters, strap muscles was divided as high as possible to preserve its nerve supply.
Blunt dissection progressed laterally until the carotid sheath was identified. The lobe was gently displaced toward the midline, and the middle thyroid vein was handled whenever found. The superior thyroid vessels were identified and ligated as close to the gland to protect the superior laryngeal nerve. Along with this, the superior parathyroid gland was identified and preserve with its blood supply. The inferior para-thyroid gland was identified and preserved followed by identification and preservation of the recurrent laryngeal nerve. Then the inferior thyroid vessels were ligated. The lobe was then retracted medially and dissected off the trachea along with the division of berry’s ligament.
Hemostasis was done followed by insertion of suction drain and closure of layers.
Postoperative assessment:
Patients were assessed postoperatively regarding:
- Operative time.
- Hospital stay.
- Wound complications such as bleeding and infection.
- Hoarseness or change of voice.
- Patients were followed up and assessed for hypocalcemia (Symptomatic and biochemical) and for hypoparathyroidism.
- Hypocalcemia (HC) is defined as at least one serum calcium measurement below 8.0 mg/dL. Symptomatic hypocalcaemia (SHC) was defined as the presence of the following signs and symptoms associated with HC: numbness of the extremities, facial paraesthesia, muscular spasms, and Chvostek's or Trousseau's signs. Biochemical hypoparathyroidism (hPT) was defined as a low intact PTH level below the lower limit of the reference range, (reference range, 15–65 pg/ml) accompanied by HC.
Plasma levels of parathyroid hormone, total calcium, were measured at 6 hours post operatively, and the following 2 days in the morning.
Patients who showed hypocalcemia were given intravenous calcium gluconate IV slowly on normal saline (one ampoule every 8 hours) along with vitamin D. Calcium and parathyroid hormone levels were measured daily for these patients till improvement, followed up with oral calcium and vitamin D daily upon discharge.
Results
Table 1 shows the baseline characteristics (age, sex, comorbidities, diagnosis, preoperative Ca and PTH levels). There was no significant difference between the studied groups regarding these characteristics.
Table 1 - Baseline characteristics of the studied groups
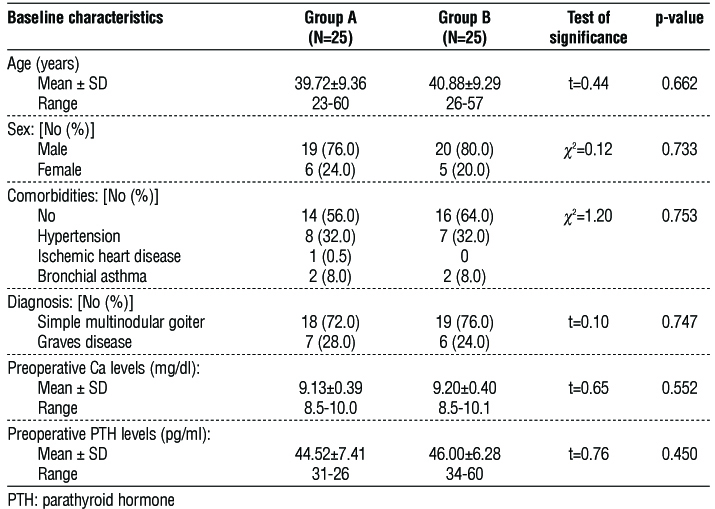
Table 2 represents post operative assessment data of the studied groups and it shows there was no significant difference between the studied groups regarding post-operative assessment data (operative time, duration of hospital stay, postoperative Ca and PTH levels, bleeding, wound infection, change of voice and PGRIS). Hypocalcemia (Ca level < 8 mg/dl) developed in 4% (1 case) of group A and B with low levels of PTH (PTH level < 15 pg/ml) presented in 4% (1 case) of group A and B. The postoperative ca and parathyroid hormone level were measured 6 hours post operatively.
Table 2 - Post-operative assessment data of the studied groups
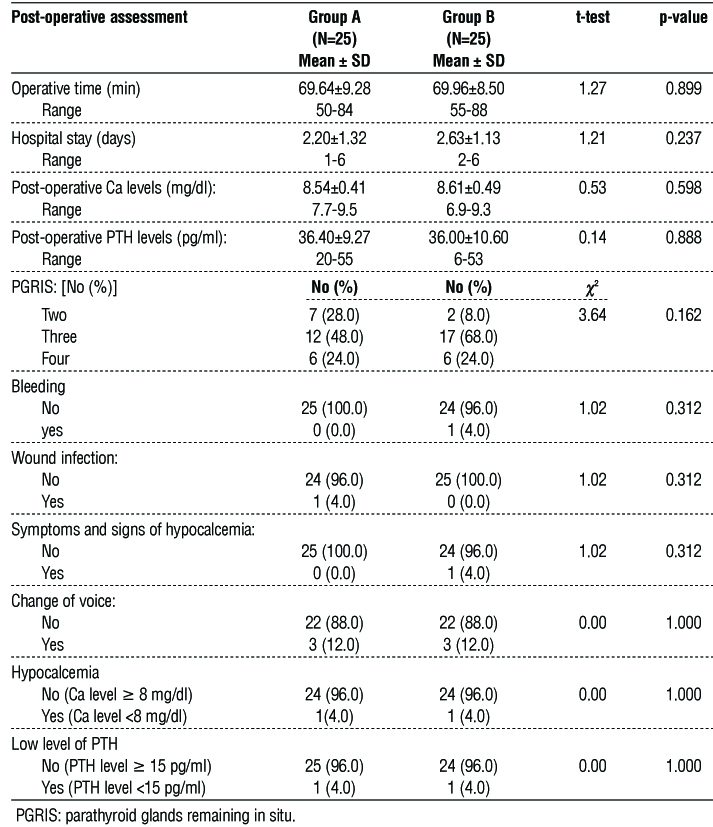
Table 3 shows the Post-operative Ca and PTH levels at different time of assessment.
At day 1: There was no significant difference between the studied groups regarding post-operative mean Ca and PTH levels. However, there were significantly higher percentage of hypocalcemic patients (had Ca level <8 mg/dl) and patients with symptoms and signs of hypocalcemia in group B than in group A patients (p=0.021 and 0.010; respectively). 7 patients in group B developed hypocalcemia while only one patient in group A, out of these patients low levels of parathyroid hormone were found in one patient in each group. Regarding the symptoms and signs of hypo-calcemia 8 patients in group B showed signs of hypo-calcemia indicating that one patient reported signs and symptoms without biochemical hypocalcemia i.e with normal calcium level.
Table 3 - Post-operative Ca and PTH levels at different time of assessment
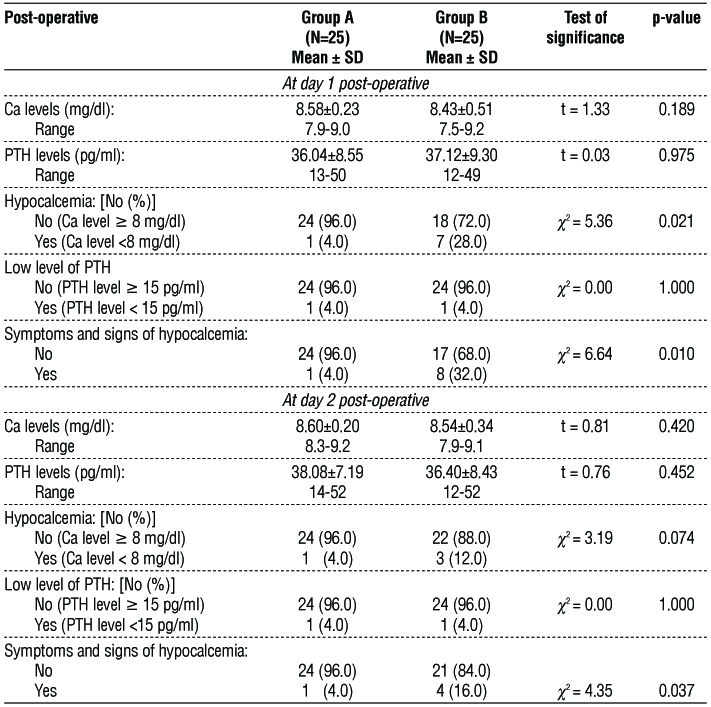
At day 2: There was no significant difference between the studied groups regarding post-operative mean Ca and PTH levels. However, there was a significant higher percentage of patients with symptoms and signs of hypocalcemia in group B than in group A patients (p=0.037). In group B 3 patients had hypo-calcemia since patients in day 1 with hypocalcemia were treated with IV calcium.
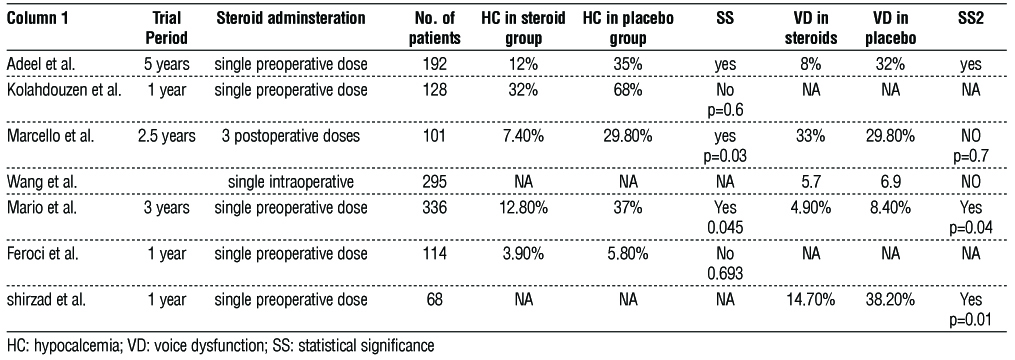
Table 4 - Comparison between different studies regarding hypocalcemia and voice dysfunction with and without steroids administration
Discussion
Post thyroidectomy hypocalcemia and voice dysfunction are well- known complications with short and long term effects; glucocorticoids has been suggested to have a physiological effect on hypo-calcemia and voice dysfunction. Although most of the studies reports the use of a single dose of gluco-corticoid, namely dexamethasone, preoperatively, we decided to use in the postoperative period. Dexamethasone is known for the immune modulating and anti-inflammatory response, our choice to use a glucocorticoid after surgery is supported by studies, which showed that glucocorticoids suppress immune response if administered when inflammation is not present but stimulate immunity during inflammatory response (7). Glucocorticoids work as physiological moderators of the iinflammation that occurs after surgery by decreasing the cellular immune response and the reaction to vasoconstrictors, which are primarily controlled by cytokine functions (6). Post thyroidectomy HC may be due to different causes, including para-thyroid removal and surgical trauma, an additional etiology includes an increase of calcitonin release due to thyroid gland manipulation during surgery other causes are postoperative hypocalcemia due to alkalosis which could result from hyperventilation from the pain and dilution hypocalcemia (8).
It is known that surgical trauma is an important cause of post-thyroidectomy HC, so reducing inflammation can minimize the occurrence of post operative hypocalcemia.
Regarding the baseline characteristics, the mean age in both groups is 39.72 group A and 40.88 group B, males are 76% in group A and 80% in group B while females were 24% in group A and 20% in group B. Co-morbidities were 44% in group A and 36% in group B, with no statistical significance.
In group A 72% had SMNG and 28% had graves, while 76% had SMNG and 24% had graves in group B. Both groups had normal pre operative ca and para-thyroid hormone levels.
There was no statistical significance in both groups regarding operative time and hospital stay.
Our results showed that 28 % of patients in group B developing post operative transient hypocalcemia, which is consistent with the British Association of Endocrine and Thyroid Surgeons report (2). But only 2 patients developed persistent postoperative hypo-calcemia at 4%, one patient in group with Pgris score 2 and one patient in group B with PGRIS 3 both patients had Graves.
Our data showed that hypocalcemia was significantly reduced in the group of pateints given dexamethasone postoperatively. In day 1, 7 patients in group B (28%) and 1 patient (4%) in group A developed hypocalcemia, out of these patients low levels of parathyroid hormone were found in one patient in each group. Regarding the symptoms and signs of hypocalcemia 8 patients in group B showed signs of hypocalcemia indicating that one patient reported signs and symptoms without biochemical hypocalcemia i.e with normal calcium level. there were significantly higher percentage of hypo-calcemic patients (had Ca level <8 mg/dl) and patients with symptoms and signs of hypocalcemia in group B than in group A patients with statistical significance (p=0.021 and 0.010; respectively).
At day 2 there was no increase in the number of patients developing hypocalcemia in group A, yet there was a significant higher percentage of patients with symptoms and signs of hypocalcemia in group B than in group A patients with statistical significance of (p=0.037). In group B, 3 patients had hypocalcemia since patients in day 1 with hypocalcemia (7 patients) in were treated with IV calcium.
M picchio et al used betamethasone post operatively in 3 daily doses with statistically significant reduction in biochemical and symptomatic hypo-calcemia. M picchio et al, discussed the PGRIS score as an independent factor for the occurrence of post operative hypocalcemia, reporting that the removal of at least 2 parathyroid glands is a significant risk factor for SHC occurrence (4). This was not shown in our statistics, individuals in group B with SHC all have PGRIS score above 2, yet in group A the individual with post operative SCH had a PGRIS score of 2. Ottavio C. identified the extend of surgery to central or lateral lymph node dissection to be the only statistically significant variable in transient post operative hypoparathyroidism which may lead to unplanned parathyroidectomy or accidental devascularization of the parathyroid gland (9).
There isn’t enough evidence in the literature about the use of glucocorticoids postoperatively to prevent hypocalcemia following total thyroidectomy, most available literature discusses the use of pre operative glucocorticoids. A Chinese retrospective study on patients undergoing thyroidectomy for papillary carcinoma showed that in the group of patients treated with intraoperative plus postoperative glucocorticoids, the incidence of hypo para thyroidism was reduced after surgery (10). A Dhahri, Mario S., used single preoperative dose of dexamesathone which showed effectiveness in reducing transient postoperative hypocalcemia and postthyroidectomy voice dysfunction (11,12).
Figure 1 (a,b) - Identification and preservation of recurrent laryngeal nerve and parathyroid gland during thyroidectomy

Also M Kolahdouzan et al , Abdellatif et al results showed statistically significant effect in transient post operative hypocalcemia (6,13). However, Feroci et al did not find a significant difference in symptomatic or asymptomatic hypocalcemia with perioperative dexamethasone use (14).
Recurrent laryngeal nerve palsy is an important cause for dysphonia and voice dysfunction Following thyroidectomy, voice impairment well-known cause of dysphonia is RLN palsy. Transection of the RLN is uncommon, nevertheless. Its functional damage is primarily caused by surgical trauma associated to the intraoperative handling of the RLN (14). Another possible reason for high-pitched voice could be damage to the external laryngeal nerve. These findings led to the suggestion that glucocorticoids be used during surgery in order to lessen the inflammatory response and maintain the function of the external and recurrent laryngeal nerves. Regarding alteration of voice, neither our investigation nor that of Marcello et al. found any statistically significant results (4). Nonetheless, following thyroidectomy, Abdel Latif et al. and Worni et al. results demonstrated an improvement in post-operative voice quality function (13,15). In Shirzad N. study, 68 patients were included and found that the use of steroids pre-operatively was statistically significant in lowering the vis score in day 1, yet no statistical significance after a week (16). Ling-Feng W., used single intra-operative dose of corticosteroid in a study including 295 patients which showed no statistical significance in prevention of permanent or temporary recurrent laryngeal nerve but reduced the recovery time in temporary nerve palsy (17). A meta-analysis by cheng S. failed to demonstrate the advantage of using dexamesathone perioperatively in improving the immediate voice outcomes, this could be due to the use of different assessment tools for voice quality (18). Mario S., concluded the use of single dose of dexamethasone pre-operatively significantly reduced the rate of post-operative temporary recurrent laryngeal nerve palsy, in a study that included 328 patients (12).
Regarding bleeding, wound infection there was no statistical significance between both groups which indicates that glucocorticoids had no significant side effect of immunosuppression and affection of wound healing.
Conclusion
This trial demonstrated that the use of low dose dexamethasone post operatively following total thyroidectomy reduced the incidence of post operative symptomatic hypocalcemia with no effect on other complications . 3 out of 5 studies that used dexamethasone showed statistical significance in prevention of hypocalcemia following total thyroidectomy, while the remaining 2 studies showed no statistical significance. Regarding voice dysfunction 3 out of 5 studies shows statistical significance in prevention of voice dysfunction and transient recurrent laryngeal nerve affection.
Limitations
Initially, there was no long-term follow-up, although comparable trials also lacked one. Secondly, there wasn't a big enough sample size. Furthermore, there was no objective way to quantify the postoperative symptomatic outcomes; instead, the patients reported them all subjectively. It has been demonstrated that indocyanine green fluorescence angiography is a trustworthy intraoperative adjunct for evaluating the perfusion and ensuing function of the remaining parathyroid glands. It is recommended to utilize this technique to evaluate the effectiveness of glucocorticoids in minimizing postoperative functional impairment of the parathyroid glands. Further research on the PGRIS, the impact of the amount of residual parathyroid glands on function, and post-operative hypoparathyroidism and hypocalcemia are also necessary.
Conflicts of interest
There is no conflict of interest.
Ethics of approval
The research was approved by the ethical committee in Ain Shams University.
References
1.Sitges SA, Gallego OL, Fontané J, Trillo L, Lorente PL, Sancho J. Contralateral surgery in patients scheduled for total thyroidectomy with initial loss or absence of signal during neural monitoring. Br J Surg. 2019;106(4):404-411.
2.Chadwick D, Kinsman R, Walton P, Systems DC. The British Association of Endocrine and Thyroid Surgeon Fourth National Audit. Henley-on-Thames: Dendrite Clinical Systems Ltd; 2012.
3.Bhattacharyya N, Fried MP. Assessment of the morbidity and complications of total thyroidectomy. Arch Otolaryngol Head Neck Surg 2002;128:389-92.
4.Marcello P, Annalisa RDF, Martina S, Simone O, Riccardo B, Giuliano G, et.al Betamethasone to Prevent Symptomatic Hypocalcaemia and Other Complications after Total Thyroidectomy: a Case-control Study. J Endocr Surg. 2021;21(3):61-69.
5. Sincar S, Akkuzu E, Kalkan G. Hopeful waiting before disappointment: vocal cord paralysis after thyroidectomy. Indian J Surg. 2020;82:693-694.
6. Kolahdouzan M, Iraj B, Eslamian M, Harandizadeh M, Meamar R. Preventive effect of dexamethasone therapy on the transient hypoparathyroidism through total thyroidectomy. Iran J Otorhinolaryngol 2019;31:73-80.
7. Lepelletier Y, Zollinger R, Ghirelli C, Raynaud F, Hadj-Slimane R, Cappuccio A, et al. Toll-like receptor control of glucocorticoid-induced apoptosis in human plasmacytoid predendritic cells (pDCs). Blood 2010;116:3389-97.
8. Del Rio P, Rossini M, Montana CM, Viani L, Pedrazzi G, Loderer T, et al. Postoperative hypocalcemia: analysis of factors influencing early hypocalcemia development following thyroid surgery. BMC Surg 2019;18:25.
9. Cavicchi O, Piccin O, Caliceti U, De Cataldis A, Pasquali R, Ceroni AR. Transient hypoparathyroidism following thyroidectomy: a prospective study and multivariate analysis of 604 consecutive patients. Otolaryngology-Head and Neck Surgery. 2007;137(4):654–8.
10. Li JH, Chen XH. Effect of perioperative application of glucocorticoid on postoperative hypoparathyroidism and hypocalcemia in patients with total thyroidectomy plus central compartment dissection. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2020;55:249-53.
11. Adeel AD, Raheel A, Ahsan R, Dujanah B, Sheikh HA, Samar G, et.al. Use of Prophylactic Steroids to Prevent Hypocalcemia and Voice Dysfunction in Patients Undergoing Thyroidectomy. JAMA Otolaryngol Head Neck Surg. 2021;147(10):1–5.
12. Schietroma M, Cecilia EM, Carlei F, Sista F, De Santis G, Lancione L, Amicucci G Dexamethasone for the prevention of recurrent laryngeal nerve palsy and other complications after thyroid surgery: a randomized double-blind placebo-controlled trial. JAMA Otolaryngol Head Neck Surg 2013;139:471–478.
13. Abdel LAM, Mohamed TY, Lotfy AE, Ahmed AHM. Dexamethazone prophylaxis before near total thyroidectomy to reduce vocal dysfunction: a randomized clinical trial. Egypt J Hosp Med. 2020; 81(4):1789-1795.
14. Feroci F, Rettori M, Borrelli A, Lenzi E, Ottaviano A, Scatizzi M. Dexamethasone prophylaxis before thyroidectomy to reduce postoperative nausea, pain, and vocal dysfunction: a randomized clinical controlled trial. Head Neck. 2011;33(6):840-846.
15. Mathias W, Hans HS, Eberhard S, Roman I, Matthia H, Stephan AV, et.al. Randomized controlled trial on single dose steroid before thyroidectomy for benign disease to improve postoperative nausea, pain, and vocal function. Ann Surg. 2008;248(6):1060-1066.
16. Nasiri S, Shafag S, Khorgami Z, Sodagari N, Aminian A, Hedayat A. Does corticosteroid have any beneficial effect on voice change after thyroidectomy? The American Surgeon. 2013;79(12): 1258–62.
17. Wang LF, Lee KW, Kuo WR, Wu CW, Lu SP, Chiang FY The efficacy of intraoperative corticosteroids in recurrent laryngeal nerve palsy after thyroid surgery. World J Surg 2006;y30:299–303.
18. Cheng S-P, Liu T-P, Yang P-S, Lee K-S, Liu C-L. Effect of perioperative dexamethasone on subjective voice quality after thyroidectomy: a meta-analysis and systematic review. Langenbeck's Archives of Surgery. 2015;400(8):929–36.
Full Text Sources:
Abstract:
Views: 5451

For Authors
Journal Subscriptions

Mar 2026
Supplements
Instructions for authors
Online submission
Contact
e-ISSN: 2601 - 1700 (online)
ISSN-L: 2559 - 723X
Journal Abbreviation: Surg. Gastroenterol. Oncol.
Surgery, Gastroenterology and Oncology (SGO) is indexed in:
- SCOPUS
- EBSCO
- DOI/Crossref
- Google Scholar
- SCImago
- Harvard Library
- Open Academic Journals Index (OAJI)
Surgery, Gastroenterology and Oncology (SGO) is an open-access, peer-reviewed online journal published by Celsius Publishing House. The journal allows readers to read, download, copy, distribute, print, search, or link to the full text of its articles.
Time to first editorial decision: 25 days
Rejection rate: 61%
CiteScore: 0.2

Meetings and Courses in 2025
Meetings and Courses in 2024
Meetings and Courses in 2023
Meetings and Courses in 2022
Meetings and Courses in 2021
Meetings and Courses in 2020
Meetings and Courses in 2019
Verona expert meeting 2019

Surgery, Gastroenterology and Oncology applies the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits readers to copy and redistribute the material in any medium or format, remix, adapt, build upon the published works non-commercially, and license the derivative works on different terms, provided the original material is properly cited and the use is non-commercial. Please see: https://creativecommons.org/licenses/by-nc/4.0/
Publisher’s Note:
The opinions, statements, and data contained in article are solely those of the authors and not of Surgery, Gastroenterology and Oncology journal or the editors. Publisher and the editors disclaim responsibility for any damage resulting from any ideas, instructions, methods, or products referred to in the content.